Subdural Empyema in a Newly Born Child: (A Case Report)
Subdural Empyema in a Newly Born Child: (A Case Report)
Dr.Abdul-Rahim H.Zwayed (Ph.D.)*1, Dr.Sreenivas A.V2, Dr.Balola Miraghani3, Dr.Enas Hasan4, Dr.Amir M. Shabana5, Dr.Wajih K. Eshak6, Dr.Yasser Abdul Raziek7, Dr.Halima Mohammed Al Amri8, Dr.Ban F. Refaat9, Dr.Ibtisam Salim Al Hamdi10
1,2,3,4. Department of Neurosurgery.
5,6 Anaesthesia.
7,8 Radiolog.
9,10. Paediatrics. Sohar Hospital, Sultanate of Oman
*Correspondence to: Dr.Abdul-Rahim H.Zwayed (Ph.D.) Department of Neurosurgery.
Email:abdulrahimns95@gmail.com
Copyright
© 2023 Dr.Abdul-Rahim H.Zwayed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 December 2023
Published: 01 January 2024
DOI:https://doi.org/10.5281/zenodo.10487352
Subdural Empyema in a Newly Born Child: (A Case Report)
Introduction
Subdural empyema is a collection of pus in the space between the dura and arachnoid, it is a rare type of intracranial infection.
We report a case aged 1 month, with subdural empyema, the presentation was focal neurologic deficit, fever, vomiting, and seizures. Diagnosis was achieved by neurologic examinations and computerized tomography.
Treatment was done by burr hole and antibiotics were administered. The patient made a good recovery without sequelae. We therefore recommend burr hole with catheter drainage plus antibiotics as a method of treating subdural empyema. We review previously published cases and highlight the uniqueness of the disease. The aim of this report is to discuss the clinical, radiological, and histological characteristics for optimal treatment of this rare case.
Keywords: Subdural, empyema, burr hole, newly born.
Case Report
One month-old term, female infant was brought to the paediatric emergency due to convulsion. The mother of child reported no history of trauma and no previous admission. No maternal risk of sepsis, she has history of fever (documented reaching more than 38.c) since 1 week, no chills, and no rigors.
History of irritability and excessive crying, with poor oral intake
First impression was as; severe dehydration, sepsis or meningo-encephalitis
On examination:
She was feverish, not in respiratory distress; pale, irritable, excessive crying mainly on manipulation, has lateralization of gaze to right side.
Pulse rate was =150 bt/mint, Blood pressure = 95/32 mmhg
Sunken anterior fontanel with reduced skin turger
Chest clear
The blood picture and biochemistry were within normal limits.
Head ultra sound reported as:
Brain parenchyma is grossly normal at exam time.
Cerebral ventricles are not dilated at exam time.
No evidence of intra cranial bleeding or midline shift
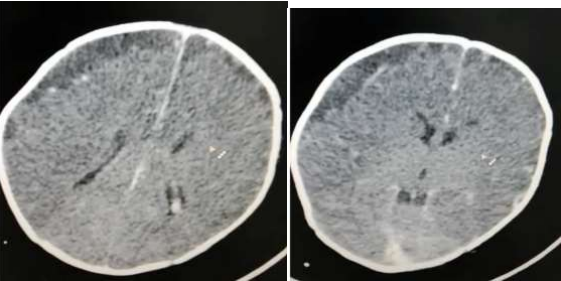
CT scan of the Head as in Fig 1:Showing: right frontal subdural collection which shows higher density than cerebrospinal fluid CSF density measuring 11 mm in maximum thickness displacing the cortical vein to the cortical outline with adjacent leptomeningeal enhancement more than contra lateral side which could represent infected fluid /abscess or hygroma.
Generalized reduced attenuation of cerebral brain parenchyma with less gray white matter differentiation in comparison to the cerebellum with white cerebellar sine which could be related to reduced brain parenchyma myelination at this age
However hypoxic ischemic injury is another most likely possibility
Fig 1: CT Head Showing: right frontal subdural collection
So urgent operation done as burr holes and aspiration of about 25 ml thick purulent material.
