Efficacy of Aligner Treatment in Controlling Teeth Movement: A Review Study
Efficacy of Aligner Treatment in Controlling Teeth Movement: A Review Study
Negin Razmi Ganji 1, Ameen Saleh *2
1.BDS student in Xi’an Jiaotong University.
2.Private Practice.
*Correspondence to: Dr. Ameen Saleh, Private Practice.
Copyright
© 2023 Dr. Ameen Saleh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 November 2023
Published: 30 November 2023
Abstract
Objective: In Invisalign treatment, inconsistency between computer predicted and actual tooth movement constantly restricts professional judgment. The goal of this study was to update the evidence on the efficacy of the Invisalign appliance.
Material and methods: From 2000 to 2023, medical databases were searched for relevant peer-reviewed studies on the use of Invisalign as a therapeutic intervention. Except for case reports and case series, all human research were included.
Results: There were 25 papers in total (4 RCTs, 6 prospective cohort studies, and 15 retrospective cohort studies). Treatment results have improved recently. Except for buccolingual inclination (P = 0.005) and occlusal contacts (P = 0.001), Invisalign therapy produced outcomes equivalent to fixed appliances in extraction situations. The best accuracy for particular tooth movement was for arch expansion (upper: 72.8%, lower: 87.7%) and molar distalization (87%). The rotation of rounded teeth and management of overbite with aligners was uncertain.
Conclusion: Invisalign therapy was less than optimal for managing buccolingual inclination and occlusal contacts. None of the tooth movements were exactly as predicted. To attain high-quality outcomes, an auxiliary or amended prescription may be required. Because study materials, treatment designs, and assessment techniques varied, results should be evaluated with caution.
Efficacy of Aligner Treatment in Controlling Teeth Movement: A Review Study
Introduction
Removable appliances similar to transparent aligners have been used for mild to moderate orthodontic tooth movements since the debut of the Tooth Positioner (TP Orthodontics) in 1944. Clear aligner treatment has been used in orthodontics for decades, but it has grown increasingly popular in recent years, notably after the advent of Invisalign appliances (Align Technology) in 1998. An online search indicates that there are now at least 27 distinct clear aligner devices available for orthodontic treatment. The purpose of this study is to discuss the growing popularity of clear aligner appliances, as well as the therapeutic scope and limitations of aligner therapy in general. The article will also explain the distinctions between the many types of clear aligner products that are now available.
Invisalign has grabbed the interest of dental professionals because it provides a more aesthetically pleasing, sanitary, and non-invasive treatment alternative for those who are interested in receiving orthodontic treatment. Using a set of transparent custom-made aligners was first described by Kesling aimed to align the dentition as a refinement approach at the conclusion of conventional orthodontic therapy[1]; The concept has improved since then, and with the assistance of CAD/CAM stereolithographic technology and Clincheck ( a simulation software for visualization of tooth movement). Align Technology (Santa Clara, Calif.) introduced the Invisalign system to the orthodontic area in 1999, planning the treatment and generating a set of custom-made, clear thermoset removable aligners from a provisional impression or oral optical scan. With 22 hours of wearing time per day, Each Invisalign tray is able to produce 0.25 to 0.3 mm of anticipated dental movement every 14 days.[2]
Anterior teeth torque control is an essential aspect of orthodontic treatment, as improper torque control can result in undesirable tooth movement and affect the overall treatment outcome[3]. Fixed appliances have traditionally been the standard of care for controlling anterior teeth torque, but recent advancements in clear aligner technology have provided an alternative treatment option. While previous studies have investigated the efficacy of aligner treatment in improving dental alignment, limited research has been conducted on the effects of aligner treatment on anterior teeth torque control[4].
In 2012, Robert Keim, chose temporary anchorage devices and Invisalign as two key developments in orthodontics in the past 15 years. It was also said that Invisalign has provided patients with a viable alternative to fixed braces and that today, virtually any malocclusion can be successfully treated using this or similar technologies.[5]
The objective of this study is to evaluate the efficacy of aligner treatment in controlling several tooth movements.
