A Novel Technique Treating Intra- Articular Calcaneal Fractures with Minimally Invasive Approach using Vertebral Body Stenting System Vbs
A Novel Technique Treating Intra- Articular Calcaneal Fractures with Minimally Invasive Approach using Vertebral Body Stenting System Vbs
Dr.Talal Almalki, Dr.Norah Almusallam
*Correspondence to: Dr.Talal Almalki, Saudi Arabia.
Copyright
© 2023: Dr.Talal Almalki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 December 2023
Published: 30 December 2023
DOI: https://doi.org/10.5281/zenodo.10444021
Abstract
Displaced intra-articular calcaneal fractures pose significant challenges due to their complex anatomy and potential complications associated with traditional open reduction and internal fixation (ORIF). Minimally invasive techniques have emerged as promising alternatives, but achieving anatomical reduction and stable internal fixation remains a hurdle. Here we present a novel minimally invasive approach utilizing the Vertebral Body Stenting System (VBS) for treating a displaced intra-articular calcaneal fracture. A 49-year-old male with a Sanders type IV fracture underwent a minimally invasive percutaneous lateral approach. Fracture fragments were reduced under fluoroscopy using periosteal elevator, K-wires, and a Steinmann pin. An inflatable VBS was introduced into the fracture gap and expanded to achieve reduction and restore the crucial angle of Gissane. Radiopaque cement was injected to fill the void and provide additional stability. Postoperative imaging demonstrated good anatomical reduction and restoration of the crucial angle. At two months follow-up, the patient had no pain, good functional outcomes, and was weight-bearing without limitations. This case report presents the successful application of a minimally invasive VBS technique for treating a displaced intra-articular calcaneal fracture. This approach offers potential benefits of reduced soft tissue disruption, adequate fracture reduction, internal support without bulky hardware, and potentially faster recovery. While further research is necessary to evaluate long-term outcomes, this case highlights the promising potential of VBS for managing complex calcaneal fractures.
Keywords: Calcaneal fracture, Minimally invasive, Vertebral Body Stenting System, VBS, Intra-articular, Reduction, Crucial angle, Case report.
A Novel Technique Treating Intra- Articular Calcaneal Fractures with Minimally Invasive Approach using Vertebral Body Stenting System Vbs
Introduction
Displaced intra-articular calcaneal fractures present a significant challenge due to complex anatomy and potential complications associated with traditional open reduction and internal fixation (ORIF). Minimally invasive techniques have emerged as promising alternatives, offering benefits like reduced soft tissue dissection, faster recovery, and earlier weight-bearing. Calcaneus fractures accounts approximately up to 2% of all fractures. A displaced intra-articular fracture constitutes up to 75% of calcaneus fractures and it represents about 60 % of all tarsal fractures in adults. [1]
Treating displaced intra-articular fractures of the calcaneus remains an obstacle for the orthopaedic surgeons. The impact of conservative management on functional status is widely acknowledged. Problems with soft tissues and insufficient reduction of fractures impede the surgical technique [2].
The use of percutaneously placed axial pins for the reduction of calcaneal fractures was first described in 1934 by Westheus [3]. Minimally invasive approaches for displaced intra- articular calcaneal fractures have been increasingly described recently. These techniques are associated with less soft tissue dissection and surgical complications when compared with extensile approaches, and allow for earlier return to activity, weight bearing and good functional outcomes. To allow for a better manipulation of the fracture, minimally invasive technique is considered as a better option to be obtained within the first two weeks of injury as the fragments are still not consolidated and this will result with an effective manipulation of the fracture fragments [4].
A minimally invasive method approach that should help with these issues is discussed in our case report.
Case Presentation
A 49-year-old male with a history of tobacco smoking, presented to our institution one week after sustaining a fall from a height of one meter, landing directly on his left heel. His primary complaint was significant left foot pain. He had previously sought treatment at another hospital, but desired a second opinion.
On initial presentation, the patient wore a below-knee backslab. Upon removal, moderate swelling and ecchymosis were evident over the left medial ankle and foot. Notably, fracture blisters and open wounds were absent. Comprehensive physical examination revealed no signs or symptoms of compartment syndrome. Pulses and neurological status were intact. Importantly, the "wrinkle sign" was not yet present, indicating that the soft tissue condition was not yet optimal for surgical intervention.
Therefore, the patient was managed conservatively with ice therapy, elevation, and re-application of the backslab to facilitate soft tissue swelling reduction and pain management.
