A Modification of Curtis and Fisher Quadricepsplasty: An Effective Management Option for Debilitating Congenital Quadriceps Contracture and Associated Knee Dislocations
A Modification of Curtis and Fisher Quadricepsplasty: An Effective Management Option for Debilitating Congenital Quadriceps Contracture and Associated Knee Dislocations
Jawad ul haq (MBBS, FCPS Orthopedics)1, Imtiaz Muhammad (MBBS, FCPS Resident Orthopedics)2, Faisal Karim (MBBS, FCPS Orthopedics)3, Usama Ali Nawazish (MBBS, FCPS Orthopedics)4, Umair Nadeem (MBBS, FCPS Orthopedics)5, Zubair Khalid (MBBS, MRCS, FCPS Orthopedics)1, Muhammad Usama(MBBS, FCPS Resident Orthopedics)2 , Haseeb Elahi (MBBS, FCPS Orthopedics)6, Attique uz Zaman (MBBS, FCPS Orthopedics)7, Amer Aziz (FRCS (Ed), FRCS (Glasgow), FCPS (Orth),‘MSc (Oth) London, MCPS HPE)8.
1. Senior Registrar, Ghurki Trust Teaching Hospital, Lahore.
2. Resident, Ghurki Trust Teaching Hospital, Lahore.
3. Senior Registrar, Shalamar Hospital, Lahore
4. Senior Registrar, Indus Hospital, Lahore
5. Assistant Professor, Ghurki Trust Teaching Hospital, Lahore.
6. Spine Fellow, Ghurki Trust Teaching Hospital, Lahore.
7. Professor, Ghurki Trust Teaching Hospital, Lahore.
8. Professor, Head of the Department, Ghurki Trust Teaching Hospital, Lahore.
*Correspondence to: Dr. Jawad ul haq, Email: dr.jawadulhaq188@gmail.com Cell no: 00923434065067 Address: Computer office, Orthoopedics ward, Ghurki trust teaching hospital, Jallo More, Lahore.
Copyright
© 2023: Dr. Jawad ul haq. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 December 2023
Published: 05 January 2024
DOI: https://doi.org/10.5281/zenodo.10461009
Abstract
Background: Congenital deformity of joints is an uncommon complaint among infants brought to the pediatric orthopedics clinic: but if not managed properly, can result in disastrous sequalae. Among these is congenital dislocation of knee (CDK). In many of these cases, there are other associated anomalies as well like club foot, development dysplasia of hip (DDH), arthrogryposis multiplex congenita (AMC), myelodysplasia or Larsen syndrome. Objective: We aim to assess and report the results of the modified approach of Curtis and Fisher quadricepsplasty in terms of wound associated problems and postoperative functional improvement. Material and Methods: This study was conducted at Orthopedics unit of GTTH Lahore. It was a retrospective case series, that was approved by ethical committee of GTTH Lahore. The study stretched over a period of 3 months: from 1stJuly, 2023 to 30th September, 2023. Results: A total of 23 patients (31 knees) were assessed. Mean age of the sample was 28±5.402 months and mean follow-up period was 48.12±24.5 months. The mean preoperative ROM was 44.19±20.12 (18.54±13.67 extension to 25.64±12.36 flexion) and mean postoperative ROM was 103.38±29.25 (1.93±8.02 extension to 105.32±24.76 flexion). Thus, the improvement of 59.19±31.51 was noted and this improvement was statistically very highly significant (p<0.001). Assessment showed that 9 knees (29%) had excellent, 11 knees (35,5%) had good, 7 knees (22.6%) had fair and 4 (12.9%) had poor functional outcome. Conclusion: The inferential analysis has brought us to the conclusion that this technique achieves adequate and sustainable ROM at the knee; and has good functional outcome. Furthermore, this technique when adopted properly lowers rate of instability at knee as well as wound related complications.
Keywords: congenital dislocation of knee, congenital quadriceps contractures, arthrogryposis multiplex congenita, development dysplasia of hip
A Modification of Curtis and Fisher Quadricepsplasty: An Effective Management Option for Debilitating Congenital Quadriceps Contracture and Associated Knee Dislocations
Introduction
Congenital deformity of joints is an uncommon complaint among infants brought to the pediatric orthopedics clinic: but if not managed properly, can result in disastrous sequalae. Among these is congenital dislocation of knee (CDK): a rare deformity, reported in 0.017/1,000 live births. In many of these cases, there are other associated anomalies as well like club foot, development dysplasia of hip (DDH), arthrogryposis multiplex congenita (AMC), myelodysplasia or Larsen syndrome1.
