Juvenile Mandibular Chronic Osteomyelitis- A Rare Case Report
Juvenile Mandibular Chronic Osteomyelitis- A Rare Case Report
Dr. Bansari Kartik Patel 1, Dr. Abhilash Panwar* 2, Dr. Dola Rama Venkata Kumar 3, Dr. Nagaraju Kamarthi 4
1. Dr. Bansari Kartik Patel, BDS, Pacific Dental College.
2. Dr. Abhilash Panwar, Postgraduate student, Department of Oral Medicine and Radiology, Subharti Dental College and Hospital.
3. Dr. Dola Rama Venkata Kumar, Professor, Pacific Dental College.
4. Dr. Nagaraju Kamarthi, MDS, Professor and Head, Department of Oral Medicine and Radiology, Subharti Dental College and Hospital.
*Correspondence to: Dr. Abhilash Panwar, Postgraduate student,Department of Oral Medicine and Radiology, Subharti Dental College and Hospital, Swami Vivekanand Subharti University, Meerut.
E-mail id: panwarabhilash@gmail.com.
Copyright
© 2024 Dr. Abhilash Panwar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 December 2023
Published: 05 January 2024
Abstract
A rare, idiopathic condition characterized by persistent bone inflammation without suppuration, sinus tract development, or sequestration is known as juvenile mandibular chronic osteomyelitis (JMCO). As the name implies, children are primarily affected by this illness. There is currently no recognized standard therapy procedure for JMCO, as the few cases that have been documented in the literature have been associated with various treatments. The purpose of this study is to present a clinical example of an eight-year-old child who had an incorrect diagnosis and ineffective treatment. Following the onset of persistent symptoms, a proper diagnosis was made based on the physical and radiographic examinations, as well as the effectiveness of the non-steroidal anti-inflammatory drug (NSAID) treatment. During a four-month follow-up period, the patient received medication therapy followed by intervals of remission. Given the condition's rarity and non-specific signs and symptoms, diagnosing and treating JMCO can be difficult. For these people, NSAIDs and regular follow-up are a safe alternative.
Keywords: Disease, Mandibular, Diagnoses and Examinations, Children
Juvenile Mandibular Chronic Osteomyelitis- A Rare Case Report
Introduction
An inflammatory condition known as osteomyelitis of the jaws is typically brought on by an odontogenic infection. Primary chronic osteomyelitis, sometimes known as juvenile mandibular chronic osteomyelitis (JMCO), is a rare non-suppurative form of chronic bone infection that does not manifest as sinus tract formation or bone sequestration.
JMCO doesn't have an acute phase and develops slowly. Rather, there are sporadic, variable-intensity signs and symptoms that persist for a few days to several weeks. Reduced mouth opening, severe mandibular swelling, and regional lymphadenopathy are among the warning signs and symptoms. Imaging, such as computed tomography, magnetic resonance imaging, conventional radiography, and bone scintigraphy, is used to support the diagnosis. In light of the infrequency of this condition and the difficulties associated with diagnosis and clinical care, we present the case of an 8-year-old girl who was well-managed.
Case Report
An 8-year-old girl was reported to the Department of Oral Medicine and Radiology, Subharti Dental Hospital with a chief complaint of pain and mild swelling in the right side of her tooth region for 1 year. The patient had previously been diagnosed with mumps and treated accordingly, but the discomfort and swelling had not subsided.
On extra-oral evaluation, mild swelling was seen on the right side of the face, and pain on palpation was present on the right side (Figure 1). No cervical lymph node enlargement was noted. Intra-orally, reduced mouth opening and slight enlargement of the right mandibular ramus were appreciated. The surface mucosa of the ramus was intact and normal in coloration. No carious lesions of the dentition were observed.
After being recommended for a hematological investigation, the patient's total blood count was found to be within normal ranges. Subsequently, the patient underwent a Mantoux test to rule out tuberculosis (TB), but the results also seemed unreactive.
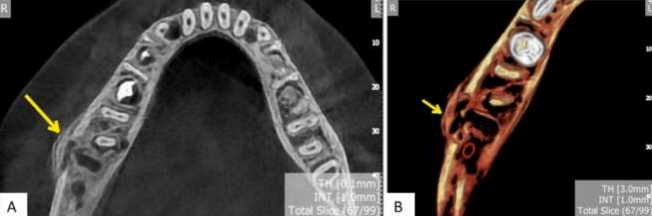
After the patient underwent additional cone beam computed tomography (CBCT) scans, the results showed many osteolytic lesions (moth-eaten) in the right mandible's ramus and body (Figure 2). It was noticed that the lesions ranged in definition from well-defined to ill-defined, and there was noticeable cortical duplication (onion peel appearance) (Figure 3).
JMCO was diagnosed based on the patient's prior history, imaging scans, and clinical presentation. The patient was given 50 mg of indomethacin every day. After one month, the clinical state improved, and the NSAIDs were withdrawn. Before the discomfort and swelling reappeared, the patient was asymptomatic for one week. The therapeutic regimen was restarted, but there was no improvement. The dose was changed to 100 mg/day and then increased to 150 mg/day. Hematological tests were performed regularly and yielded normal results. Continuous monitoring was performed, and the patient has been symptom-free for four months without medicine.