Material and Methods
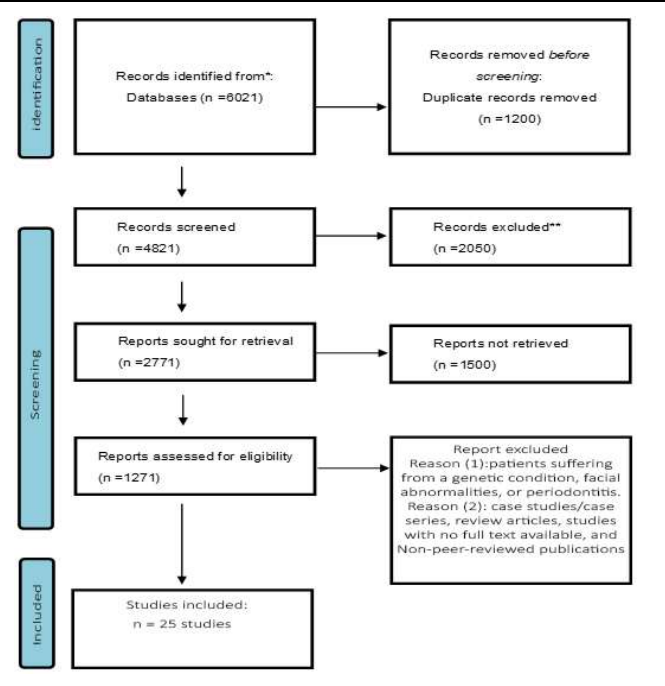
Previous systematic reviews found few papers that addressed our study issue. To broaden the research resources, randomized controlled trials (RCTs), observational studies, and any other study type, excluding case reports and case series, were included in this review. All of the research had to be about Invisalign appliances and required to quantify tooth movement or treatment results. Studies with treatment in conjunction with orthognathic surgery, patients suffering from a genetic condition, facial abnormalities, or periodontitis, case studies/case series, review articles, studies with no full text available, and Non-peer-reviewed publications were not considered in this study (Figure 1).
A comprehensive search of medical databases and Google Scholar was done. The first author (A.S.M) used the search method specified in Table 1 to obtain the available peer-reviewed papers between January 2000 and July 2023. Medline (Ovid) employed medical subject headings to accomplish the same search approach as the other databases. Google Scholar does not accept truncation symbols, and the search modality differs from that of medical databases, thus other key phrases were utilized in Google Scholar.
Table 1: search strategy and keywords
|
Database |
Keywords |
|
PubMed/Scopus/Embase Medline/Cochrane Library |
(orthodontic* OR Clear OR sequential removable) aligner* OR Invisalign and (effect* OR efficacy* OR outcome* OR Predict* OR tooth movement*) |
|
Google Scholar |
(Invisalign efficacy outcome) |
The obtained records' titles and abstracts were loaded into reference management software (Endnote X8, Clarivate Analytics, Philadelphia, PA, USA). Following deduplication, references were reviewed and evaluated using the inclusion and exclusion criteria.
Figure 1: Searching strategy flow chart
Observational study risk of bias was investigated using items drawn from the Research Triangle Institute item bank.[6] Twenty-nine questions from 11 categories intended for assessing observational studies were adapted to get 11 items for this review. Each question received a yes, no, partial, cannot determine, and not relevant response. Cannot determine and partial were thought to suggest a non-obvious risk of bias. The questions of the evaluation addressed overall bias in an individual study, and a study with more than one item scored as non-obvious or high risk of bias could not be classified as having a low risk of bias.
The scoring method was done independently by two investigators (A.S.M and S.H.C.), and any disagreements were discussed with the other authors to establish a consensus.
