Ocular Surface and Pre-Operative Cataract Surgery: Much Beyond Artificial Tears Ocular Surface and Preoperative Cataract Surgery: Far Beyond Artificial Tears
Ocular Surface and Pre-Operative Cataract Surgery: Much Beyond Artificial Tears
Ocular Surface and Preoperative Cataract Surgery: Far Beyond Artificial Tears
Raphael Barcelos *1, Monica Alves 2, Andreo Garcia Morante Parra 3, Talita Pires da Fontoura 4, Letícia Pitta Manhães 5, Daniela Trovão de Figueirôa 6, Gabriel Gorgone Giordano7,
Mauro Silveira de Queiroz Campos 8
1. Department of Ophthalmology, Federal University of São Paulo - UNIFESP, São Paulo, Brazil.
2. Department of Ophthalmology, State University of Campinas - UNICAMP, Campinas, Brazil.
3. Paraná Eye Hospital - HOP, Curitiba, Brazil.
4. Department of Ophthalmology, Ophthalmological Hospital -BOS, Sorocaba, Brazil.
5. Department of Ophthalmology, University of Sao Paulo - USP, São Paulo, Brazil.
6. Suel Abumjanra Institute - ISA, São Paulo, Brazil.
7. Department of Ophthalmology, State University of Campinas - UNICAMP, Campinas, Brazil.
*Correspondence to: Raphael Barcelos, Department of Ophthalmology, Federal University of São Paulo -UNIFESP, São Paulo, Brazil.
Copyright
© 2023 Raphael Barcelos. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 October 2023
Published: 20 November 2023
DOI:https://doi.org/10.5281/zenodo.10164463
Summary
Over time, the evolution of cataract surgery and optical biometrics has led to surgeons have on hand instruments capable of promoting the elimination of ametropia residuals and minimize optical aberrations. However, the expected results in surgery cataracts depend mainly on good surgical planning, involving aspects such as the choice of intraocular lenses and precise routines to identify pathologies that may affect the ocular surface. In this context, this study aimed to carry out a review broad bibliographical, through exploratory methodology, where databases were used digital with selected works by authors relevant to the topic. It was concluded that the evaluation of homeostasis or identification of changes in the ocular surface before performing the biometry in the preoperative period of cataract surgery is of fundamental importance for the understanding the impact of these changes, allowing early identification and the treatment of ocular surface diseases such as dry eye in its different degrees of classification, contributing to the best choice of intraocular lenses and lower chances of refractive errors and residual ametropia.
Keywords: ocular surface assessment; intraocular lenses; cataract surgery; dry eye disease
Ocular Surface and Pre-Operative Cataract Surgery: Much Beyond Artificial Tears Ocular Surface and Preoperative Cataract Surgery: Far Beyond Artificial Tears
Introduction/Justification of the Review
The choice of intraocular lens for cataract surgery is made by measuring the anteroposterior axial length and the correct measurement of the corneal curvature using biometric formulas validated for the characteristics of each eye.
Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of ocular discomfort, visual disturbances and tear film instability, with possible damage to the ocular surface being accompanied by an increase in film osmolarity lacrimal and inflammation of the ocular surface.
The tear film is directly related to the maintenance of the regularity pattern of corneal surface. Changes in the tear film, whether qualitative or quantitative promote direct interference in the quality of image capture and, therefore, As a result, we may have a topographic image that does not correspond to reality. [1]
The expected results in cataract surgery depend not only on one act well-executed surgery, with an appropriate and accurate technique, and it is also important to your surgical planning. Currently, where intraocular lenses are implanted toric, bifocais, trifocais, extended depth of focus (EDOF) and pseudo-accommodative there is a greater demand for refractive results by patients and the surgeon must not fail to consider and give due importance to the stability of the tear film and a surface healthy eye. The evolution of cataract surgery and Optical Biometry has meant that surgeons have in hand instruments capable of not only promoting the elimination of residual ametropia, but also to minimize optical aberrations. Cataract surgeons need to employ its routine methods to identify pathologies that may affect the ocular surface. To the significant irregularities of the ocular surface must be corrected, so that measurements keratometric measurements are more accurate and the best intraocular lens is chosen.