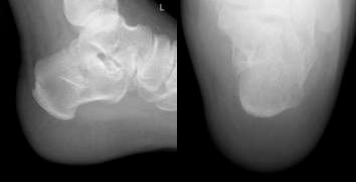
Radiographic assessment confirmed the diagnosis of an intra-articular calcaneal fracture. This was characterized by disruption of the Bohler angle and an increase in the Gissane angle, suggestive of posterior facet height loss (Figures 1 and 2). No extension into the calcaneocuboid joint was identified.
CT Findings
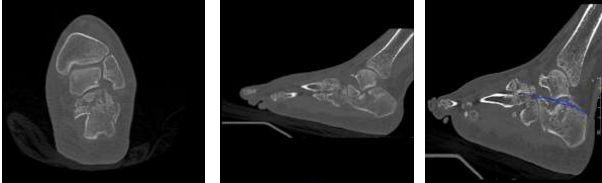
A computed tomography (CT) scan was performed to delineate the precise fracture anatomy, classify the fracture pattern according to the Sanders system, and inform treatment strategy.
The CT images revealed a Sanders type IV fracture, characterized by three fracture lines and four main posterior facet fragments (Figures 3 and 4). This complex fracture pattern demonstrates disruption of both the intra-articular and extra-articular components of the calcaneus. Furthermore, the crucial angle of Gissane measured approximately 165 degrees (Figure 5). This value significantly exceeds the normal range of 115-145 degrees, indicating significant posterior facet height loss and a potential for compromised joint congruity and long-term functional outcomes.
Surgical Technique
One week following the initial presentation, the patient underwent a planned surgical procedure for definitive fracture reduction and stabilization. A minimally invasive approach, carefully weighed against the potential benefits of open reduction, was chosen due to the anticipated advantages in terms of soft tissue preservation and faster recovery.
The patient was positioned supine on a radiolucent table, facilitating fluoroscopic imaging throughout the procedure. Spinal anesthesia was administered, ensuring adequate analgesia while maintaining patient cooperation. A sandbag was placed under the left hip to optimize surgical exposure and access to the fracture site. Prior to draping, meticulous verification confirmed that patient positioning did not restrict fluoroscopic visualization angles.
Prophylactic antibiotic administration (Cefazolin 2 g IV) was initiated on the operating table to prevent potential surgical site infections. Standard sterile draping and preparation protocols were followed to ensure a sterile surgical field.
Reduction Technique
The minimally invasive fracture reduction employed a meticulous sequence of maneuvers to achieve optimal anatomical restoration. Initial reduction of the lateral and medial walls of the calcaneus was facilitated using pelvic reduction clamp over a soft tissue protection. This maneuver enabled us to reduce the blowout lateral wall which was evaluated by fluoroscopic guidance. Following lateral wall reduction, a single Steinmann pin was employed to maintain the alignment and act as a "joystick" for further adjustments. The pin was inserted medially and advanced laterally in the most posterior part of the calcaneus away from fracture to effectively restore the calcaneal length. A Steinmann pin holder provided additional control during this maneuver to prevent varus. To address the posterior facet depression, a small (approximately 1 cm) lateral stab incision was created. An AO periosteal elevator was then introduced through the fracture gap, ensuring minimal soft tissue disruption. This instrument facilitated mobilizing the fragments and elevation of the depressed posterior facet fragment, restoring its anatomical position. After elevation of the facet and reducing the crucial angle of Gissane, gap was created and before introducing the stent four Kirschner wires (K-wires) was strategically placed at the inferior part of the defect from medial to lateral in one row, the purpose was to introduce the stent above it and during inflation to direct the force only upward to reduce and hold the posterior facet in its anatomic position. An intraoperative X-ray confirmed the preliminary reduction and restoration of the crucial angle of Gissane closer to the normal range.