Table 2: Studies included in the current review
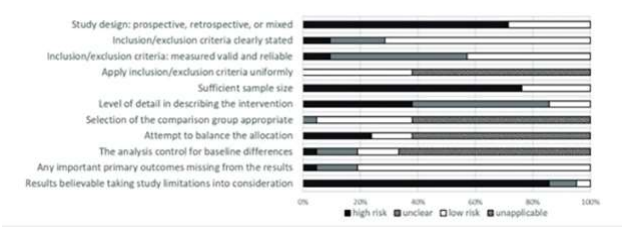
Figure 2: Risk of bias for the observational studies
Results
Following an examination of the abstracts and full texts, 25 publications (4 RCTs, 6 prospective cohort studies, and 15 retrospective cohort studies) were chosen for inclusion in the review.
The articles we found had a lot of heterogeneity, including three trials on treatment effectiveness with varying aligner thickness and wearing regimens.[23-25], six studies comparing Invisalign treatment with fixed appliances,[7-12] nine studies comparing actual tooth movement with predictions,[13-21] two studies on outcomes with different treatment strategies,[4, 22] three retrospective studies on Invisalign treatment effects,[26-28] and two studies on treatment efficacy in patients with different amounts of crowding or overbite.[29, 30]
Each study's comparison group and outcome measures were also different, as shown in Table 2 The majority of the research in our review showed insufficient description of the intervention.
Figure 2 summarizes the risk of bias assessment for observational research, more than 90% of the publications revealed a partial or high risk of overall bias due to the retrospective nature of more than half of the research (15 studies, 71.4%), one-arm study design (13 studies, 61.9%), and imprecise explanation of treatment details (18 studies, 85.7%). Table 3 and Table 4 shows the assessment findings for the RCTs and the observational studies, with numerous studies expressing concerns about the likelihood of bias.
Discussion
Most research methodologies lack agreement, which reflects the fast evolution of materials and biomechanical aspects of aligner designs. The Power Ridge, a minor distortion on the aligner for creating moments on incisors, was launched by Align Technology in 2008 as the first force-driven feature. Several more features, such as optimized attachments and particular treatment methods, were also unveiled. SmartTrack has also replaced the prior aligner material EX30. The research results related with past characteristics may not be applicable to current patients. For example, the patients in Khosravi et al.'s overbite research began therapy before the G5 protocol (Invisalign procedure for deep bite) was established and the SmartTrack material was available.[30] Thus, The capacity to control overbite with new features is yet unknown.
Early research found that extraction cases using the Invisalign appliance had a low completion rate, poor root control, and even significant dental tipping.[23-25] Kassas et al. found substantial improvements in alignment and buccolingual inclination after treatment in non-extraction cases. However, overjet, occlusal relations, buccolingual inclination, and occlusal contacts were still less controlled than with fixed appliances (p0.05).[7]
Studies undertaken following the introduction of SmartForce features yielded comparable results: reduced control of overjet, overbite, occlusal relationship, buccolingual inclination, and occlusal contacts as compared to fixed appliances.[9, 12] However, Li et al. discovered that with well-designed attachment placement and treatment methodology, root control at the extraction site can be as excellent as that of fixed appliances in their extraction research.
The treatment did not follow the expected tooth movement in ClinCheck.[17] As a result, several studies have been conducted to assess the accuracy of various forms of the orthodontic tooth movement (OTM). Certain OTM should be designed as a biomechanical force plan and overcorrection is recommended in ClinCheck.[31]. Alternatively, accessories may be required to get the desired result.
The majority of participants in the gathered samples of all sorts of aligner studies were non-extraction cases. As a result, the distance between each OTM was restricted. Grünheid et al. assessed the precision of several forms of OTM of each tooth and discovered that rotation of rounded teeth, intrusion of front teeth, and posterior tooth movements were not entirely achieved.[19] Charalampakis et al. discovered that incisor intrusion and canine rotation were the most incorrect OTM.[21] These findings were, to some extent, contradictory to Kraviz et al.'s accuracy research.[14] The disagreement may be due to changes in attachments and aligner material employed, superimposition procedures, and targeted teeth between different investigations.