Search Methodology And Literature Review
Search Methodology
The search methodology included digital databases such as Medline/Pubmed and Scielo. The accesses were carried out from May 27th to June 22nd. In the database Medline/Pubmed, the words used in the search were: “ocular surface and eye biometry”.
In addition to the databases, TFOS/DEWS II - Definition and classification: Jennifer P. Craig, MCOptom, PhD1, Kelly K. Nichols, OD, PhD1, Esen K. Akpek, MD, Barbara Caffery, OD, PhD, Harminder S. Dua, MD, PhD, Choun-Ki Joo, MD, PhD, Zuguo Liu, MD, PhD, J. Daniel Nelson, MD, Jason J. Nichols, OD, PhD, Kazuo Tsubota, MD, PhD, Fiona Stapleton,
MCOptom, PhD, 2017, the book on External Eye and Cornea Diseases/Brazilian Council of Ophthalmology; coordinator: Milton Ruiz Alves; editors Ana Luisa Hoffing Lima, Maria Cristina Nishiwaki Dantas, Milton Ruiz Alves. – 4th ed. Rio de Janeiro; Cultura Medica, 2016, the book Wavefront and Topography, Tomography and Biomechanics of the Cornea: propaedeutics complementary study in refractive surgery/Renato Ambrósio Jr. [et al.], - 2nd ed., the book “Catarata.
Faria, Marco Antônio Rey”, “and the book Polisuk, Paulo - Topography of the Cornea: atlas clinician/Paulo Polisuk. – 4. ed - Rio de Janeiro: Cultura Médica, 2015 were consulted.
Literature Review
Computerized corneal topographers using placido rings are based on the principle of reflection of the rings by the cornea. The anterior surface works like a mirror convex that reflects light, which is analyzed and captured by the surveyor to create the map topographic view of its anterior curvature. The tear film is directly related to the maintenance of the regularity pattern of the corneal surface. Changes in the tear film, whether
Qualitative or quantitative will directly interfere with the quality of image capture and consequently we can have a topographic image that does not correspond to reality. [1]
The use of lubricants can cause an increase in the tear film in the lower region of the cornea, which can lead to the demonstration of a strong increase in inferior corneal curvature. Therefore, if using lubricants, even those without preservatives, care must be taken and ask the patient to blink several times to spread the lubricant evenly on the cornea at the time of the examination. In addition, the examination must be carried out by least 1 minute after instilling the eye drops, so that the tear lake formed inferiorly has already has been drained. Two The use of the placido disk aims to promote greater accuracy in determination of the central corneal power, as the placido topography is still the best and most direct way to assess the curvature of the anterior surface of the cornea.1 Unfortunately, such equipment does not evaluate the posterior surface of the cornea and has certain limitations to analysis of data from the corneal periphery, in addition to topography being a very examining examination dependent.[1]
From the 90s onwards, segment tomographs began to be developed anterior segment, which enabled the analysis of keratometry and more variables of the anterior segment. Initially, the combination of placido technology with slit scanning was used. vertical lights, to triangulate the position of thousands of points on the anterior and posterior surface of the cornea.[1]
Systems that do not have placido and use only Scheimpflug images calculate the anterior curvature indirectly through mathematical algorithms and elevation analysis. Elevation is the difference between the location of the spatial point located by the system and a ideal reference surface. Elevation maps complement map information of curvature, but they do not replace it.[1]
The most used reference surface is the sphere that best fits the values found (BFS, from best fit sphere). In addition to BFS, there are maps that compare a sphere incomplete, which exclude data from a small zone whose center is the most elevated (Belin/ Ambrosio Enhanced Display-BAD), a symmetrical asphere (BFA, best fit asphere) from one asfera torica (BFTA, de best fit toric asphere).[1]
BFTA maps from CT scanners are enabling a better understanding of asymmetries, irregularities and roughness of the corneal surfaces that cause aberrations high-order optics.[1]
