Clinical Case Report Neonatal Meningitis due to Neisseria Meningitidis Associated with Neonatal Encephalitis due to Vhh-6 in Intensive Care Unit
Clinical Case Report Neonatal Meningitis due to Neisseria Meningitidis Associated with Neonatal Encephalitis due to Vhh-6 in Intensive Care Unit
Vallejo Chaves Saul Hernando1, Portilla Álvarez Fanny2
1-2 Neonatal Intensive Care Unit, UROS Clinic. Neiva, Huila, Colombia.
1-2 Pediatric Service, UROS Clinic. Neiva, Huila, Colombia.
*Correspondence to: Dr. Saul Hernando Vallejo Chaves, Pediatrician, Universidad Surcolombiana, Neonatal Intensive Care Unit, UROS Clinic, Email Saulhv4@hotmail.com https://orcid.org/0000-0003-3878-5256
Copyright
© 2023: Dr. Saul Hernando Vallejo Chaves. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 November 2023
Published: 27 November 2023
Abstract
Neonatal bacterial meningitis is one of the infectious diseases that is most associated with high rates of morbidity and mortality in affected individuals. Although this entity occurs worldwide, its incidence and prevalence are higher in developing countries, due to the lack of adequate prenatal control, which is one of the associated factors. In the last ten years, there has been the availability of effective antibacterial agents, which have allowed notable advances in their treatment, helping to minimize the severity of the clinical picture and/or sequelae and, consequently, a better prognosis and a reduction in the risk of infection. associated mortality; However, this disease is still common, which suggests that the key to a good prognosis lies both in its prevention, which is based on early detection and treatment before the colonization of the infectious agent in pregnant women, as well as in a good clinical diagnosis and confirmation by paraclinical studies, which will allow the appropriate treatment to be selected. The main causal agents continue to be Streptococcus agalactiae (Group B), gram negative bacilli, Listeria monocytogenes and Streptococcus pneumoniae. Risk factors are preterm birth (less than 37 weeks), premature rupture of membranes greater than 18 hours, or a maternal temperature greater than or equal to 38°C at the time of delivery. Intravenous treatment should be continued with the appropriate antibiotic for the isolated germ, up to two weeks after the blood culture becomes negative. Unfortunately, severe long-term sequelae are common (12% to 29% of those affected), especially in infections associated with group B Streptococcus and gram-negative bacilli, even in cases in which treatment has been timely and adequate. .
Human herpesvirus 6 is a ubiquitous virus to which most of the population is immune from the age of three years and older. Infections in neonates are rare, since the immune pregnant woman transmits antibodies to the fetus. The manifestations of the infection are varied, from roseola to hepatitis, meningitis or encephalitis. Human herpes virus 6, although rare, should be considered in the differential diagnosis of neonatal encephalitis.
We present the case of a full-term newborn of 20 days of life, controlled gestation with a normal course, eutocic delivery without infectious risk factors, admitted to the neonatal intensive care unit with a diagnosis of fever without focus. He went to the second level due to fever of 2 days of evolution, refusal to feed, loss of appetite, weakness, drowsiness, he had a paroxysmal crisis that required management with a barbiturate. On physical examination, signs of decompensated shock, dehydration, with a dystrophic appearance, reticular cutis, jaundiced tint up to the chest, irritable to manipulation and axial hypotonia, with the rest of the examination normal. The diagnostic aids reveal a low infectious risk blood count, frankly positive C-reactive protein (CRP 20.5 mg/dl) and procalcitonin (PCT 0.98 ng/ml), preserved kidney and liver function, non-prolonged coagulation times, normal blood glucose and electrolytes, Non-pathological urinalysis, Gram negative, lumbar puncture was performed, finding pathological cerebrospinal fluid, with marked pleocytosis of neutrophilic predominance, severe hypoglycorrhachia and marked hyperproteinorrachia, GRAM, KOH, BK, Indian ink negative, FilmArray of CSF (cerebrospinal fluid) (Table I) with positivity for the polymerase chain reaction (PCR) of HSV-6, Neiseria meningitidis (Table I), so neonatal meningococcal meningitis associated with encephalitis due to HSV -6 was diagnosed. Some characteristics of meningococcal infection and infection by herpes simplex virus type 6 are described, and the diagnosis and treatment recommended for this type of infection are highlighted, as well as reference is made to case reports published in the international literature.
KEYWORDS: Herpes virus type 6, meningococcal meningitis, Neisseria meningitidis, newborn, neonatal crisis, Neiva, Huila, Colombia.