Rotation, a difficult movement with Invisalign[32], was also the first form of OTM studied. Using IPR to create a gap for the rotated tooth might be crucial.[13] Vertically positioned ellipsoid attachments only provide marginal gains in rotational precision. Simon et al. discovered that premolar de-rotation accuracy with improved rotation attachment was considerably lower (37.5%).[4] These findings should be thought of with caution. The study undertaken by Kravitz et al. had sampling bias; more severe tooth rotation (more than 5°) was detected in the attachment group (15 out of 17 cases) than in the IPR (12 out of 18 cases) and control groups (2 out of 18 cases).[13] Simon et al.'s findings were attributed to poor patient compliance; after excluding outliers, the attachment group's mean accuracy was 47.3%. This discovery also shows that attachment can interact with an ill-fitting aligner to produce an undesirable force system and poorer rotation. The crown form, rotation severity, and quantity of correction per aligner all have an impact on treatment accuracy.[4, 14, 19]
The incisor lingual root torque was roughly 50% accurate.[4] Power ridge was not superior to the horizontal ellipsoid attachment. Aligners, according to Castroflorio et al., may give better root management than fixed appliances.[16] However, because all of the patients in this research had intentional lingual crown tilting rather than lingual root torque, the findings should be interpreted with caution. Torque control in molars may be impaired in posterior teeth due to the lesser force created by the aligner in this area and the bigger roots of the molars.[19]
The accuracy of distallization movement was rather good, and both were viable options for treating minor crowding with the Invisalign appliance.Duncan et al. analyzed their cases and found that the majority of patients had considerable arch extension. Invisalign therapy was more likely to procline the incisors in more crowded cases (>6 mm).[29] The linear accuracy of molar distalization was about 87% in Simon et al.'s investigation; attachments give a minor improvement to the accuracy (NS).[4] Garino et al. investigated two different attachment designs and discovered that when vertical rectangular attachments were applied from canines to second molars, distalization was almost translationally achieved; if the attachments were only applied from first premolars to first molars, less distal movement of posterior teeth was achieved.[22] To accomplish the required outcomes, planning overcorrection in molar distalization might be explored. Meanwhile, vertical rectangular attachments from the canines to the second molars may be advantageous. Shifting the cusp tip was more effective for expansion than shifting the gingival edge (tipping movement). The average accuracy assessed from the cusp tip was 82.9% in the upper arch and almost 100% in the lower arch with tipping movement.[18, 20] As a result, expansion overcorrection should be employed with caution. Periodontal tissue may be jeopardized by excessive growth. It should be noted that both Solano-Mendoza et al. and Houle et al. employed the EX30 material, which has subsequently been replaced with the SmartTrack material. To the best of our knowledge, no expansion research with new material has been reported. Several studies compared the efficacy of aligners to fixed appliances in a variety of ways, with varying findings. Grünheid et al. discovered that aligners, rather than fixed appliances, enhance intercanine distance in the lower arch.[10] Hennessy et al. discovered no difference between the two appliances in lower incisor proclination.[11]An earlier study found that fixed self-ligating brackets improved arch expansion.[8] These inconsistencies could be attributed to 1) a lack of information (e.g., Hennessy et al. only evaluated the root axis on cephalograms without taking linear measurements) and 2) an inadequate description of the treatment modality, including the amount of IPR, the movement planned in ClinCheck, and the intention to change the arch form. If arch expansion was not included in the ClinCheck design, the comparison with fixed appliances might be not matched.