Analysis of the elevation on corneal tomography made it possible to calculate the curvature posterior corneal and total dioptric power of virgin corneas or those submitted to surgery refractive.[1]
The Scheimpflug system enables segmental analysis of the eye in sagittal planes, from the anterior surface of the cornea to the posterior surface of the lens, which makes it possible to obtain measurements and real distances between the structures and quantify the opacities in the media carried out.[1]
There are several devices that use this system on the market. It is currently not known amount of optical aberrations that an eye can tolerate without presenting symptoms, but this could explain causes of dissatisfaction in patients with toric or multifocal IOLs diffractive images and understand the real role of the cornea in the vision of these patients.[1]
The analysis of Zernike polynomials on corneal tomography in the preoperative period assist with the choice of intraocular lenses ensuring greater safety in the implantation of Premium IOLs. This is due because surgeons assume that optical aberrations from the aqueous humor, posterior capsule, and vitreous humor are insignificant and those of the IOLs and cornea can be measured with greater accuracy. [1]
Corneal tomographs highlight the main high-order aberrations, which can without shown in both microns and diopters, second order aberrations such as defocus. Astigmatism and third order, both vertical and horizontal or oblique, as well as trefoil and eat. We also have fourth-order astigmatism, such as tetraleaf, fourth-order astigmatism. order and spherical aberrations at the center. State-of-the-art CT scanners can show us additionally aberrations of: 5th; 6th; 7th; and 8th orders and the total RMS (of total root mean square).[1]
This RMS is the square root of the variance of the sum of the squares of all the coefficients of Zernike. It works as if it were a general and non-specific representation of the aberrations of the cornea. [1]
Dry eye disease is probably the most common etiology for changes in ocular surface and follows a chronological line somewhat similar to the opacification of the crystalline. Other causes of ocular surface changes include: blepharitis; dystrophies of epithelium and basement membrane; dermatochalasis; Loose eyelid syndrome; conjunctivitis allergic; Salzmann Nodular Degeneration; and bullous keratopathy. [4]
The main signs and symptoms of dry eye are: burning eyes; ocular hyperemia; tearing; burning eyes; visual blurring; foreign body sensation; irritation eyepiece; and photophobia. Dry eye is found, in practice, in more than half of patients undergoing cataract surgery4, being Meibomius Gland Dysfunction (MGD) diagnosed in the majority of patients with dry eye disease and in more than half of candidates for refractive surgery.[5]
The majority of patients undergoing cataract surgery can be asymptomatic for dry eye, but may already present changes in the osmolarity of the tear film. It is of great importance to identify changes in the ocular surface even preoperatively, as surgery can intensify or exacerbate film dysfunction subclinical lacrimal tear, generating discomfort and symptoms for the patient. Many patients do not report symptoms until they are questioned about their presence.
In addition to inaccurate preoperative calculations, untreated Dry Eye Disease that persists can generate vision instability, fluctuation and fatigue, generating dissatisfaction for the patient and surgeon in the postoperative period. Surgeries in patients with ocular surface disease are not treated can also generate more propensity for infectious processes.[6]
Data from the European Society of Cataract and Refractive Surgery Clinical Survey (ESCRS) 2018, on ocular surface diseases showed that less than half of the doctors are examining the ocular surface before cataract surgery in all its patients and about 20% are examining only when the patient presents complaints or symptoms of dry eye.[7] This fact occurs even with 90% of those interviewed agreeing that Mild to moderate tear film dysfunction already significantly affects preoperative keratometry. surgery and IOL calculation. [7]
One factor to be taken into account is the fact that the patient receives a diagnosis of tear film dysfunction and/or dry eye preoperatively in a more receptive manner than after the procedure performed.
