Extramedullary Plasmacytoma of the Nasopharynx: A Case Report
Extramedullary Plasmacytoma of the Nasopharynx: A Case Report
Syeda Anam Hassan*1
*Correspondence to: Syeda Anam Hassan, India.
Copyright
© 2023 Syeda Anam Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 November 2023
Published: 13 December 2023
Abstract
Plasmacytoma is a rare and discrete solitary mass of neoplastic monoclonal plasmacells. Extramedullary plasmacytoma(EMP) tends to occur during the 5th and 7th decades of life and is rarely diagnosed in younger patients. Here we report a 38yr old female patient presenting with longterm nasal obstruction; who was found to have emp of nasopharynx. The patient was treated with radiotherapy with a satisfactory outcome.
Key Words: plasmacytoma, extramedullary ,head and neck, nasopharynx.
Extramedullary Plasmacytoma of the Nasopharynx: A Case Report
Introduction
Plasmacytoma is a rare and discrete solitary mass of neoplastic monoclonal plasmacells,which was first described by schridde in 1905(1).Emp has been reported rarely and accounts for 4% of all non epithelial tumors of upper respiratory tract(2). while ocassionally localised to git, lungs, testes and skin.It has been previously reported that 80% of Emp are localised in H&N region(3,4). Common clinical symptoms include epistaxis, rhinorhea, a sore throat dysphonia and hemoptysis(5,6). EMP is usually managed through radiotherapy with or without surgery. The current presents the case of a middle age female patient with Emp of nasopharynx who was treated successfully with radiotherapy.Written informed consent was obtained from the patient.
Case Report
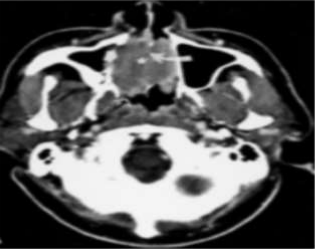
A 38yr old female was reported to the Department of Radiotherapy in the month of July at MNJ Cancer Hospital due to chief complaints of intermitent epistaxis from nose since 3months,In addition,the patient reported difficulty in swallowing ,persistent nasal obstruction and snoring.A phyisical examination revealed a mass seen in nasopharynx.on clinical examination of neck,a node is present on the left side of neck level 2 was seen. Magnetic Resonance Imaging of head and neck showed evidence of Nasopharynx-T1/T2 isointense moderatly homogenously enhancing soft tissue density lesion in nasopharynx along the midline approximately m/s 32x30mm ,superiorly fat planes lost with planum sphenoidale.Inferiorly fatplanes lost with distal aspect of hardpalate.Anteriorly fat planes lost with superior and middle turbinate(Right>left). There is evidence of few enlarged level IB, 2 nodes on the left largest m/s 18x15mm at level 2a.
On HPE: Microscopically The tumor shows cells arranged in sheets and individually scattered. Individual cells are round to oval with moderate amount of cytoplas; round hyperchromatic nucleus and prominent nucleolus focal areas of hyalinization and congestive blood vessels are seen f/s/o undifferentiated Nasopharyngeal carcinoma.
Specimen -> Nasopharyngeal mass biopsy -> Block received.[2nd opinion)
Microscopillay -> Sections are infiltrated by sheets of uniform polygonal cells with eccenteric nucleus with cart wheel chromatin and a rim of cytoplasm with a perinuclear clearing in some cells.Few of these have central nuclei and occassional binucleate forms are seen.Homogenous Esoinophilic material is seen between.The material is congophilic with reddish green birefringence under polarized light confirming it as amyloid.
Figure 1
Figure 2
Figure 3
Diagnosis
The above features are consistent with a plasmacytoma with amyloid deposits.