Clinical Case Report Neonatal Meningitis due to Neisseria Meningitidis Associated with Neonatal Encephalitis due to Vhh-6 in Intensive Care Unit
Introduction
Neonatal meningitis (NM) is a devastating disease known for more than a century. The first publications highlighted its clinical rarity and cumbersome diagnostic process 1,2. However, over time it has been reported on all continents, and despite scientific and technological advances, it continues to be a public health problem 3. The incidence varies considerably. In developed countries, it is estimated around 0.3 cases per thousand live births; while, in developing countries this incidence can reach up to 6.1 cases per thousand live births3. With new methods, detection has improved and mortality has decreased; However, morbidity remains high (20-60%) 4.
NM is classified as early and late 5. Early NM begins within the first 72 hours and is related to contamination through the birth canal with bacteria such as Escherichia coli, Streptococcus group B and Listeria monocytogenes9,10. After 72 hours, late MN is related to germs from the hospital environment, such as coagulase-negative Staphylococcus and gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae, Enterobacter spp.) 5.
MN constitutes a health emergency, and as soon as it is suspected, empirical antibiotic treatment should be indicated 12. However, the diagnosis is complex due to the low specificity of the signs and symptoms and the difficulty in isolating the germs by culture, leaving it as The only recourse is clinical suspicion in the presence of risk factors 5
Given the scarce information on MN in our country, such as its frequency, impact on morbidity and mortality and the prevalence of the pathogens involved, it is of utmost importance to know the epidemiological and clinical profile of the disease. For this reason, the objective of the study was to estimate the incidence, associated factors, clinical and cerebrospinal fluid (CSF) characteristics, etiology and complications of MN.
Clinical Case
A 20-day-old male newborn, the result of the first pregnancy of a 19-year-old mother, was born by cesarean section indicated for suspected macrostomia at 38 weeks without complications and spontaneous neonatal adaptation, Silverman Anderson with a score of 0 without signs of respiratory distress, with a complete negative STORCH, admitted to a second level hospital (Pitalito – Huila) in the arms of his mother who reported a clinical picture of 24 hours of evolution characterized by unquantified feverish peaks associated with easy crying and loss of appetite, he repeatedly denied diarrhea, cough, rhinorrhea, rash and drowsiness, she was referred to a first level hospital due to persistence of fever, which they quantified up to 38.2 °C. Upon admission to this institution, a fever peak of 38.5° was documented. He denied close contact with patients with suspected and/or diagnosed COVID 19. He was admitted in acceptable general conditions, hemodynamically stable, febrile, dry mucous membranes, with clinical signs of SIRS, no evidence of SIRS. respiratory difficulty, oximetry appropriate to the environment, no signs of low output, no neurological focus. Paraclinical admission with low-risk blood count, clearly positive c-reactive protein, preserved kidney and liver function, non-prolonged coagulation times, normal blood glucose and electrolytes, non-pathological urinalysis, Gram negative, lumbar puncture procedure was performed without complications, finding cerebrospinal fluid pathological, with marked pleocytosis of neutrophilic predominance, severe hypoglycorrhachia and marked hyperproteinorrachia, GRAM, KOH, BK, Indian ink negative. Therefore, they are referred to our neonatal intensive care unit Clínica Uros for multidisciplinary management.
Patient is admitted in stable conditions hemodynamically compensated in cardiorespiratory sufficiency, with adequate pattern and saturations, from the hemodynamic point of view with adequate distal perfusion, looks pink, no signs of low output, differential blood pressure in the 4 normal extremities without requiring inotropic support at the time, At the gastro-intestinal level, she continues with breastfeeding, without distension or emesis, and adequate metabolic controls. At an infectious level, it looks bad, infected, for which studies are expanded in the context of a newborn presenting with acute febrile syndrome, with suspicion of late neonatal sepsis, due to clinical and laboratory findings, suspicion of bacterial meningitis, under antibiotic management If the diagnosis is suspected, an evaluation by pediatric infectious disease is requested. This is a patient in the course of late neonatal sepsis of meningeal focus, with documentation of meningitis due to meningococcus documented by nested PCR of meningitis performed in the clinical laboratory of the UROS clinic, presents a septic appearance in course, a meningitis form is filled out. HERPES TYPE 6 was also documented, for which treatment was started with acyclovir, it is very probable chromosomal passage without indication to start acyclovir, it was decided to suspend, given that his pleocytosis at the remission site was very important, a head CT scan was added while an MRI could be performed given that the possibility of empyema exists.