Fig 2: color of the aspirated subdural purulent material
We put a subdural drain and was left for 2 days as no more drainage with coverage of systemic antibiotics for 21 days.
The culture of the aspirated material showed growth of:
Streptococcus Agalactiae : sensitive to many antibiotics as; Ampicillin/Amoxicillin & clavulanic acid (Augmintin)/Cefotaxime,Ceftriaxone /Ciprofloxacin, Erythromycin, Penicillin ,and Clindamtycin.
We select Cefotaxime and was given according to recommended dose with his age and weight .
The patient was kept in the hospital until the completion of antibiotics then discharged in uneventful condition.
Discussion
Subdural empyema is a rare disease .In the literatures, only few cases have been reported and their ages much older than our case [4].
In this case report we present one month-old patient with a subdural empyema, arising in the left frontal region.
Subdural empyema (SE) is a life-threatening infection, because the symptoms might be very mild initially, so rapid recognition and treatment are important; the early initiation of appropriate treatment gives the patient a good chance of recovery with little or no neurological deficit.
A subdural empyema in an infant with no previous perinatal source of infection which causes his clinical problems through extrinsic compression on the brain and orbital contents by an inflammatory mass mimicking the presentation of a space occupying lesion is something rare.
About 95% of subdural empyemas are located within the cranium; most involve the frontal lobe, and 5% involve the spinal neuraxis. (2,7)
Subdural Empyema (SDE) is usually referred to an intracranial purulent material between the dura and arachnoid matter.
In infants and young children, SDE could be life threatening if not managed properly (10).The mortality rate of patients with SDE is around 4%, while the morbidity for survivors is even higher with residual neurologic deficits reaching up to 50%,hemiparesis 15-35% and persistent seizures 12-37.5% (6).
In infants and young children, SDE most often occurs as a complication of meningitis. In such cases, SDE should be differentiated from reactive subdural effusion (i.e. sterile collection of fluid due to increased efflux of intravascular fluids from increased capillary wall fenestrations into the subdural space).
In older children and adults, it occurs as a complication of paranasal sinusitis, otitis media, or mastoiditis.(3,11,13,17).
However, in older children, sinusitis and otitis media are the most common sources (17). If the source of SDE is sinusitis, then the frontal sinus is the most common culprit followed by the ethmoid, sphenoid, and maxillary sinuses (8). The infection is spread from the paranasal sinuses to the subdural space through bone erosion or takes the haematogenous route (9). It has been reported that lumbar puncture might lead to spinal SDE (7). Other causes of SDE are iatrogenic such as subdural hematoma drainage, craniotomy and intracranial pressure monitoring (13).
SDE is a primarily intracranial infection located between the dura mater and the arachnoid mater. It has a tendency to spread rapidly through the subdural space until limited by specific boundaries (e.g., falx cerebri, tentorium cerebelli, base of the brain, foramen magnum). The subdural space has no septations except in areas where arachnoid granulations are attached to the dura mater. SDE is usually unilateral. (2,11)
With progression, SDE has a tendency to behave like an expanding mass lesion with associated increased intracranial pressure (I.C.P.) and cerebral intra-parenchymal penetration. Cerebral edema and hydrocephalus also may be present secondary to disruption of blood flow or cerebrospinal fluid (CSF) flow caused by the increased ICP.Cerebral infarction may be present from thrombosis of the cortical veins or cavernous sinuses or from septic venous thrombosis of contiguous veins in the area of the SDE.(1,12).
Infants and young children with SDE might present with altered mental status, meningeal irritation, and/or signs and symptoms of intracranial pressure. Some studies showed that 40% of patients with SDE present with seizures (16).
Bacterial meningitis is considered a major source of SDE in infants and cerebro spinal fluid CSF culture is the “gold standard” for the diagnosis.(14).