Figure 1, Figure 2, Figure 3
Discussion
JMCO has an unknown etiology, and patients typically have no infection, suppuration, sinus tract, or bone sequestra [1]. In our case, the patient maintained good dental hygiene. Due to similar clinical symptoms, patients with JMCO are frequently misdiagnosed with juvenile recurrent parotitis [2]. JMCO diagnosis and treatment continue to be difficult because of its rarity, nonspecific indications and symptoms, and a lack of evidence-based therapeutic procedures.
JMCO typically affects only one side of the jaw, with normal skin and mucosa covering the afflicted bone [3]. When many bones are involved, the illness is known as chronic recurrent multiple osteomyelitis (CRMO), and it exhibits the same clinical, radiological, and histopathologic features as JMCO. Bone scans in CRMO instances demonstrate hyperactive foci of skeletal bone, which can aid in diagnosing [4].
Imaging tests are typically used to confirm the diagnosis of JMCO. Typical findings include mandibular enlargement and change in contour, lytic areas, enlargement of the mandibular nerve canal, partial destruction of the cortical-cancellous border, periosteal reaction, and a sclerotic, "ground glass appearance," or mixed radiopaque-radiolucent bone pattern [5]. Adjacent soft-tissue thickening is also common. The "ground glass" bone pattern frequently causes fibrous dysplasia (FD) to be considered in the differential diagnosis.
Obel et al. suggested that a JMCO diagnosis should follow the criteria adapted from Manson et al. which comprises: (1) at least 6 months of disease duration; (2) radiographic diagnosis of a mandibular bone lesion; (3) imaging tests showing osteomyelitis; (4) no identifiable cause; and (5) ineffective antibiotic therapy [6].
The histologic characteristics are described variably by different authors, although many involve the presence of an infiltrate of infected cells in the infected bone. Some features are comparable to those seen in FD, although this entity possesses metaplastic bone trabeculae, whereas JMCO has peripheral osteoblasts, bone marrow fibrosis, and new bone production [7].
Our patient's diagnosis was established based on results from the history, clinical presentation, and imaging. The successful NSAID treatment regimen also served as confirmation.
JMCO has been treated with a variety of methods. Although surgical treatments such as decortication have been recorded, conservative treatment is an appealing alternative strategy, particularly in young patients [7]. NSAID therapy, which was also successful for our patient, is the most effective recorded treatment. Some authors believe antibiotic therapy is ineffective, and our patient reported no detectable clinical effects. Interferons or, hyperbaric oxygen therapy, glucocorticoids, tumor necrosis factor neutralizing drugs, and bisphosphonates have been reported as effective therapies in CRMO and certain relapsing cases [8].
There have been no reports of specific NSAID therapies for the treatment of JMCO. Obel et al. published a case study in which three patients were effectively treated with ibuprofen 200 mg three times per day, with one patient adding oral steroids with this regimen [9]. Heggie et al. adopted indomethacin 75 mg/day to treat eight patients, seven of whom improved their symptoms and one of whom required surgical treatment [2], this suggests that the medicine dose should be modified based on the ongoing outcomes. When the pain and swelling reduce and bone structures seem normal in imaging investigations, the case is considered resolved.
Conclusion
JMCO is a difficult condition that should be treated separately from infectious osteomyelitis. There is no recognized treatment regimen because it is a rare illness with no known cause. We feel that NSAIDs should be used as the first-line treatment and that surgical methods should be avoided. JMCO treatment must be individualized to each patient, including follow-up visits to assess patient progress, the need for treatment modifications, and indicators of relapse.
References
1.Baltensperger M, Gratz K, Bruder E, Lebeda R, Makek M, Eyrich G. Is primary chronic osteomyelitis a uniform disease? Proposal of a classifcation based on a retrospective analysis of patients treated in the past 30 years. J Craniomaxillofac Surg. 2004;32:43–50.
2.Heggie AAC, Shand JM, Aldred MJ, Talacko AA. Juvenile mandibular chronic osteomyelitis: a distinct clinical entity. Int J Oral Maxillofac Surg. 2003;32:459–68.
3. Eyrich GKH, Baltensperger MM, Bruder E, Graetz KW. Primary chronic osteomyelitis in childhood and adolescence: a retrospective analysis of 11 cases and review of the literature. J Oral Maxillofac Surg. 2003;61:561–73.
4. Job-Deslandre C, Krebs S, Kahan A. Chronic recurrent multifocal osteomyelitis: fve-year outcomes in 14 pediatric cases. Joint Bone Spine. 2001;68:245–51.
5. Frid P, Tornes K, Nielsen Ø, Skaug N. Primary chronic osteomyelitis of the jaw—a microbial investigation using cultivation and DNA analysis: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:641–7.
6. Manson D, Wilmot DM, King S, Laxer RM. Physeal involvement in chronic recurrent multifocal osteomyelitis. Pediatr Radiol. 1989;20:76–9.
7. Berglund C, Ekstromer K, Abtahi J. Primary chronic osteomyelitis of the jaws in children: an update on pathophysiology, radiological fndings, treatment strategies, and prospective analysis of two cases. Case Rep Dent. 2015;2015:152717.
8. Yamazaki Y, Satoh C, Ishikawa M, Notani K, Nomura K, Kitagawa Y. Remarkable response of juvenile difuse sclerosing osteomyelitis of mandible to pamidronate. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:67–71.
9. Obel G, Krogdahl A, Thygesen T, Godballe C. Juvenile mandibular chronic osteomyelitis: 3 cases and a literature review. J Oral Maxillofac Surg. 2013;71:305–9.