What drives this deformity is a shortened and fibrotic quadricep femoris muscle. This impedes flexion at knee: leaving the joint unstable and useless. As is the general rule, an attempt towards correction of this pediatric deformity with casting should be made. But if these congenital quadriceps contractures (CQC) are not managed properly in the infantile period, they present with recalcitrant deformities that are not amenable to closed method of treatment. For operative management of CDK and CQC, literature has reported many techniques ranging from percutaneous techniques and mini-open tenotomies to formal open lengthening procedures.2 The quadriceps lengthening devised by Curtis and Fisher has been practiced universally owing to the excellent functional results:3 however, the open anterior quadricepsplasty has the drawbacks of wound dehiscence with anterior incision, mediolateral instability of knee following intraoperative release of retinacula or collaterals as well as inability to achieve desired length of the quadriceps. A modified technique: referred to as Calandra and furnish modification by Curtis and Fisher and later on adopted by Tercier S et al.4 supposedly addresses the above-mentioned limitations. Thus, we aim to assess and report the results of the modified approach in terms of wound associated problems and postoperative functional improvement in the patients undergoing quadricepsplasty. The inferences of our work will help surgeons develop best practice guidelines for CQC and CSK management. The objective is to identify and follow the technique that gains more function and at the same time avoid complications associated with the procedure.
Methodology
This study was conducted at Orthopedics unit of Ghurki trust teaching hospital (GTTH) Lahore. It was a retrospective case series, that was approved by ethical committee of GTTH Lahore. The study stretched over a period of 3 months: from 1stJuly, 2023 to 30th September, 2023. Record of a total of 23 patients with CDK/CQC, who underwent quadricepsplasty since 1st January 2015 were traced through the database and studied retrospectively: if they satisfied the study inclusion criteria. Irrespective of the gender, all the patient who had completed 3 years follow-up after undergoing quadricepsplasty via modified Curtis and Fisher technique were included. The patients with incomplete data, history of previous surgery on the same limb and those with any bony abnormality of the articulating surfaces of distal femur or tibia were excluded. Eventually a total of 23 patient were recruited: among these 8 patients underwent bilateral quadricepsplasty. Thus, a total of 31 knees were analyzed. This included cases that had been diagnosed with Arthrogryposis Multiplex Congenita (AMC) or Larsen syndrome. Similarly, cases with hip pathologies (DDH) and foot pathologies (including congenital talipes equinovarus [CTEV], Congenital vertical talus [CVT], plano-valgus) were part of the study sample.
The surgical procedure performed in these cases is a modification of Fisher and Curtis quadricepsplasty. The procedure is performed without a tourniquet with the patient in supine position. Orientation of knee is established by hyperextending it and placing two fingers at the distal femoral condyles. With this orientation lateral aspect is identified and incision is given at the distal mid-lateral thigh to the knee. Then deep fascia is cut and deep dissection is done till the quadriceps tendon is identified. The rectus femoris tendon is then separated from vastus medialis and lateralis; and a long slender tendon is fashioned. This rectus femoris tendon is cut transversely around the mid-thigh region its musculotendinous junction. This cut tendon and the attached patella are reflected distally and knee is bent at 90 degrees to view the distal femoral attachment of vastus medialis and lateralis in the suprapatellar region. With flexion of the knee pristine surface of knee joint becomes visible and the distal attachments of vastus medialis and lateralis get lateralized. These attachments of the vasti are then detached from distal femur and are fixed to the proximal end of previously incised rectus femoris tendon. Care is taken not to divide medial and lateral retinaculae or collateral ligaments of knee. This procedure allows sufficient gain of quadriceps length that a 90-degree knee flexion can be achieved without any tension on sutured tendons. Wound is closed inlayers after thorough hemostasis and placement of a drain. Above knee plaster of paris (POP) cast is applied with knee in 90-degree flexion: before application of POP. It is made sure that the skin on the anterior aspect of knee is not blanching because of stretch/tension at this 90?. This cast is left in place for 4 weeks and knee range of motion exercises are started thereafter. The physical therapy is supervised by a dedicated physiotherapy department. Regular OPD visits with both the orthopedic surgeons and the physiotherapists are done at 2-week, 4-week, 6-week, 3-month and then every 3 monthly till 12 months postoperative.