There are many pathogens that can cause SDE and it depends on the route of the infection as well as the age of the patient. Enterobacteriace, Group B streptococci or Listeria monocytogenes are usually the cause of SDE in neonates with meningitis
C-reactive protein, erythrocyte sedimentation rate, and white blood cell count are usually elevated in patients with SDE. In addition, it has been reported that diabetes or hyperglycemia are risk factors for intracranial empyemas (5).
CSF examination is an adjunctive test in the diagnosis of SDE and may be obtained in addition to the other diagnostic tests previously outlined.
CSF findings include the following:
WBC count (predominantly polymorphonuclear neutrophils) is increased.
A significant increase (>50/mm3) may be seen, although a slightly elevated cell count of 5-20 per cubic millimeter (reference range, 0-5/mm3) does not rule out the possibility of SDE.
Increased protein level greater than 100 mg/dL may be seen (reference range, 20-40 mg/dL), although less substantial elevations (50-90 mg/dL) do not rule out the possibility of SDE. (15,19)
Decreased glucose levels of 40 mg/dL or less usually are seen (reference range, 50-80 mg/dL). CSF glucose levels should be normalized with a blood glucose level obtained concurrently. Occasionally, the CSF is normal and sterile in these cases. The specific CSF findings should be compared with the accepted normal values of the treating physician's laboratory (18,19)
Imaging of the head is recommended for every patient suspected of having SDE.Cranial ultrasonography is usually the first imaging mode to be ordered in infants because it is safe, cost-effective, and it usually differentiates subdural empyema from subdural effusion (11).
Cranial CT scan was the standard technique for quick diagnosis before the advent of MRI. The use of high-resolution, contrast-enhanced CT scan increases diagnostic yield, although it sometimes gives equivocal or normal results.(1,20)
Computed Tomography (CT) of the head is considered cost-effective and accessible. However, it can be normal in up to 50% in patients with SDE (11). When using CT as an imaging modality, SDE will appear crescentic in shape over the cerebral convexity with a surrounding rim that is enhanced with the use of contrast (20).
Magnetic resonance imaging (MRI) has a sensitivity of 93% (12), and is considered the best imaging mode for SDE because it usually portrays clearly the collections, and reveals signs of meningeal infections. However, MRI machines are not available in every health care setting and it could delay the urgent interventions (11).
Conservative treatment is recommended for patients with non-focal neurological deficits, no changes in mental status, empyema is limited and localized except the posterior fossa, and if the response to antibiotics is adequate. However, following the conservative approach will require frequent imaging to follow up on the SDE (9).
Another school that advocates conservative management indicates that patients who respond well clinically as well as radiographically, antibiotics alone suffice; otherwise neurosurgical intervention is warranted (10).
If the organism is unknown, then Cloxacillin plus ceftriaxone/cefotaxime plus metronidazole is recommended; however, if there is a suspicion for methicillin-resistant Staph. aureus, then vancomycin instead of cloxacillin is warranted (9). Linezolid is an alternative treatment in case of conventional antibiotic regimen failure (9).
As far as the duration of antibiotic treatment, it differs among practices. For instance one of the practices recommends at least two weeks through the intravenous route, followed by six weeks of oral therapy.
The second practice states that intravenous route should be for six weeks followed by an oral course of four to six weeks (6). Intravenous steroids use has been advocated due to its function in reducing edema, swelling and inflammation (9).
Depending on the presentation, lowering intracranial pressure might be required with modalities like elevation of the head, Mannitol or Ventriculostomy (12). Anti-seizure medications are recommended as prophylaxis because of the high rate of seizures associated with SDE (12).
Regarding the duration of therapy, there are different schools: some advocate for the treatment only during the acute phase of disease, others prefer indefinitely and the rest prefer to discontinue the anticonvulsants once the patient is seizure free for at least two years (9).