Introducing the Vertebral Body Stenting System (VBS) for Intra-Articular Calcaneal Fracture Reduction:
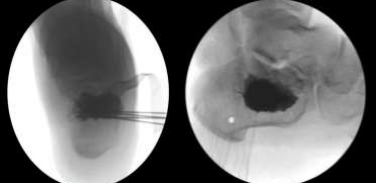
To further stabilize the fracture and maintain the restored articular congruity, the minimally invasive procedure incorporated the use of Vertebral Body Stenting System (VBS) from DePuy Synthes. Then 4 K-wires was introduced from lateral to medial at the inferior part of the created gap to prevent inferior displacement of the stent. Through the previously created lateral stab incision, a medium-sized Vertebral Body Stent with Balloon was introduced into the fracture void. This pre-inflated stent, with a maximum volume of 4.5 ml and maximum inflation pressure of 30 ATM, served as a crucial tool for both reduction and internal support. Inflation proceeded under fluoroscopic guidance, gradually increasing pressure until an appropriate resistance was encountered at around 20 ATM (Figure 7). The inflated stent acted as a highly effective reduction tool. Its expandable nature compacted the softer inner bone within the calcaneus, simultaneously creating a void space and elevating the depressed posterior facet fragment back to its anatomical position (Figures 9, 10, 11, and 12). This restoration of height and improved articular surface alignment contributed significantly to fracture stabilization were the inferiorly placed K-wires prevented downforce. Following successful VBS deployment, and stent visualization to be holding the reduction radiopaque, injectable polymethyl methacrylate cement (VERTECEM V+ CEMENT KIT) from DePuy Synthes was utilized as a void-filling agent. Under fluoroscopic control, 4 ml of cement (2 syringes) were injected into the newly created cavity within the calcaneus (Figure 8). This cemented augmentation provided additional stability and maintained the fracture reduction. After a ten-minute cement curing period, the temporary Kirschner wires were safely removed. The surgical site was meticulously closed, dressed, and supported with a below-knee backslab for additional immobilization. Final intraoperative radiographs confirmed satisfactory reduction, restoration of the crucial angle of Gissane, and appropriate cement distribution (Figures 13 and 14).
Postoperative Care and Optimizing Recovery and Monitoring Outcomes
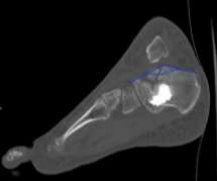
Following the minimally invasive procedure, the patient's care focused on optimizing recovery and preventing potential complications. Thromboembolic prophylaxis with anticoagulants was resumed 12 hours postoperatively, Patient did not require much pain control and he was discharged home on the first postoperative day. Strict non-weight bearing on the left lower limb was enforced for the initial two weeks to allow for undisturbed fracture healing and soft tissue recovery. Regular follow-up appointments were scheduled within the orthopedic foot and ankle clinic to monitor progress and address any emerging concerns. Thromboembolic prophylaxis with Enoxaparin (40 mg once daily subcutaneously) was continued for two weeks following discharge. The dressing clinic visit within the first week confirmed no signs of infection or complications. Suture removal was performed at the two-week mark, revealing a well-healed wound with no soft tissue issues. After the initial non-weight bearing period, the patient progressed to partial weight bearing for gradual return to mobility. Follow-up radiographs (Figures 15, 16, and 17) were obtained to assess fracture alignment and stability. Additionally, a CT scan was performed within three weeks postoperatively (Figures 18, 19, 20, and 21) for in-depth evaluation of the internal components and fracture healing process. The crucial angle of Gissane on the follow-up CT scan measured approximately 145 degrees (Figure 22), indicating near-anatomical restoration of the posterior facet and a significant improvement from the initial measurements. Overall, the patient's postoperative course was uneventful, with no reported complications or concerns. Continued follow-up appointments and imaging at scheduled intervals will be crucial to monitor long-term fracture healing, maintain optimal outcomes, and address any potential issues that may arise.
The calcaneus plays a crucial role in weight bearing, gait, and mobility, contributing significantly to 80% of total body weight distribution. Achieving an anatomically congruent subtalar joint is paramount for restoring optimal hind foot and ankle function. Displaced intra-articular calcaneal fractures, however, present a complex challenge due to their potential to cause long-term disability, chronic pain, and impaired functional outcomes [5].
Treatment strategies for these fractures remain a topic of debate, with both conservative and surgical approaches employed. Traditionally, open reduction and internal fixation (ORIF) combined with primary subtalar arthrodesis was the gold standard, achieving good-to-excellent outcomes in 60-85% of cases [9, 10,11]. However, concerns regarding extensive soft tissue dissection, hardware complications, and potential for iatrogenic neurovascular injury have prompted exploration of alternative techniques like sinus tarsi approach, nevertheless some articles in literature addressing the MIS approach to treated these notorious fractures. The use of vertebroplasty balloons have been mentioned but very seldom and was not popularized. This case report presents a novel application of the Vertebral Body Stenting System (VBS) and not only the balloon which in our opinion significantly improve the reduction especially with the inferior buttressing with K-Wires. We believe the VBS, which was originally designed for spinal stabilization in osteoporotic or acute vertebral body fractures, offers several advantages over traditional ORIF in calcaneal fractures. Furthermore, percutaneous access reduces soft tissue disruption, potentially minimizing wound healing complications, infection risk, and pain. The VBS's expandable stent facilitates targeted manipulation of fracture fragments under fluoroscopic guidance, allowing for accurate restoration of the articular surface. The stent provides internal stability without bulky implants, reducing the risk of hardware-related complications like migration or loosening. Minimized soft tissue disruption and reduced surgical trauma may contribute to faster recovery and earlier weight-bearing.