The data that was collected from these patients included basic demographic details and perop and final postop knee flexion and extension range of motion: both active and passive. Alongside this, quadriceps power was graded as per MRC power scale and knee joint was assessed for any laxity (grading of laxity was also done). The last follow-up assessment also included history of ambulatory status (community, household or no ambulation) as well as brace requirement. Based on these observations knee extension lag, flexion deformity and functional outcome were derived. Knee extension lag was defined as in ability to achieve full extension of knee actively. Flexion deformity was defined as the flexion that remained after full passive extension of knee. Functional outcome was categorized into excellent, good, fair and poor: as per previously used criteria5. Excellent knee function means a full range of stable, painless motion (up to 130–140? flexion); good means knee flexion of 90? or more with slight instability or pain; fair means knee flexion of 45 - 90 ? with mild instability or pain, and poor means knee flexion of less than 45 with gross instability and pain. This categorization was modified to add the disability that occurs due to extension lag, flexion deformity or brace/walking-aid requirement. One category was incurred in case any of the aforementioned disabilities were noted in the patient.
The collected data was entered in SPSS 23 and both descriptive and inferential analysis was performed for all the studied variables. Paired t- testing was used to evaluate improvements noted after the surgery and chi-square/independent sample t-test were applied for rest of the postoperative variables.
Results
A total of 23 patients (31 knees) were assessed. Mean age of the sample was 28±5.402 months and mean follow-up period was 48.12±24.5months. Majority of the sample were female (58.1%) and 17 patients (54.8%) had a diagnosis of congenital syndromes. Sixteen of these were diagnosed cases of AMC and 1 was diagnosed with Larsen syndrome. Associated DDH was noted in 4 patients and foot deformities were noted in 9 cases: 6 had CTEV, 2 had calcaneo-valgus and a single patient had CVT.
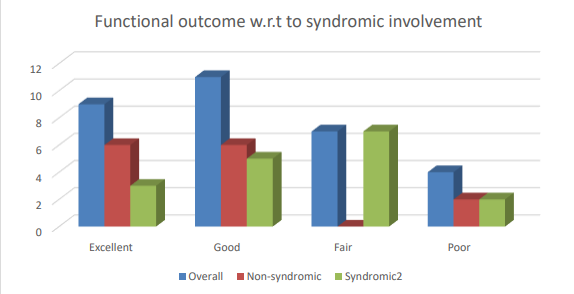
The preoperative and postoperative range of motion are presented in table 1. The mean preoperative ROM was 44.19±20.12 (18.54±13.67 extension to 25.64±12.36 flexion) and mean postoperative ROM was 103.38±29.25 (1.93±8.02 extension to 105.32±24.76 flexion). Thus, the improvement of 59.19±31.51 was noted and this improvement was statistically very highly significant (p<0.001). The postoperative mean power of quadriceps was 4.61±0.55 as per MRC grading. On the final postoperative assessment extension lag of 6.61±10.59 and flexion deformity of 3.38±6.63 was noted. The postoperative results were gauged as per the aforementioned outcome categorization system and the results showed that 9 knees (29%) had excellent, 11 knees (35,5%) had good, 7 knees (22.6%) had fair and 4 (12.9%) had poor functional outcome (figure 1). The figure also depicts that the functional outcome varied among the syndromic and non-syndromic patients.
Table 1: Comparison of pre and post quadricepsplasty knee range of motion.
|
|
Preop (mean ± SD) |
Postop (mean ± SD) |
t-value |
p-value |
|
Extension |
5.179 |
<0.001 |
||
|
Flexion |
-15.056 |
<0.001 |
||
|
Range of motion |
-10.456 |
<0.001 |
Overall improvement in ROM following the procedure was 59.19±31.51
Figure 1: Functional outcome as per the sample categories
Table 2 summarizes the comparative analysis of syndromic and non-syndromic patients. The two subgroups differed significantly from each other only in terms of postoperative quadriceps power (p=0.034) and functional outcome (p=0.049). Table 3 summarizes similar comparison between the case in which adjacent joints (hip and feet) were involved or not. Among these only the preoperative ROM displayed significant difference (p=0.012). Case by case assessment of the whole study population is summarized in table 4.
Table 2: Comparison of syndromic and non-syndromic patients undergoing quadricepsplasty
¥ Fisher exact test interpretation
Table 3: Comparison of patients with or without hip or foot involvement undergoing quadricepsplasty
¥ Fisher exact test interpretation
Table 4: Case by case demonstration of pre and post operative measurements
Discussion
The aim of quadricepsplasty has been achievement of around 90? flexion without causing weakness of the extension mechanism6. The results of our study illustrated that the technique we implemented was able to achieve 90 flexion on operation table and eventually improvement of 59.19±31.51 from the preop range of motion at a minimum of 3 years follow-up was noted. The added advantage of this technique in comparison to the traditional Curtis and Fisher technique is lowered wound complications.4 In our study where lateral incision was advocated, only one patient developed partial wound dehiscence and a single case developed wound infection. Both these cases were managed conservatively and the only long-term sequelae was a broader scar in each of these cases.
