A Case of Panfolliculoma in a Patient with CYLD Cutaneous Syndrome
A Case of Panfolliculoma in a Patient with CYLD Cutaneous Syndrome
Maryam Abdo, MD1, Farhan Ismael Sami, MD 2*, Daniel J. Mettman, MD3
1. PGY-3, Pathology and Laboratory Medicine, The University of Kansas Medical Center.
2. PGY-2, Pathology and Laboratory Medicine, The University of Kansas Medical Center.
3. Assistant Professor, Pathology and Laboratory Medicine, The University of Kansas Medical Center.
*Correspondence to: Farhan Ismael Sami, MD, PGY-2, Pathology and Laboratory Medicine, The University of Kansas Medical Center.
Copyright
© 2023 Farhan Ismael Sami, MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 October 2023
Published: 06 December 2023
DOI: https://doi.org/10.5281/zenodo.10275665
Abstract
Panfolliculoma (PF) is a very rare benign adnexal skin tumor displaying follicular differentiation with recapitulation for each component of the normal hair follicle. It usually presents clinically as a solitary, small (<3 cm), slow-growing, tumor on the face or scalp. To our knowledge, none of the reported cases have occurred in a patient with a known diagnosis of an inherited syndrome. Herein we report the first case of a panfolliculoma in a patient with CYLD cutaneous syndrome.
Key Words: (Panfolliculoma, Folliculosebaceous neoplasms, CYLD cutaneous syndrome, Brooke-Spiegler Syndrome, Familial Cylindromatosis, Multiple Familial Trichoepithelioma).
A Case of Panfolliculoma in a Patient with CYLD Cutaneous Syndrome
Introduction:
Panfolliculoma (PF) is a very rare – fewer than 50 cases reported benign adnexal skin tumor displaying follicular differentiation with recapitulation for each component of the normal hair follicle. It was first described by Ackerman in 1993 as “superficial trichoblastoma with advanced follicular differentiation” with the term “panfolliculoma” penned to communicate the recapitulation of all hair follicle components (1). In 2014, Shan and Guo classified PF into three subtypes: nodular, in which neoplastic cells predominate as solid dermal cell aggregates; cystic, in which neoplastic cells predominate as cystic dermal cell aggregates; and superficial, in which neoplastic cells predominate as intraepidermal cell aggregates (2). Clinically, PF usually presents clinically as a solitary, small (<3 cm), slow-growing, tumor on the face or scalp (3). They tend to occur in adulthood and there is a slight predilection for males (4). To our knowledge, none of the reported cases have occurred in a patient with a known diagnosis of an inherited syndrome.
CYLD?cutaneous syndrome (CCS) is an autosomal dominant disorder that is most commonly diagnosed in the second or third decade by the manifestation of multiple benign skin tumors. CCS encompasses the conditions formerly broken into Brooke-Spiegler syndrome, multiple familial trichoepithelioma, and familial cylindromatosis (5). As such, the syndrome is characterized by any of trichoepitheliomas, trichoblastomas, cylindromas, or spiradenomas and the presence of a germline CYLD mutation (5).
Herein we report the first case of a panfolliculoma in a patient with CYLD cutaneous syndrome.
Case Report:
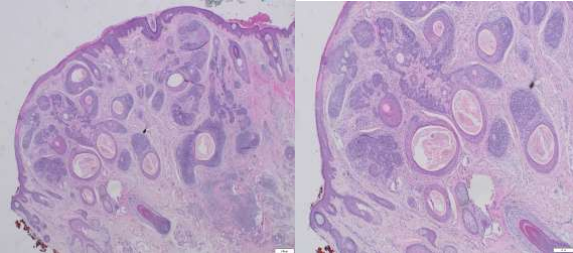
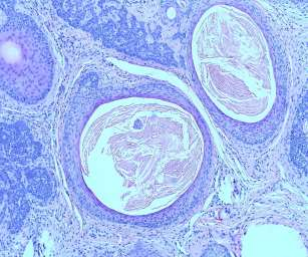
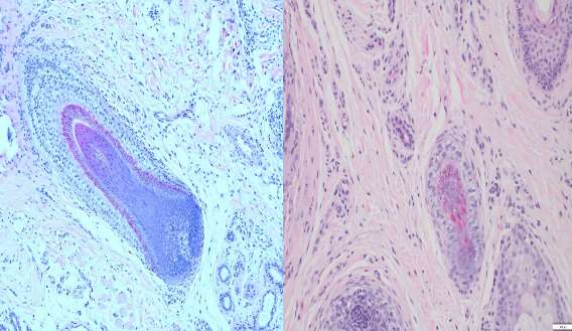
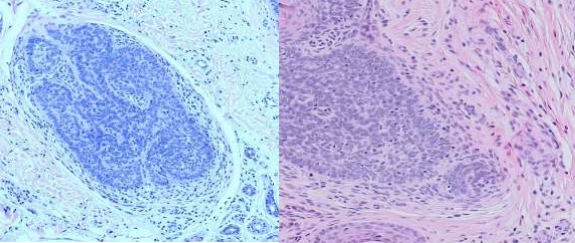
A 39-year-old male presented to the dermatology clinic of a Veterans Affairs medical center with a cystic nodule of the left medial eyebrow measuring 0.8 x 0.7 cm (figure 1). The patient was known to have CCS. His father, paternal aunt, and paternal grandfather had been diagnosed with Brooke-Spiegler syndrome (diagram 1). After presenting with multiple trichoepitheliomas, he had tested positive for a heterozygous pathogenic variant (c.2288-2289del p.Phe 763) of CYLD NM-015247.2CYLD. With this history, the clinical differential for this eyebrow lesion was cylindroma versus spiradenoma. Microscopic examination of the excision specimen revealed a well-circumscribed, dermal-based adnexal proliferation with areas recapitulating each part of the normal hair follicle: the?infundibulum, inner root sheath, outer root