The risk of Dry Eye Disease increases postoperatively due to various etiologies, which include pupil dilation, exposure to operating microscope light, type and duration anesthetic, antisepsis procedures such as the use of povidone-iodine, location of incisions, denervation of corneal nerves by incisions in the cornea, corneal epithelial damage, elevation of inflammatory markers with ocular surface damage and loss of cell density goblets. Suction procedures such as those used in the femtolaser can increase the chance of dry eye disease. [8]
Phacoemulsification modifies the function of the Meibomius glands, which can generate exacerbation of MGD in the postoperative period. Postoperative abnormalities often remain for 3 months, but can remain for up to 1 year after surgery.[8]
In a study carried out by Gibbons et al. in 2017, at the Bascom Palmer Eye Institute, It was shown that in patients undergoing cataract surgery, 35% of patient dissatisfaction patients were related to dry eye after surgery.[9]
The compromised ocular surface in addition to affecting the pre-operative calculation of the Lens Intraocular, may affect axis and magnitude estimates of toric IOLs and promote greater surgical difficulty.
There is a certain gap in the literature regarding work on management and impacts of the eye dry in the preoperative period of intraocular surgeries, with many studies found related to dry eye in the postoperative period of cataract surgery and especially surgery refractive.
Significant irregularities of the ocular surface must be corrected, so that keratometric measurements are more precise and the Intraocular Lens is chosen in the best way possible. possible way. 10 Conjunctiva and all layers of the cornea should be evaluated for pathologies that may change the mean keratometry or show optical aberrations.
The Duke University study, carried out in 2018, emphasizes and supports the concept of carrying out preoperative screening for ocular surface dysfunction, without taking into account counts symptoms as an important factor, as many patients with potentially significant differences in ocular surface dysfunction are asymptomatic.[11]
In this study, 80% of patients undergoing cataract evaluation had objective signs of ocular surface dysfunction preoperatively and 57% of patients did not had a previous diagnosis of ocular surface disease, which suggests that ocular surface dysfunctions tear film have a high prevalence and are underdiagnosed in patients when evaluating cataract surgery.[11]
Dry eye was first characterized in 1995, this being the first attempt formal way of defining and classifying dry eye disease. When was Tear Film and Ocular Surface Society (TFOS), by 1995 there were about 5,000 citations of eye work dry. In 2005 there were already more than 50,000 citations. In 2007, the first Report was published of the TFOS International Dry Eye Workshop, which became widely known as TFOS DEWS, where dry eye was more formally divided into evaporative dry eye and watery.[5]
In 2017, a workshop, held through a 2-year effort by 12 subcommittees, composed of 150 experts from 23 countries, led to the publication of the extremely important report TFOS International Dry Eye Workshop II (TFOS DEWS II).[5]
The President, Vice President and Organizer of TFOS DEWS II developed the qualifications for participation and responsibility of all Workshop members. O
Steering Committee appointed chairs for each of the 12 individual subcommittees. Furthermore, 139 experts in their respective fields were chosen, based on their global representation on the subject, its clinical perspectives, research perspectives and multidisciplinary patients, from a much larger group of individuals who have been appointed and/or expressed written interest in participating in TFOS DEWS II.[5]
The need for DEWS II was due to the large number of works produced on dry eye since the 2007 Workshop. The Steering Committee was formed by 25 members and was responsible for strategies, tactics, structures, communication methods, schedule, assessment of policies of interest and development of work objectives that would be used in the study. This committee selected subcommittee chairs and members, proposed guidelines for determining acceptable levels of evidence and documentation methods for support this evidence and considered the most appropriate journal for which publication would be targeted.[5]
DEWS II aimed to update the definition, classification and diagnosis of Dry Eye Disease, in addition to carefully evaluating its etiologies, mechanisms, distribution, impacts, its approach, management and therapy.[5]
