The Practice of Neonatal Resuscitation at the Limits of Viability – UAE Perspective
The Practice of Neonatal Resuscitation at the Limits of Viability – UAE Perspective
Dr. Nuralhuda Omar*, Dr. Dalia Ra’a Said, Dr Sameh Aly Kasem
*Correspondence to: Dr. Nuralhuda Omar, United Arab Emirates- UAE.
Copyright
© 2023: Dr. Nuralhuda Omar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 November 2023
Published: 15 December 2023
Abstract
Background: Attitude toward neonatal resuscitation at the limits of viability between 22 -24 weeks of gestation have been variable among neonatologists. Extremely preterm infants' eligibility for intensive care is frequently determined by gestational age. However, the prognosis for these patients is still also impacted by other variables as birth weight, complication during pregnancy and condition at birth.
Objective: Explore and compare the current approach to delivery room management of extremely premature infants in the peri viable period (22-24 weeks gestational age) within various perinatal centres around the United Arab Emirates.
Methods: This is a qualitative electronic study design conducted among consultant neonatologists, senior neonatal specialists and neonatal fellows. Data collected and statistically analyzed.
Results: Majority of neonatologists believe that the survival rate of 22 weeks is poor (<20%), while the survival rate of 23 week is expected to improve to (40-60%). Other than gestational age birth weight was among the most important factors (75%) that might impact the decision to of resuscitation. Among respondents (53%) believe resuscitation should be initiated starting from 23 weeks’ gestation, while (16%) suggest beginning resuscitation from 22 weeks’ gestation. Physicians believe that parents have the right to participate in decision making regarding full resuscitation (38%) as youngest as 22 and 23 weeks.
Conclusion: Our results reveal that the physicians showed less preference in resuscitation at 22 weeks gestation , whereas they should always be resuscitated from 24 weeks gestation and it is a grey area at 23 weeks. The prognosis of a favorable outcome and decision for resuscitation depends on multiple factors than decisions based on gestational-age thresholds. Birth weight was among the most important factors that might impact the decision to resuscitate at the edge of viability
The Practice of Neonatal Resuscitation at the Limits of Viability – UAE Perspective
Introduction
In taking care of extreme preterm infants the decisions about whether to resuscitate or not can be really challenging at the limits of viability of extremely preterm (22 -24 weeks of gestational age). When these extremely preterm infants born, they encounter several difficulties with high rates of mortality and morbidity. Survival rate of extreme preterm has increased over the last few decades due to several factors as antenatal steroids, early surfactant administration, total parenteral nutrition and diverse modalities of mechanical ventilation . However, with the advancements in medical care, there still remain a dynamic concern regarding long-term morbidity and neurodevelopmental impairment among survivors in preterm population. Making decisions about to offer resuscitation or not is based on the medical advancements, it is also dependent on the views of hospitals where experienced neonatologists are and available resources. Several obstacles may limit the age of viability survival rate. Furthermore, resuscitation thresholds have been variable among neonatologists.
There remains a need for understanding how physicians make these decisions of saving the lives of premature babies by studying what the attitude, and practices of neonatologists when confronted with these situations.
Methodology
This is a qualitative Electronic study design conducted among 37 physicians working in the Neonatal Intensive Care units (NICU) within various hospitals around the UAE . Ethical approval from the local ethics committee was obtained. A self-administered questionnaire was distributed to physicians over E-mail. The questionnaire included various aspects of the study objectives including demographic data of participants, level and capacity of the prenatal care unit, perception of the expected survival rate of different gestational age groups from 22 – 24 Weeks of gestation. Furthermore, the participants were questioned about their behavior towards decision of resuscitation when asked about several clinical scenarios. 1) a female preterm, mother had received steroids antenataly, 2) a male preterm, mother with no any antenatal steroids, 3) preterm, active , heart rate of 130. 4) a nonreactive preterm, poor tone, heart rate of 60. Doctors were asked to show their practice in each scenario at 22-, 23- and 24-weeks gestational age.
Those scenarios adopted from Jonathan M. Fanaroff et al. study [1]. Factors that influenced the decision to provide resuscitation were also evaluated. Results were statistically analyzed.
Results
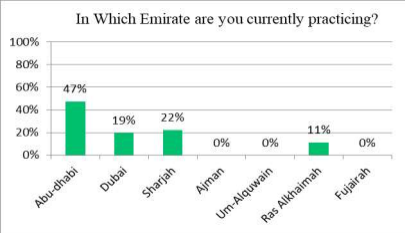
The questionnaire was mainly distributed in physicians working in governmental hospitals in various emirates with majority of responders being from the Emirate of Abu-Dhabi 47% and the remaining from Dubai, Sharjah and Ras Al-Khaimah (Figure 1).