The two most surgical procedures that have been conducted for SDE are craniotomy and burr holes. There is a consensus that Burr hole compared to craniotomy has a higher rate of SDE recurrence (7, 9, 11)
However, one study showed that there was no difference between the two modalities in terms of recurrence rate, antibiotic therapy duration, neurological outcome and complications (10).
Craniotomy is considered as the technique of choice because it allows complete evacuation of the empyema, and it decompresses the underlying cerebral hemisphere (1). However, bridging veins injury might be a complication of craniotomy (13).
There are situations were burr holes are recommended over craniotomy like patients with septic shock or with parafalcine empyemas (1). Other indications for burr holes use include emergency situations or if the patient is considered frail (7).
The disadvantages of Burr Hole are that the technique is not optimal for multi-loculated subdural collections and that can lead to secondary injury of the cortex and therefore might exacerbate infections (1).
Stereotactic burr hole placement with drainage and irrigation is another option but is less desirable because of decreased exposure and possible incomplete evacuation of the purulent material.(5,6,14)
In terms of surgical intervention, there is a consensus that the mortality rate is 28% in patients with SDE, 23.3 % if burr holes technique is used and 8.4 to 11.5 % if craniotomy or craniectomy is performed (7).
Some surgeons use functional endoscopic sinus surgery (FESS) since it might aid in drainage and recovery (12), and others conduct percutaneous needle aspiration of SDE via the fontanelle in infants (7).
Neurological deficits and cerebral herniation on CT scan are indicators of poor prognosis in patients with SDE (9).
Nowadays, the survival rate for children with SDE is more than 90% if surgical intervention was done on timely basis (19).
The mortality rate has continued to decline because of early diagnosis and treatment,more accurate localization with head CT scan,early sinus drainage, and recognition of the prominent role of anaerobes in the disease. (13)
In the developed world, the mortality rate has improved tremendously: it is about 6-35% variance depending on areas and hospitals); however, about 55% of patients have neurological deficits at the time of hospital discharge (13,15,17)
Rate of disability due to SDE depends of the timing of the surgical intervention (if needed). If the intervention is done within 72 hours of symptoms the chance of disability is 10%, while the probability increases to 70% if the surgery is conducted after 72 hours. The health care provider has to have an ethical responsibility in counseling patients to be compliant with the antibiotics as well as with the anticonvulsants
Conclusion
Subdural empyema is a rare condition, denotes the collection of purulent material in the subdural space and is commonly seen in infants and older children
In infants, the most common cause is bacterial meningitis.
The clinical symptomatology is varied and has a wide range including prolonged or recurrent fever, seizures, meningeal irritation, and raised intracranial pressure.
It can mimic as well as complicate meningitis and heightened clinical awareness is therefore paramount.
SDE regarded as a neurosurgical emergency, so rapid recognition and treatment can avoid life-threatening complications.
Diagnosis was achieved by neurologic examinations and computerized tomography.
Conservative management with antibiotics and follow up imaging is recommended if there are no focal deficits, change in mental status or if the patient is responding well to antibiotics.
Alternatively, craniotomy is warranted in addition to antibiotics therapy. The surgeon might opt for burr holes in case the patient is frail or in septic shock and antibiotics course.
We therefore recommend burr hole with catheter drainage plus antibiotics as a method of treating subdural empyema and necessary for a delightful outcome
References
1.Adame N, Hedlund G, Byington C. L. Sinogenic intracranial empyema in children. Pediatrics. 2005;116:461–467.[PubMed]
2.Agrawal A, Timothy J, Pandit L,Shetty J. P. A Review of Subdural Empyema and Its Management. Infectious Diseases in Clinical Practice. 2007;15(3):149–153.