On neurological examination, active, with adequate response to stimuli, focal seizure was reported lasting more than 20 minutes with respiratory difficulty, cyanosis, oxygen was required under a nasal cannula, which was managed to be removed, impregnation with phenytoin was initiated, pediatric neurology evaluation was requested, patient was referred with high neurological risk due to meningitis and neonatal crisis, with neurological examination with deficit for gestational age, positive suction for gestational age, with simple head CT without pathological alterations, who due to paroxysmal crisis is started on management with AED, currently without new visible seizures , with 12-hour telemetry that shows pathological activity, due to this finding, anti-seizure management is appropriate, with simple brain MRI that shows occupation of the occipital horns of the lateral ventricles that presents restriction in diffusion and there are also centers of restriction in the subarachnoid space in the frontal, temporal and left parietal convexities as well as the interhemispheric sulcus. Focal hyperintensity that presents diffusion restriction in the knee of the left internal capsule of 4 mm. Rest of the brain parenchyma with signal intensity appropriate for age. Central midline. Turkish chair with usual appearance. Normal sized ventricular system. Vascular structures with signal void. Opinion: The findings described are attributed to meningitis with ventriculitis and a small ischemic lesion in the internal capsule due to a probable vasculitic focus secondary to an infectious process. An evaluation by physiatry is requested, the rehabilitation process begins, at the time of antibiotic management, with an adequate response to treatment, it is expected to evaluate short, medium and long-term sequelae.
Table 1
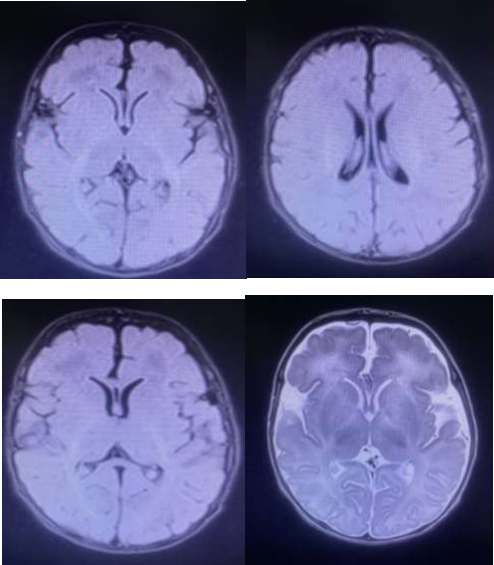
Figure 1: Simple Brain Resonance Images
Simple brain MRI that evidences occupation of the occipital horns of the lateral ventricles that presents restriction in diffusion and there are also foci of restriction in the subarachnoid space in the frontal, temporal and left parietal convexities, as well as the interhemispheric sulcus. Focal hyperintensity that presents diffusion restriction in the knee of the left internal capsule of 4 mm. Rest of the brain parenchyma with signal intensity appropriate for age. Central midline. Turkish chair with usual appearance. Normal sized ventricular system. Vascular structures with signal void. Opinion: The findings described are attributed to meningitis with ventriculitis and small ischemic lesion in the internal capsule due to a probable vasculitic focus secondary to an infectious process.
Conclusions
The incidence of meningitis is higher in the neonatal period than in any other stage of life. An estimated incidence of 0.2-1 per 1000 live newborns is estimated. The mortality of neonatal meningitis continues to be high: between 10 and 30% Of those who survive, between 20-60% present sequelae
The late form of meningitis is more common than the vertical or early form
The most frequent microorganisms in the vertical meningitis group were gram positive, while in the late meningitis group they were gram negative.
The number of meningitis due to gram-positive and negative microorganisms was similar, although in the group of patients weighing less than 1500 g the percentage of meningitis due to gram-negative microorganisms was much higher.
HHV-6 causes various clinical symptoms, including severe symptoms with important neurological sequelae. This virus is inhibited by acyclovir only at probably toxic concentrations, so it is not considered as a treatment. Although HHV-6 becomes undetectable with ganciclovir at therapeutic doses, this unfortunately does not correlate with the resolution of neurological symptoms as in the case presented.
References
1. Nuñez-Cuadros E, Yun-Castilla C, Moreno-Algarra C, Moreno-Pérez D, Ros-López B, García-Martín
2. FJ et al. Medical and neurosurgical management of Citrobacter koseri, a rare cause of neonatal meningitis. J Med Microbiol. 2014; 63:144-147
3. Coto-Cotallo GD, López-Sastre JB, Fernández-Colomer B. Castrillo Hospital Group. Neonatal meningitis. Epidemiological study of the Castrillo Hospital Group. An Pediatr. 2002; 56(6): 556-563
4. Lewis G, Schweig M, Guillén-Pinto D, Rospigliosi ML. Neonatal meningitis in a general hospital in Lima, Peru, 2008 to 2015. Rev Peru Med Exp Salud Pública. 2017; 34(2): 233-238.
5. Radouani MA, Kabiri M, Mustapha M, El Hassani A, Barkat A. Epidemiological study of neonatalbacterial meningitis: moroccan data. J Infect Dis Ther. 2014; Available online: DOI: 10.4172/2332- 0877.1000167