The TFOS/Dry Eye Workshop II redefined the classification of dry eye as a multifactorial disease of the tears and ocular surface, which results in symptoms of discomfort, visual disturbances and tear film instability, with possible damage to the ocular surface. AND accompanied by increased tear film osmolarity and surface inflammation eyepiece. This was the first time that dry eye was identified as a disease that has many associated causes, and which results in signs and symptoms, in association with hyperosmolarity of the tear film and inflammation of its ocular surface.[5]
TFOS DEWS II defines:
“Dry eye is a multifactorial disease of the ocular surface characterized by a loss of tear film homeostasis and accompanied by ocular symptoms, in which the instability and hyperosmolarity of the tear film, inflammation and damage of the ocular surface and neurosensory abnormalities play etiological roles.”[5]
The addition of the term “loss of homeostasis” clarified, based on recent evidence peer-reviewed studies that tear film hyperosmolarity and surface inflammation ocular have causal etiological roles associated with neurosensory abnormalities.[5]
Hyperosmolar stress is believed to be the main factor responsible for increasing in the epithelial cells of the ocular surface the release of inflammatory factors and proteases, which will give rise to the vicious circle of dry eye and this direct or diffuse hyperosmolarity leads to loss of epithelial and goblet cells. Change in cell hyperosmolarity ocular surface epithelium triggers an inflammatory cascade with cellular signaling in response to stress (MAPkinases - Mitogen-Activated Protein Kinase) and NFkB (Kappa Light Chain Nu-clear Factor, enhancer of activated B cells) and which culminate in increase in inflammatory cells (Interleukin-1 ÿ, Interleukin-ÿ), TNF (Necrosis Factor tumor) and extracellular matrix metalloproteinases (MMP-9). MMP-9 is a protease central action to hyperosmolar stress, which has already been suggested to be measured in tears as dry eye meter and its action leads to the breakdown of the epithelial barrier, which causes occurrence of APCs and NKs, which are components of the innate immune system and which produce tissue damage. APCs migrate to lymph nodes, where they contribute to activation of CD4 T cells, which secrete interferon gamma and IL-17 and are recruited to ocular surface generating more damage to the epithelial barrier, decreasing cell density caliciformes.[4,5]
These inflammatory mediators also decrease glycocalyx expression, component of the outer surface of the epithelium that interacts with the muco-aqueous layers of the tear film and plays an important role in ocular lubrication. It is believed that this change in the glycocalyx expression occurs associated with tear film instability evidenced by Reduced BUT and would justify the punctate keratopathy that occurs in dry eye.[4,5]
The main risk factors for dry eye are: use of topical and systemic medications; previous intraocular surgery or non-surgical procedure; use of botulinum toxin; dehydration; enlarged palpebral fissure due to anomalous anatomy or surgery plastic; changes in blinking rhythm; users of electronic devices; heat exposure; cold; low humidity; air pollution; excessive evaporation; DGM; secondary to dermatoses systemic; sex; ethnicity and age; vitamin A deficiency; allergies and use of eye drops; especially antiglaucoma eye drops. The prevalence of dry eye disease, with and without symptoms, ranges from 5 to 50%. Its prevalence based on signs alone is even more variable, reaching 75% in some cases. populations. This is due to the great variability of methodology used in the studies and the inclusion criteria used in them.
For example, few studies have been carried out on young populations, despite what has been studied so far points to a lower prevalence in them.[5]
It is more common in women and patients of Asian origin. The preference for Asians appears to be a risk factor, but there is no established base reason. It is known also, that the prevalence only becomes higher in women with increasing age and that this occurs due to genetic and hormonal factors, as androgens play an important role in regulation of the ocular surface and ocular annexes, and its deficiency can cause dysfunction of the lacrimal glands and also the meibomian glands, thus contributing for both the aqueous and evaporative deficiency components.[5]
Dry eye can be divided into 2 groups according to its pathophysiology. The eye dryness may be due to aqueous deficiency of the tear film (DAFL) and excessive evaporation, which, for the most part, are associated with meibomian gland dysfunction.