While literature on this new technique remains limited, initial reports from Gupta et al. [16] and Jacquot and Atchabahian [17] demonstrate promising outcomes in terms of bone healing and complication rates. But to our knowledge no other case was discussing the used of the stunting system compared to balloon only and non was utilizing the inferior K-wire buttressing.
Future Directions
Further research is warranted to evaluate the long-term efficacy and safety of the VBS technique for calcaneal fractures. Additionally, exploring alternative void-filling materials like calcium phosphate/sulfate bone substitutes instead of PMMA cement holds potential, particularly for younger patients, due to their favourable clinical and radiological profiles [18,19 ].
Important Practice Points from our Case Report
1.Minimal invasive VBS technique offers a promising alternative to traditional ORIF for displaced intra-articular calcaneal fractures. Percutaneous access minimizes soft tissue disruption, potentially leading to faster recovery, reduced pain, and lower risk of wound complications.
2.The VBS's expandable nature allows for targeted manipulation and adequate restoration of the articular surface under fluoroscopic guidance. This precise reduction is crucial for achieving optimal functional outcomes and minimizing long-term complications like post-traumatic arthritis.
3.The VBS provides internal stability without the need for extensive hardware, reducing the risk of hardware-related complications like migration or loosening. This may contribute to improved long-term implant survivorship and potentially facilitate future hardware removal if desired.
4.Minimized surgical trauma and soft tissue disruption associated with the VBS technique may lead to faster recovery, less pain, lower complications, less OR time, less expensive and earlier weight-bearing compared to traditional ORIF, which can significantly improve patient quality of life and functional outcomes.
5.Further research is necessary to evaluate the long-term efficacy and safety of the VBS technique for calcaneal fractures. Exploring alternative void-filling materials like calcium phosphate/sulfate bone substitutes holds potential, especially for younger patients, due to their favorable clinical and radiological profiles.
Conclusion
A novel minimally invasive VBS technique “stinting” successfully treated a displaced intra-articular calcaneal fracture in our patient. This approach offers reduced tissue disruption, adequate reduction, and internal support without bulky hardware, potentially leading to faster recovery. While further research is needed, this case highlights the promising potential of VBS in managing complex calcaneal fractures.
Reference
1. Bulut T, Gursoy M, Ozturk T, Ozcan C, Sener M. Sanders type 3-4 calcaneal fractures fixed with locking plate: does tri-cortical iliac bone autograft provide extra benefit for stabilization? Ther Clin Risk Manag. 2018 Sep 11;14:1665-1670. doi: 10.2147/TCRM.S146530. PMID: 30254447; PMCID: PMC6140723.
2.Ramos RR, de Castro Filho CD, Ramos RR, Bittar CK, de Cillo MS, de Mattos CA, Zabeu JL, Mazzuia AR. Surgical treatment of intra-articular calcaneal fractures: description of a technique using an adjustable uniplanar external fixator. Strategies Trauma Limb Reconstr. 2014 Nov;9(3):163-6. doi: 10.1007/s11751-014-0207-x. Epub 2014 Dec 25. PMID: 25540120; PMCID: PMC4278970.
3.Griffin D, Parsons N, Shaw E, Kulikov Y, Hutchinson C, Thorogood M, Lamb SE; UK Heel Fracture Trial Investigators. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014 Jul 24;349:g4483. doi: 10.1136/bmj.g4483. PMID: 25059747; PMCID: PMC4109620.
4.Sanders R. Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am. 2000 Feb;82(2):225-50. doi: 10.2106/00004623-200002000-00009. PMID: 10682732.
5.van Tetering EA, Buckley RE. Functional outcome (SF-36) of patients with displaced calcaneal fractures compared to SF-36 normative data. Foot Ankle Int. 2004 Oct;25(10):733-8. doi: 10.1177/107110070402501007. PMID: 15566705.