3.Aldinger F. A, Shiban E, Gempt J, Hollow screws: a diagnostic tool for intracranial empyema. Acta Neurochir (Wien) 2013;155(2):373–7. http://dx.doi.org/10.1007/s00701-012-1581-0 . [Pub Med]
4.Banerjee A. D, Pandey P, Devi B. I, A. Pediatric supratentorial subdural empyemas: a retrospective analysis of 65 cases. Pediatr Neurosurg. 2009;45(1):11–8.
http://dx.doi.org/10.1159/000202619 . [PubMed]
5.Bouziri A, Khaldi A, Smaoui H, Menif K, Fatal subdural empyema caused by Streptococcus constellatus and Actinomyces viscosus in a child. Journal of Microbiology, Immunology and Infection. 2011;44:394–396 http://dx.doi.org/10.1016/j.jmii.2010.03.002 . [PubMed]
6.Bruner D. I, Littlejohn L, Pritchard A. Subdural Empyema Presenting with Seizure, Confusion, and Focal Weakness. Western Journal of Emergency Medicine. 2012;13(6):509–511
http://dx.doi.org/10.5811/westjem.2012.5.11727 . [PubMed]
7.Chen CY, Huang CC, Chang YC: Subdural empyema in 10 infants: US characteristics and clinical correlates. Radiology 1998 Jun; 207(3):609-17
8.De Bonis P, Anile C, Pompucci A, Cranial and spinal subdural empyema. Br J Neurosurg. 2009;23(3):335–340. http://dx.doi.org/10.1080/02688690902939902 . [PubMed]
9.Farah J. O, Kandasamy J, May P, Buxton N, . Subdural empyema secondary to sinus infection in children. Childs Nerv Syst. 2009;25:199–205 http://dx.doi.org/10.1007/s00381-008-0665-x . [PubMed]
10.Feuerman T, Wackym PA, Gade GF: Craniotomy improves outcome in subdural empyema. Surg Neurol 1989 Aug; 32(2): 105-10
11. Gupta S, Vachhrajani S, Kulkarni A. V, Neurosurgical management of extra axial central nervous system infections in children. J Neurosurg Pediatr. 2011;7(5):441–451. http://dx.doi.org/10.3171/2011.2.PEDS09500 . [PubMed]
12. Kapu R, Pande A, Vasudevan M. C. Primary inter hemispheric subdural empyemas: A report of three cases and review of literature. Indian Journal of Neurosurgery. 2013;2(1):66–70.
13. Lefebvre L, Metellus P, Dufour H, . Linezolid for treatment of subdural empyema due to Streptococcus: case reports. Surgical Neurology. 2009;71(1):89– 91 http://dx.doi.org/10.1016/j.surneu.2007.06.083 .
14. Liu Z. H, Chen N. Y, Tu P. H, . The treatment and outcome of postmeningitic subdural empyema in infants. Neurosurg Pediatrics. 2010;6:38–42 http://dx.doi.org/10.3171/2010.4.PEDS09433 . [PubMed]
15. Mat Nayan S. A, Mohd Haspani M. S, Abd Latiff A. Z. Two surgical methods used in 90 patients with intracranial subdural empyema. J ClinNeurosci,2009:16(12) :1567–71. http://dx.doi.org/10.1016/j.jocn.2009.01.036 . [PubMed]
16. Mauser HW, Van Houwelingen HC, Tulleken CA: Factors affecting the outcome in subdural empyema. J Neuro Neurosurg Psychiatry. 1987; 50: 1136-41.
17. Nathoo N, Nadvi S. S, Gouws E, . Craniotomy improves outcomes for cranial empyema in computed tomography era experience with 699 patients. Neurosurg. 2001;49:872–8. [PubMed]
18. Sucu N, Koksal I, Aksoy F, . Subdural Empyema due to Streptococcus constellatus. Ann Neurosurg. 2006;6(2):1–4.
19. Wu T. J, Chiu N. C, Huang F. Y. Subdural empyema in children —20-year experience in a medical center. J Microbiol Immunol Infect. 2008;41:62–67. [PubMed]
20. Zimmerman RD, Leeds NE, Danziger A: Subdural empyema: CT findings.Radiology 1984 Feb; 150(2): 417-22