Regardless of the type of dry eye, the vicious circle of tears ends up heading towards a common denominator which is tear film instability, with the initial cause becoming often indistinguishable. [4.5]
Aqueous tear film deficiency can also be subdivided into Sjögren's and Non-Sjögren's Syndrome . Sjögren's form may still be subdivided into primary Sjögren's or secondary Sjögren's. [4]
In the primary Sjögren's form, the patient has only Sjögren's and in the secondary form, association with some systemic disease, the most common being Rheumatoid Arthritis, but also having a relevant association with Systemic Lupus Erythematosus, Polyarteritis Nodosa, Wegener's Granulomatosis and Systemic Sclerosis. The main symptoms of Sjögren 's syndrome are: dry eye; and xerostomia. Its diagnosis is made with a marker dry eye or dry mouth, such as sialometry, a marker of the immunological basis of the disease (Anti-Ro and Anti-La and salivary gland biopsy). In Sjögren's Syndrome, imaging tests such as USG and MRI of glands can also help with the diagnosis. [4.5]
In the Non-Sjögen form, tear deficiency may occur due to insufficient production tear, obstruction of the lacrimal glands, neurotrophic keratitis with reflex block sensory production, Diabetes, chemical injury or use of systemic medications. Also may occur due to congenital alacrimia (rare form), lacrimal gland ablation and dry eye associated with age, which is the main non- Sjögren's cause and is characterized by decreased drive sensorial. [4,5]
Dry eye is a disease that can be accompanied by symptoms of anxiety and depression, as patients are accompanied by signs and symptoms that change their routine, style and quality of life and which are little understood even by the ophthalmologist himself.
The tear film is the first and most important refractive interface of the ocular surface, as this is where the greatest variation in the refractive index occurs: air = 1, tears = 1.34, cornea = 1.38). Its irregularity can generate inaccurate keratometric measurements in the preoperative period, in addition to corneal optical aberrations.
The tear film is divided into 3 layers: lipid; watery; and mucosa. The dysfunctions of Meibomius glands such as meibomitis cause changes in the lipid layer, causing greater evaporation and potentially generating evaporative dry eye. There is an association of blepharitis, especially posterior ones, with changes in the meibomian glands, due to large release of exotoxins that generate inflammation of the ocular surface and irritation around of the meibomian glands.
There are several studies that report an association of neurosensory factors associated with dry eye disease, and which suggest that there is underreporting of discomfort by these patients, as this group has greater pain tolerance.11 This reinforces the theory that the majority of dry eye sufferers are asymptomatic.
Dry eye is characterized by hyperosmolarity and this hyperosmolarity is the main responsible for the mechanism for inducing inflammation of the ocular surface, presenting, therefore, hyperosmolarity correlates with the severity of tear film dysfunction. In eyes with a healthy tear film, a minimum power difference of 0.1 may occur D between blinks. In eyes with unstable tear film, a higher variation may occur at 1.0 D, which can generate an error of the same magnitude when calculating the IOL power.[12]
Tear film dysfunction also affects tear film accuracy and reproducibility. keratometry. According to the work “Optimization of the ocular surface for biometric measurements accurate”, presented at ESCRS 2019, in Paris, by Cochener-Lamard the eyes with hyperosmolarity are associated with large differences in K cylinder measurements (17% have difference of 1.0 D), and changes in IOL power, (10% had changes in K greater than 0.5 D ).12 These changes in K can have a significant impact on the actual diagnosis of the astigmatism and its necessary treatment, especially in multifocal and toric lenses.
Dry eye treatment should be performed before surgery, ideally before surgery. biometry, and can be performed clinically or surgically, in very severe cases. O
Treatment must be individualized and is staggered. In the clinical form, it should include education of the patient in relation to their pathology, identification and treatment of environmental conditions, behavioral conditions and conditions such as the use of contact lenses, guidance on the importance of flashing, guidance on using electronic devices more appropriately (placing the ceiling of the computer at a lower level to reduce the palpebral fissure and reduce evaporation lacrimal), avoid trigger factors such as dust, air conditioning, cigarette smoke and advise adequate oral hydration. Patients with blepharitis should be advised to practice correct eyelash hygiene.