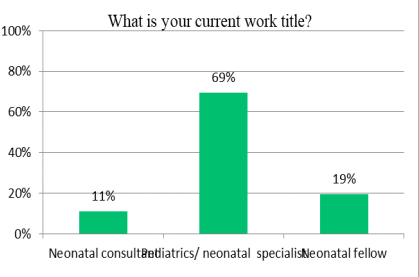
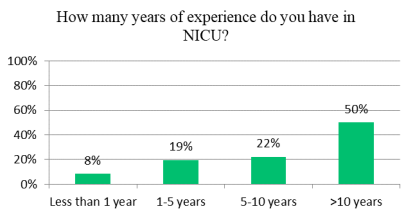
Most of the physicians who participated in the study are specialists 69% while neonatology consultants 11% and the remaining being training fellows (Figure 2). Almost 50% of physicians have more than a 10-year experience in NICU settings (Figure 3). All physicians reported that they are working in level 3 and above NICU. The average number of beds in NICU units was 50 beds.
Figure 1. Distribution among various Emirates.
Figure 2. Distribution of Physician.
Figure 3. Years of experience
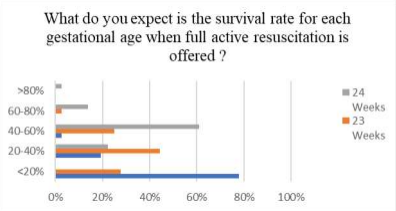
It was found that majority of neonatologists believe that the survival rate of 22 weeks of gestation is expected to be <20%, the survival rate of 23 week is expected to be between 20-40% and the survival rate of 24 week is expected to be 40-60% (Figure 4).
Figure 4. Expected Survival Rate for Gestational age 22-24 Weeks
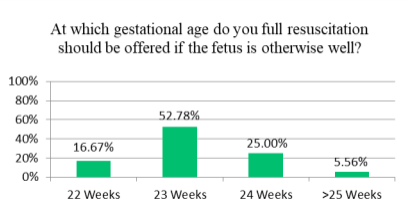
Majority of neonatologists (53%) believe full resuscitation should be initiated starting from 23 weeks’ gestation, while a minority (6%) believe resuscitation should be initiated from > 25 weeks’ gestation, 16% of physicians suggest beginning resuscitation from 22 weeks’ gestation figure 5
Figure 5. Gestational Age at which physicians will attempt resuscitation.
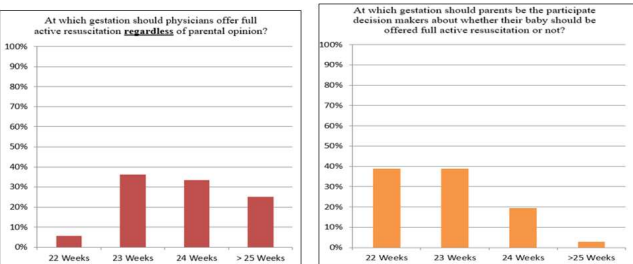
Physicians believe that parents have the right to participate in decision making regarding full resuscitation equal (38%) at 22- and 23-weeks’ gestation. Meanwhile, majority of physicians believe that resuscitation should be attempted starting 23 weeks of gestation compared to 22 weeks of gestation (Figure 6).
Figure 6. Impact of parental decision on physician attempt to do resuscitation
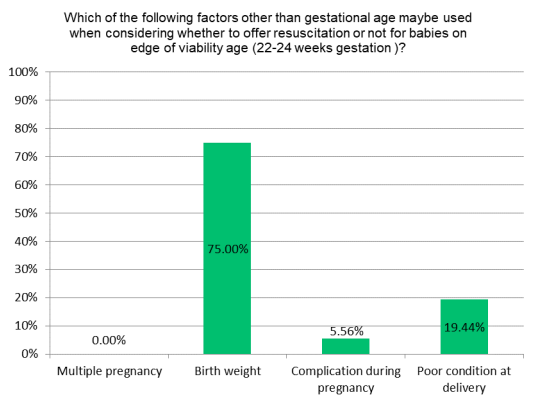
Figure 7. Factors affecting decision for resuscitation other than gestational age.