Several studies have demonstrated that deep bite cases can be effectively repaired using Invisalign.[33, 34] In our review, however, the efficiency of incisor intrusion and overbite correction was variable.Khosravi et al. [14] demonstrated the therapeutic impact of overbite management and deepbite correction in their cases; molar extrusion and increased SN-MP and AFH play a crucial role in decreasing overbite. Furthermore, proclination of the lower incisors and intrusion of the upper incisors aided treatment outcomes. These modifications might be attributed to the biting ramp feature utilized in this group. Overbite was corrected in the open bite group by incisor extrusion, whereas SN-MP and AFH were preserved. Moshiri et al., on the other hand, discovered that open bite correction was achieved through molar intrusion and incisor extrusion combined with mandible autorotation[28], and they hypothesized that the thickness of the aligner material in the posterior region was insufficient to cause molar intrusion; inclusion of intrusion movement in ClinCheck should be requested.
Invisalign treatment includes several elements and auxiliary services. Furthermore, the wearing strategy, overcorrection, staging, patient compliance, and even the use of accelerating devices in combination all have an impact on the success of aligner therapy. Unfortunately, the studies in our evaluation rarely documented the therapy strategy in full. Future research into more sophisticated Invisalign features and materials, as well as well-designed procedures, will be required to give more up-to-date information on the efficacy of Invisalign therapy”[35]
Conducting a review study on the efficacy of Invisalign treatment has significant clinical relevance and applicability. It empowers practitioners to make evidence-based decisions; This ensures that clinical decisions are based on scientific research rather than anecdotal evidence or marketing claims, which aids in treatment planning, facilitates patient education, and helps practitioners stay current with advancements in technology. Ultimately, this contributes to improved treatment outcomes and patient satisfaction.
Conclusion
Twenty-five papers on the effectiveness of Invisalign therapy were evaluated. Because the majority of the studies were retrospective, the findings should be regarded with caution. To identify the consequences of certain treatment procedures and the accompanying treatment results, the research design must be thoroughly studied.
The following findings could've been taken from the existing study:
- Except for the regulation of buccolingual inclination and occlusal contacts, equivalent outcomes between Invisalign and fixed appliances can be attained with developments in material, technology, and expertise.
- Treatment accuracy varies depending on the kind of OTM. To complete complex OTM, careful Clincheck design and the usage of accessories are required.
- For some forms of OTM, overcorrection in Clincheck design can be considered, while over-expansion should be utilized with caution.
References
1. KESLING H D. Coordinating the predetermined pattern and tooth positioner with conventional treatment [J]. American journal of orthodontics and oral surgery, 1946, 32(5): 285-93.
2. SAIF B S, PAN F, MOU Q, et al. Efficiency evaluation of maxillary molar distalization using Invisalign based on palatal rugae registration [J]. American Journal of Orthodontics and Dentofacial Orthopedics, 2022, 161(4): e372-e9.
3. MURPHY S J, LEE S, SCHARM J C, et al. Comparison of maxillary anterior tooth movement between Invisalign and fixed appliances [J]. American Journal of Orthodontics and Dentofacial Orthopedics, 2023.
4. SIMON M, KEILIG L, SCHWARZE J, et al. Treatment outcome and efficacy of an aligner technique–regarding incisor torque, premolar derotation and molar distalization [J]. BMC oral health, 2014, 14: 1-7.
5. WEIR T. Clear aligners in orthodontic treatment [J]. Australian dental journal, 2017, 62: 58-62.
6. VISWANATHAN M, BERKMAN N D. Development of the RTI item bank on risk of bias and precision of observational studies [J]. Journal of clinical epidemiology, 2012, 65(2): 163-78.
7. DJEU G, SHELTON C, MAGANZINI A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system [J]. American journal of orthodontics and dentofacial orthopedics, 2005, 128(3): 292-8.
8. PAVONI C, LIONE R, LAGANÀ G, et al. Self-ligating versus Invisalign: analysis of dento-alveolar effects [J]. Annali di stomatologia, 2011, 2(1-2): 23.
9. LI W, WANG S, ZHANG Y. The effectiveness of the Invisalign appliance in extraction cases using the the ABO model grading system: a multicenter randomized controlled trial [J]. International journal of clinical and experimental medicine, 2015, 8(5): 8276.
Please click here to view complete article