Commercial substances or those manipulated with tea tree oil are more effective than use of children's shampoo. The use of artificial tear substitutes is recommended, with preference for preservative-free lubricants, which is the first line treatment. Night gels can be indicated mainly in those patients with complaints in the morning, as patients stop blinking at night during REM sleep. Patients with lagophthalmos can require night occluders.
Oral supplementation with polyunsaturated essential fatty acids, such as omega 3 (richly present in linseed oil and fish oil) help combat inflammatory process proving to be effective in practice, as they act by reducing markers inflammatory processes, but their process has not yet been completely elucidated with results varied as in several studies reported in DEWS. It is known that they have great potential of help in treatment, but it is not the main determinant in treatment as there is a individual variation in the metabolization of these fatty acids and despite recent developments, poorly tolerated by many patients. It has systemic contraindications: fibrillation atrial; bleeding disorders; and liver diseases.
The use of therapeutic soft lenses can also be used in non-keratitis. infectious diseases, such as filamentary keratitis, where after removing filaments in a Manually, a therapeutic contact lens is used for better patient comfort.[4,5]
The exchange of soft lenses for scleral lenses can also be without proposals, as the eclerals maintain better corneal lubrication.[4,5]
In more serious cases, autologous serum can be used, which is rich in growth, but it is difficult to obtain for use in Brazil.[4,5]
Blood products are indicated in dry eyes due to aqueous deficiency that is difficult to treat and that cannot be resolved with eye drops No preservatives.
Stimulation of tear production can be used in aqueous deficiency with the use of systemic secretagogues such as pilocarpine or sevimeline and topical production stimulators of mucin. The treatment of the evaporative component can be done by guidance, treatment of Meibomius gland dysfunction, use of special glasses and lenses, humidifiers of air, occlusion of tear punctums, and use of high-intensity pulsed light.[4,5]
Occlusion of tear punctums with plugs is efficient in aqueous dry eye, but its use is controversial in evaporative dry eye.[4,5]
The most used are point occluders collagen tear pads that have an average lifespan of 1 to 16 weeks. Non-absorbable ones are generally made of silicone and are a very interesting tool in very symptomatic after refractive surgery. In this case, they are removed 6 months after surgery. Corneal when innervation has already been reestablished.[4,5]
Plugs are only indicated after control of inflammation. In moderate and severe cases anti-inflammatory treatment may be done through the use of corticosteroids or immunomodulators such as cyclosporine or tacrolimus and aim to reduce symptoms. Topical corticosteroids should be used for a short period of time period of time with rapid regression and act by inhibiting MAPK, cytokines and metalloproteinases. [4,5]
Studies suggest that starting fluorometholone before topical cyclosporine promotes a faster improvement in the Schirmer Test, dye test and symptoms when compared to the use of cyclosporine alone. After these first weeks, gradual weaning of corticosteroids. This association promotes better adherence to treatment.
Cyclosporine 0.05% or Restasis (immunomodulator with anti-inflammatory action) is a drug in an oily vehicle, without preservatives and which acts by inhibiting calcineurin and reducing the production of IL-2 and T lymphocytes. Its onset of action is later, requiring a period of treatment of at least 6 months. Tacrolimus 0.03% and 0.01% is an option for patients who do not obtained a good response or did not tolerate cyclosporine due to its greater potency, however have low acceptance [4,5] and are better tolerated in those patients with Rosacea and blepharitis and with better acceptance at a reduced concentration (0.01% or 0.02%). O Surgical treatment in more extreme cases may involve tarsorrhaphy or bone transplantation. salivary glands.[4,5]
Debridement of the eyelid margin can also be performed (Line Marx) with the aim of releasing the orifices of the ducts obstructed by the process of hyperkeratinization.
There is a consensus that there is a need for routine preoperative assessment to assessment of the risk of developing or worsening dry eye disease in all patients.
It is believed that in most cases, around 80%, only 2 minutes are needed estimated to evaluate the ocular surface and only 5 minutes in patients at higher risk of Dry Eye disease or who have symptoms.
Tests for diagnosing dry eye have sensitivity and specificity highly dependent on the inclusion criteria for DED, study population and severity of the disease group.