sheath, matrix, and bulb (figure 2.A&B). Areas resembling the infundibular portion of the hair follicle contained cystic cell aggregates lined by stratified squamous epithelium with a granular layer and filled with “basket-weave” orthokeratin (figure 2.C). Areas resembling the suprabulbar portion of the hair follicle showed clear cells as seen in the external root sheath and eosinophilic cells as seen in the internal root sheath (figure 2.D&E). Areas resembling the bulbar portion of the hair follicle showed immature basaloid cells and papillary mesenchymal bodies (figure 2.F&G). The lesion was uniformly circumscribed and without cytologic atypia, so a diagnosis of PF was rendered.
Discussion:
Our case is classic for a panfolliculoma with the presentation of a small, slow-growing nodule on the face of an adult male and the histomorphology of a benign, nodular-type, dermal-based, adnexal proliferation with areas recapitulating each part of the normal hair follicle.
As stated before, to our knowledge, based on a PubMed search of “panfolliculoma”, fewer than 50 cases – 45 to be exact – have been described in the literature. None of the reported cases mentioned a known diagnosis of or clinical suspicion for an inherited syndrome with the exception of one case in which the patient and her daughter had similar lesions (6).
Therefore, this case of panfolliculoma in a patient with known CYLD cutaneous syndrome represents the first case of panfolliculoma in a patient with a known inherited syndrome. Our medical center has only around 1,000 dermatologic surgical pathology specimens per year. The detection of a lesion that has been reported fewer than 50 times at an institution with such a low volume raises the question as to whether this lesion is underrecognized and/or that this rare lesion was present in this patient because of this patient’s rare condition (i.e. CYLD cutaneous syndrome). Either way, this report adds to the limited literature on this entity and lays the groundwork for additional reports to investigate a possible relationship between panfolliculoma and CCS or any other inherited syndromes.
Figure 1. Left medial eyebrow cystic nodule
Figure 2.A&B Dermal-based adnexal proliferation of cystic and solid structures with follicular differentiation towards all components of the hair follicles (4X, 10X)
Figure 2.C Infundibular/isthmus differentiation (20x)
Figure 2.D&E Area resembling the suprabulbar portion of the hair follicle (20x)
Figure 2. F&G Area resembling bulbar areas with immature basaloid cells and papillary mesenchymal bodies
Figure 3. Family pedigree showing four members in three successive generations affected with the disease: grandfather, father, paternal aunt, the patient.
Conclusion:
Panfolliculoma is a rare, likely underreported, benign follicular neoplasm. This case arising in a patient with confirmed CCS raises the possibility of an association between the two conditions. Attention on this diagnosis and case may result in increased reporting of this entity and establishment of a relationship – or lackthereof – between panfolliculoma and CCS.
Financial support and sponsorship: None
Conflicts of interest:
There are no conflicts of interest.
References:
1.Ackerman, A.B.; de Viragh, P.A.; Chongchitnant, N.?Neoplasms with Follicular Differentiation; Lea & Febiger: London, UK, 1993.?
2.Shan, Shi-Jun, and Ying Guo. "Panfolliculoma and histopathologic variants: a study of 19 cases."?The American Journal of Dermatopathology?36, no. 12 (2014): 965-971.
3.Tumours of cutaneous appendages. In: Patterson JW. Weedon's skin pathology, 4th edn. Churchill Livingstone, 2016: 919.
4.Juang, Shiow-Jen, Khin-Than Win, and Feng-Jie Lai. "Panfolliculoma: Report of the Youngest Case and Literature Review of Its Histopathologic Variants."?Life?12, no. 6 (2022): 881.
5.Dubois A, Rajan N. CYLD Cutaneous Syndrome. 2020 Apr 16. In: Adam MP, Mirzaa GM, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555820/
6.Abid A, Parker D, Blalock TW. Panfolliculoma in SUFU-mutated basal cell nevus syndrome. JAAD Case Rep. 2023 Feb 19;34:40-42. doi: 10.1016/j.jdcr.2023.01.033. PMID: 36936865; PMCID: PMC10018224.