As per our local neonatologist population, birth weight was among the most important factors (75%) that might impact the decision to resuscitate at the edge of viability and around (20%) poor condition at delivery (Figure 7).
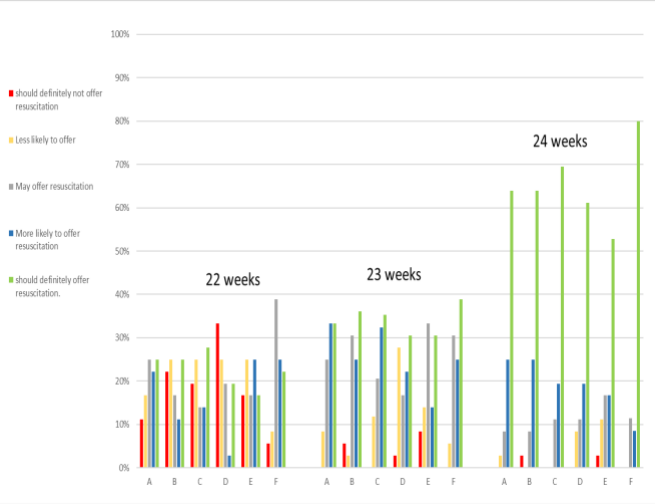
Figure 8. The participants were asked about their behavior towards decision of resuscitation when asked about several clinical scenarios. (A)Parents want full resuscitation where clinicians feel it is not the baby’s best interest. (B) Parents wants comfort care only where clinician feels baby should be offered full resuscitation. (C) Low socioeconomic status of the family. (D) Presence of known abnormality requiring surgery. (E) Presence of known anomaly compatible with life. (F) Previous pregnancy loss / No live born children
Figure 9. The participants were asked about their behavior towards decision of resuscitation when asked about several clinical scenarios. (i) a female preterm, mother had received steroids antenataly (ii) a nonreactive preterm, poor tone, heart rate of 60. Participants were asked to select their response at 22, 23 and 24 weeks of gestation for each of the following scenarios: (i) start resuscitation with full care (intubation with chest compressions), (ii) start pulmonary resuscitation only (intubation with no chest compressions), (iii) comfort care measures only (no intubation and no chest compres- sions) and (iv) other (none of the above options). Those scenarios adopted from Jonathan M. Fanaroff et al. study [1].
Figure 9. The participants were asked about their behavior towards decision of resuscitation when asked about several clinical scenarios. (i) a male preterm, mother with no any antenatal steroids, (ii) a preterm, active , heart rate of 130. Participants were asked to select their response at 22, 23 and 24 weeks of gestation for each of the following scenarios: (i) start resuscitation with full care (intubation with chest compressions), (ii) start pulmonary resuscitation only (intubation with no chest compressions), (iii) comfort care measures only (no intubation and no chest compres- sions) and (iv) other (none of the above options). Those scenarios adopted from Jonathan M. Fanaroff et al. study [1]. \
Discussion
The issue of resuscitating extremely premature infants on the margins of viability continues to be a topic of debate and controversy around the world . When it comes to current practice this study conducted among physicians working in the Neonatal Intensive Care units (NICU) within various hospitals around the UAE majority agree if parents desire resuscitation 22 weeks gestational age is the youngest age to offer active resuscitation, while it should always be attempted starting from 23 weeks as youngest age regardless the parents wish.
In comparison a study done by Bonnie H. Arzuaga et al. [3], of total of 758 surveys which demonstrate geographical variation but overall, 68% providers contemplate 23-week gestation to be the youngest age that should be resuscitated at parental demand while 51% considered 25-week gestation to be the youngest age of obligatory resuscitation even with parental refusal.
When making decisions regarding the resuscitation of extremely premature infants, it is important to consider survival outcomes which may play a role in the decision to offer resuscitation or withdraw intensive care intervention. The physicians in this survey expected survival rate of 22 week to be lower than 20%, and higher survival rate expectation at 24-week gestation (40-60%). To the best of our knowledge, so far there is no published local data in the United Arab Emirates (UAE) regarding survival rate of extremely premature infants. However, there is one study done by Tyson et al. [4] in US, among the 4192 study infants for whom consequences were demonstrated at 18 to 22 months, 49% died, 61% died or had intensely impairment, and 73% died or had impairment. The rates for these consequences in accordance to the week of gestation were 95%, 98%, and 99%, correspondingly among study infants born at 22 weeks; 74%, 84%, and 91% among study infants born at 23 weeks; 44%, 57%, and 72% among study infants born at 24 weeks.