In the United States of America, it is recommended to carry out a questionnaire associated with carrying out an objective test for all patients in the preoperative period of surgery of cataracts. These objective tests include measuring tear film osmolarity and/or metalloproteinase dosage.
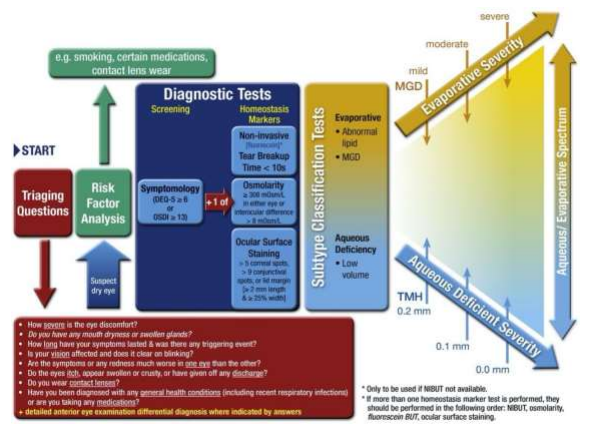
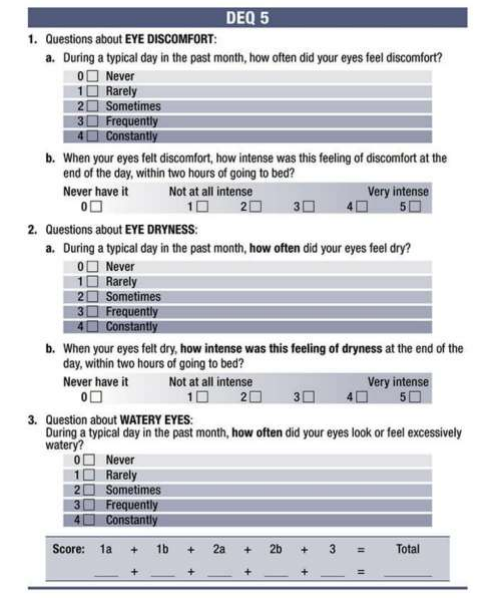
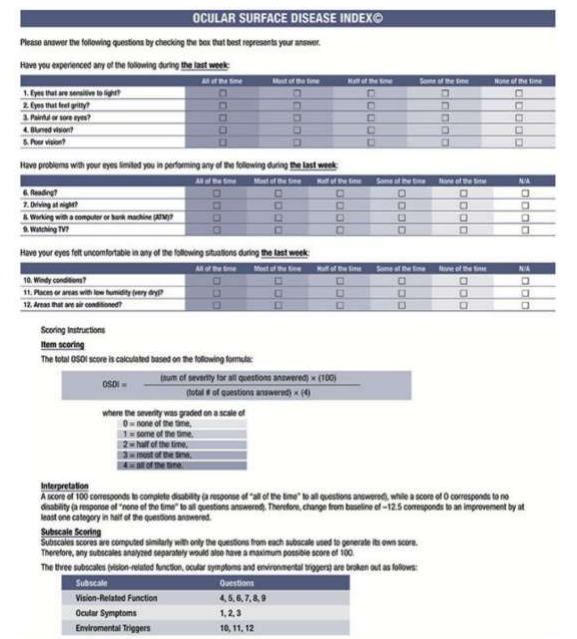
Research evidence suggests that the best form of screening would be to use questionnaires and analysis of risk factors of the patient's past history accompanied by a very detailed anterior biomicroscopy. According to DEWS-II, eye is diagnosed dry eye, if dry eye is suspected, that is, the patient presents anamnesis, risk factors for dry eye and a positive result for screening questionnaires such as: 5-item Dry Eye - DEQ-5 (Figure 2); or the Ocular Surface Disease Index (OSDI) (Figure 3) associated with an objective test, with the 3 standardized tests being staining by 1% fluorescein tear osmolarity test or Tear film break-up time (Figure 1).
Please click here to view complete article