6.Poeze M, Verbruggen JP, Brink PR. The relationship between the outcome of operatively treated calcaneal fractures and institutional fracture load. A systematic review of the literature. J Bone Joint Surg Am. 2008 May;90(5):1013-21. doi: 10.2106/JBJS.G.00604. PMID: 18451393.
7Sharr PJ, Mangupli MM, Winson IG, Buckley RE. Current management options for displaced intra-articular calcaneal fractures: Non-operative, ORIF, minimally invasive reduction and fixation or primary ORIF and subtalar arthrodesis. A contemporary review. Foot Ankle Surg. 2016 Mar;22(1):1-8. doi: 10.1016/j.fas.2015.10.003. Epub 2015 Nov 21. PMID: 26869492.
8.Shervin N, Rubash HE, Katz JN. Orthopaedic procedure volume and patient outcomes: a systematic literature review. Clin Orthop Relat Res. 2007 Apr;457:35-41. doi: 10.1097/BLO.0b013e3180375514. PMID: 17415062.
9.Zwipp H, Rammelt S, Barthel S. Calcaneal fractures--open reduction and internal fixation (ORIF). Injury. 2004 Sep;35 Suppl 2:SB46-54. doi: 10.1016/j.injury.2004.07.011. PMID: 15315878.
10.Potter MQ, Nunley JA. Long-term functional outcomes after operative treatment for intra-articular fractures of the calcaneus. J Bone Joint Surg Am. 2009 Aug;91(8):1854-60. doi: 10.2106/JBJS.H.01475. PMID: 19651941.
11.Howard JL, Buckley R, McCormack R, Pate G, Leighton R, Petrie D, Galpin R. Complications following management of displaced intra-articular calcaneal fractures: a prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma. 2003 Apr;17(4):241-9. doi: 10.1097/00005131-200304000-00001. PMID: 12679683.
12.ESSEX-LOPRESTI P. The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg. 1952 Mar;39(157):395-419. doi: 10.1002/bjs.18003915704. PMID: 14925322.
13.PALMER I. The mechanism and treatment of fractures of the calcaneus; open reduction with the use of cancellous grafts. J Bone Joint Surg Am. 1948 Jan;30A(1):2-8. PMID: 18921620.
14.Robinson Y, Heyde CE, Försth P, Olerud C. Kyphoplasty in osteoporotic vertebral compression fractures--guidelines and technical considerations. J Orthop Surg Res. 2011 Aug 19;6:43. doi: 10.1186/1749-799X-6-43. PMID: 21854577; PMCID: PMC3170323.
15.Papanastassiou ID, Phillips FM, Van Meirhaeghe J, Berenson JR, Andersson GB, Chung G, Small BJ, Aghayev K, Vrionis FD. Comparing effects of kyphoplasty, vertebroplasty, and non-surgical management in a systematic review of randomized and non-randomized controlled studies. Eur Spine J. 2012 Sep;21(9):1826-43. doi: 10.1007/s00586-012-2314-z. Epub 2012 Apr 29. PMID: 22543412; PMCID: PMC3459114.
16.Gupta AK, Gluck GS, Parekh SG. Balloon reduction of displaced calcaneus fractures: surgical technique and case series. Foot Ankle Int. 2011 Feb;32(2):205-10. doi: 10.3113/FAI.2011.0205. PMID: 21288423.
17.Jacquot F, Atchabahian A. Balloon reduction and cement fixation in intra-articular calcaneal fractures: a percutaneous approach to intra-articular calcaneal fractures. Int Orthop. 2011 Jul;35(7):1007-14. doi: 10.1007/s00264-011-1249-z. Epub 2011 Mar 29. PMID: 21445550; PMCID: PMC3167396.
18.Bano A, Pasku D, Karantanas A, Alpantaki K, Souvatzis X, Katonis P. Intra-articular calcaneal fracture: closed reduction and balloon-assisted augmentation with calcium phosphate cement: a case report. Cases J. 2009 Dec 9;2:9290. doi: 10.1186/1757-1626-2-9290. PMID: 20062614; PMCID: PMC2803954.
19.Maestretti G, Sutter P, Monnard E, Ciarpaglini R, Wahl P, Hoogewoud H, Gautier E. A prospective study of percutaneous balloon kyphoplasty with calcium phosphate cement in traumatic vertebral fractures: 10-year results. Eur Spine J. 2014 Jun;23(6):1354-60. doi: 10.1007/s00586-014-3206-1. Epub 2014 Feb 9. PMID: 24509773.