The main purpose was to determine attitude towards decision of resuscitation of extremely premature infants at the limits age of viability (22-24 weeks gestation) when asked about different clinical scenarios to select their likely response at 22, 23 and 24 weeks, scenarios questions adopted from Jonathan M. Fanaroff et al. study [2]. We noted variations between physician attitude in the case of a female infant whose mother had received antenatal steroids 94% choose to start resuscitation with full care (intubation with chest compressions), if infants born at 24 weeks, 88% at 23 weeks and 50% at 22 weeks’ gestation while 30% physicians toward comfort care measures only at 22 weeks’ gestation. Also, it showed approximately the same response when asked about a situation of a male infant whose mother had not rceived antenatal steroids. Participants were asked as well to select their likely response at 22, 23 and 24 weeks of gestation for each of the following scenarios:
•A premature infant who was lively and horrible with a heart rate of 130
•A nonreactive infant with deprived tone having heart rate of 60.
At 24 and 23 weeks of gestation, there was a preference for full support in both scenario , while 47% select comfort care measures only (no intubation and no chest compressions) at 22 weeks of gestation. In Jonathan M. Fanaroff et al. study [2]. The preference was for comfort care in situations where the group considered there to be a higher chance of a poor outcome. This included the case scenarios of male infants who had not received steroids as well as infants who were nonreactive and had a low heart rate at birth. There was a strong preference for resuscitating female infants who had received steroids as well as vigorous and active infants.
Conclusion
Our results reveal that the physicians showed less preference in resuscitation at 22 weeks gestation, whereas they should always be resuscitated from 24 weeks gestation and grey area at 23 weeks. The prognosis of a favorable outcome and decision for resuscitation depends on multiple factors than decisions based solely on gestational-age thresholds. Birth weight was among the most important factors that might impact the decision to resuscitate at the edge of viability.
Limitations
•In this qualitative study may be variation between how a physicians answered a survey questions and how they would act in real situation.
Consent: No individual person’s data asked in the survey or appears in this manuscript.
Competing of interests: The authors have no conflicts of interest relevant to this article to disclose.
References
1.Fanaroff, J.M. et al. (2014) ‘The ethics and practice of neonatal resuscitation at the limits of viability: An international perspective’, Acta Paediatrica .
2.Rent, S. et al. (2022) ‘Perspectives on resuscitation decisions at the margin of viability among specialist newborn care providers in Ghana and Ethiopia: A qualitative analysis’, BMC Pediatrics, 22(1).
3.Meadow, W. and Arzuaga, B. (2013a) ‘National variability in neonatal resuscitation practices at the limit of viability’, American Journal of Perinatology, 31(06), pp. 521–528.
4.Tyson, J.E. et al. (2008) ‘Intensive care for extreme prematurity — moving beyond gestational age’, New England Journal of Medicine, 358(16), pp. 1672–1681
5.Cavolo, A. et al. (2019) ‘Physicians’ attitudes on resuscitation of extremely premature infants: A systematic review’, Pediatrics, 143(6).
6.Mactier, H. et al. (2020) ‘Perinatal management of extreme preterm birth before 27 weeks of gestation: A framework for practice’, Archives of Disease in Childhood- Fetal and Neonatal Edition, 105(3), pp.232–239.
7.Singh J, Fanaroff J, Andrews B, et al. Resuscitation in the “gray zone” of viability: determining physician preferences and predicting infant outcomes. Pediatrics 2007;120(3):519–526
8.Partridge JC, Freeman H, Weiss E, Martinez AM. Delivery room resuscitation decisions for extremely low birthweight infants in California. J Perinatol 2001;21(1):27–33
9.Janvier A, Leblanc I, Barrington KJ. The best-interest standard is not applied for neonatal resuscitation decisions. Pediatrics 2008;121 (5):963–969
10.Janvier A, Barrington KJ. The ethics of neonatal resuscitation at the margins of viability: informed consent and outcomes. J Pediatr 2005;147(5):579–585
11.Anvier A, Barrington KJ, Desche?nes M, Couture E, Nadeau S, Lantos J. Relationship between site of training and residents’ attitudes about neonatal resuscitation. Arch Pediatr Adolesc Med 2008;162(6): 532–537
12.Partridge JC, Freeman H, Weiss E, Martinez AM. Delivery room resuscitation decisions for extremely low birthweight infants in California. J Perinatol 2001;21(1):27–33