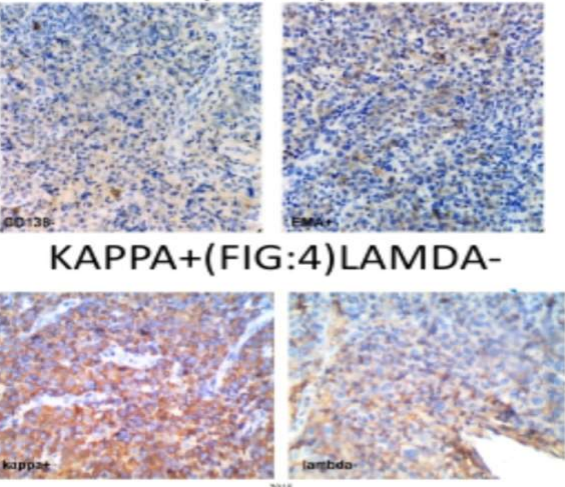
The positivity for vimentin and EMA and negativity for pancytokeratin reported else where are consistent with the immune profile of plasma cells.
IHC report showed: Kappa - Positive
Lamba - Negative
IMP: Morphology is correlation with Immune stains consistent with plasma cell Neoplasm.
FNAC from left cerical L. N showed: Plasma cell Neoplasm
In addition; expression was +ve IgG, K+ve; m band present; i.e monoclonal gammopathy was seen in IgG and Kappa region.The CBP; sr.calicum creatinine and uric acid within normal limits. On Electrophoresis of sr.protein; m band was seen in gamma region; B2 globulin was reduced; gamma globulin was increased and whole body bone survey revealed no detectable osteolytic linens. A bone marrow aspiration was in normal limits. A final diagnosis of Extramedullary plasma cell of Nasopharynx was determined and IMRT was planned for the patient.
Discussion
Plasmacytomas are rare tumors that often appear in the H&N region and are characterised by monoclonal prolifation of plasma cells.These are classified into 3 subtypes.The most common type is multiple Myeloma; which is usually a disseminated disease and is characterised by abnormal M protein. The other two types; Solitary plasmacytoma of bone and EMP of soft tissue, are considerably less common.On both clinical presentation and pathologic examination these tumors may be confused with more common tumors of head and neck. Medullary plasmacytoma has more tendency for conversion to multiple Myeloma when compared to extramedullary plasmacytoma.The diagnosis of EMP of soft tissue has been based on following Inclusion criteria. (1)Pathological tissue evidence of momclonal plasmacells involving a singal extramedullary site. (2)No bone marrow involved. (3)Negative skeletal survey results. (4)No anemia; hyperical cornea or renal impairment lavsed by plasmacell dyscrasia and (5)low screen or urinary levels of monoclonal immunoglobulin(8).There is greater male prepondrence (M:F IS 3:1) and EMP tends to occur during the 5th and 7th decades of life; rarely being diagnosed in younger patients. Only four cases of EMP have been previously reported in relatively young patients:
(1) Two 3.5yr old males with unexpected EMP followig adenoidectomy for chronicrihnosinusitis. (2) A 12yr old female who presented with progressive hoarseness and was subsequently found to have EMP coexisting with localized involving the larynx(10) and (3) A 11yr old male who presented with an EMP of orbit(11). (4) In present patient the tumor was localized in the nasopharynx.There was no involvement of bony structure or bone marrow and the diagnosis of solitary EMP of nasopharynx was confirmed. The etiology of this disease remains unkown; but factors such as viral (EBV) pathogensis and chronic irritation from inhaled irritants have been previously indicated(12-14) Despite the typical presentation as a locally destructive tumor, plasmacytomas are highly radiosensitive; 70-80% survival may be obtained with the use of radiotherapy.Radiotherapy remains the main stay for management of EMP.
The biochemical nature of amyloid deposits was also shown to be of kappa Ig light chain; suggesting the pathogenic relationship between Plasmacytoma and Amyloid deposition in the nasopharynx of this patient. There was no other evidence of malignancy or amyloid else where.This case aslo supports the concept that localized Nasopharynxed Amylodosis may be manifestated of low grade B – cell lymphoma(10)
Previously; Susnerevala et al proposed a pathological grading system based on multiple myeloma grading criteria; tumors classified into low, intermediate and high grades, whicha have been found to correlate closely with outcomes. The study recommended the use of adj chemo in patients with higher grade disease (14).The general EMP; are considered radiosensitive with a local control rate of 90-100% (15).
A radiation dose of 40-50Gy delivered to the primary site of EMP in the nasopharynx is usually recommended(8). Irradiation to the neck is required only in cases with clinically positive cervical node mets. In a recent study it was found that the primary modality of EMP is radiotherapy. Moreover, RT combined with surgery produced an improved outcome, as determined by survival rates(12). Although the rate of chemotherapy in EMP treatments has not been established, chemo is usually considered for EMPs with high risk factors for local treatment failure (tumor size >5cm) and in case of refractory disease.
Followup radiological and electrophoresis assessment is required following treatment to detect recurrence and progression to multiple myeloma, which occurs in 10-30% of cases. The overall 10 yr survival rate is 70%. (7, 8) A literature search revealed no preblications supporting the use of surgery alone to treat EMP. In the current case, the patient was treated with IMRT.
Reference
1.Schridde H. Weitere Untersuchungen uber die Kornelungen der Plasmazellen. Centralbl Allg Pathol Anat. 1905;16:433–435. (Article in German)
2.Fu YS, Perzin KH. Nonepithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx. A clinicopathologic study VI Fibrous tissue tumors (fibroma, fibromatosis, fibrosarcoma) Cancer. 1976;37:2912– 2928. [PubMed]
3.Knowling MA, Harwood AR, Bergsagel DE. Comparison of extramedullary plasmacytomas with solitary and multiple plasma cell tumors of bone. J Clin Oncol. 1983;1:255–262. [PubMed]
4.Galieni P, Cavo M, Pulsoni A, et al. Clinical outcome of extramedullary plasmacytoma. Haematologica. 2000;85:47–51. [PubMed]
5.Miller FR, Lavertu P, Wanamaker JR, Bonafede J, Wood BG. Plasmacytomas of the head and neck. Otolaryngol Head Neck Surg. 1998;119:614–618. [PubMed]
6.Nofsinger YC, Mirza N, Rowan PT, Lanza D, Weinstein G. Head and neck manifestations of plasma cell neoplasms. Laryngoscope. 1997;107:741– 746. [PubMed]
7.Straetmans J, Stokroos R. Extramedullary plasmacytomas in the head and neck region. Eur Arch Otorhinolaryngol. 2008;265:1417–1423. [PubMed]
8.Soutar R, Lucraft H, Jackson G, et al. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol. 2004;124:717– 726.[PubMed]
9.Mann G, Trebo MM, Minkov M, Simonitsch I, Chott A, Gadner H. Extramedullary plasmacytoma of the adenoids. Pediatr Blood Cancer. 2007;48:361–362. [PubMed]
10.Nagasaka T, Lai R, Kuno K, Nakashima T, Nakashima N. Localized amyloidosis and extramedullary plasmacytoma involving the larynx of a child. Hum Pathol. 2001;32:132–134. [PubMed]
11.Sharma MC, Mahapatra AK, Gaikwad S, Biswal A. Primary extramedullary orbital plasmacytoma in a child. Childs Nerv Syst. 1996;12:470–472. [PubMed]
12.Sasaki R, Yasuda K, Abe E, et al. Multi-institutional analysis of solitary extramedullary plasmacytoma of the head and neck treated with curative radiotherapy. Int J Radiat Oncol Biol Phys. 2012;82:626– 634.[PubMed]
13.Sasaki S, Hashimoto K, Nakatsuka S, et al. Plasmablastic extramedullary plasmacytoma associated with Epstein-Barr virus arising in an immunocompetent patient with multiple myeloma. Intern Med. 2011;50:2615–2620. [PubMed]
14.Susnerwala SS, Shanks JH, Banerjee SS, Scarffe JH, Farrington WT, Slevin NJ. Extramedullary plasmacytoma of the head and neck region: clinicopathological correlation in 25 cases. Br J Cancer. 1997;75:921– 927. [PMC free article] [PubMed]
15.Chao MW, Gibbs P, Wirth A, Quong G, Guiney MJ, Liew KH. Radiotherapy in the management of solitary extramedullary plasmacytoma. Intern Med J. 2005;35:211–215. [PubMed].