Another known complication of quadricepsplasty is instability of knee: a frequency as high as 78% has been reported3,7. In our study only grade one instability was noted in 6 knees (19.35%): half medial and half lateral. 60% of these were AMC cases: these syndromic patients have an innate tendency to have unstable knee. Thus, it can be inferred that the implemented technique of quadricepsplasty has the advantage of lowering the postoperative knee instability. At the same time the results achieved in terms of knee range of motion after more than 3 years follow-up was good and comparable to previously reported figures. An improvement of 59.19±31.51 in ROM of knee was noted in our study group. These are more or less similar to the results of Ferris et al and Johnson et al. i-e 76 and 49, respectively. Thus, the modified Curtis and Fisher technique that we use is effective at achieving all the three-intended goal: avoid skin complications, lower risk of postoperative knee instability and achieve good sustained improvement in range of motion at knee.
This lengthening of quadriceps tendon can render it weak and this weakness can manifest over long term in terms of extensor lag or flexion deformity. However, another school of thought is that this weakness is caused by the congenital syndromes that lead to knee contracture in the first place. In either case the remanent weakness and deformity is a genuine concern. Ooishi et al. reported an extensor lag of 30 in one out of the three patients he studied8. Bell et al. reported an extensor lag of 30 in 80% of the patients they studied9. Similar were the findings of this study: around 25% of the patient had mild (0-20) flexion deformity on the last follow-up. These results have been explained previously as an imbalance between the flexors and extensors around the knee joint. Quadricepsplasty weakens the extensor of knee (quadriceps). This allows hamstrings and gastrocnemius to overpower quads and thus cause flexion deformity at the knee. Furthermore, as most of the cases undergoing quadricepsplasty are syndromic and have muscle imbalance: this can further exaggerate the knee deformity.10
There were a few limitations of the study. Lack of a control group lowers the validity of comparative analysis presented by the study: had there been a group of patients undergoing traditional Curtis and Fisher quadricepsplasty, more solid conclusions could have been made. Furthermore, a larger and multicentric trial would add to the solidity of inferences, as most of the studies done till now lacked a large study group because the prevalence of severe CQC and CDK that require operative management is low.
Conclusion
The inferential analysis has brought us to the conclusion that the modified Curtis and Fisher quadricepsplasty achieves adequate and sustainable range of motion at the knee; and has good functional outcome. Furthermore, this technique when adopted properly lowers rate of instability at knee as well as wound related complications.
Conflict of interests: We have no conflict of interests or acknowledgements to mention.
Author’s contributions: JUH, MI and ZK proposed the study, analyzed the data, and prepared the final draft. HE contributed to the study design and data interpretation. UN, AUZ, AA contributed to review of the final manuscript, writing discussions and critical review.
Acknowledgements: We acknowledge the cooperation of all the doctor and non-doctor staff of Orthopedics unit of GTTH, Lahore: they were of huge assistance in the whole process of data collection.
Reference
1. Dobbs MB, Boehm S, Grange DK, Gurnett CA. Case report: congenital knee dislocation in a patient with Larsen syndrome and a novel filamin B mutation. Clin Orthop Relat Res 2008: 466(6):1503–1509
2. Shah NR, Limpaphayom N, Dobbs MB. A minimally invasive treatment protocol for the congenital dislocation of the knee. J Pediatr Orthop.2009: 29(7):720–725
3. Curtis BH, Fisher RL. Congenital hyperextension with anterior subluxation of the knee. Surgical treatment and longterm observations. J Bone Joint Surg Am. 1969; 51:255–269
4. Tercier S, Shah H, Joseph B. Quadricepsplasty for congenital dislocation of the knee and congenital quadriceps contracture. J Child Orthop. 2012; 6(5): 397–410
5. Ferris B, Aichroth P (1987) The treatment of congenital knee dislocation—a review of 19 knees. Clin Orthop 216:135–140
6. Johnson E, Audell R, Oppenheim WL. Congenital dislocation of the knee. J Pediatr Orthop.1987 7:194–200
7. Oetgen ME, Walick KS, Tulchin K, Karol LA, Johnston CE. Functional results after surgical treatment for congenital knee dislocation. J Pediatr Orthop. 2010 30:216–223
8. Ooishi T, Sugioka Y, Matsumoto S, Fujii T (1993) Congenital dislocation of the knee—its pathological features and treatment. Clin Orthop 287:187–192
9. Bell MJ, Atkins RM, Sharrard WJW. Irreducible congenital dislocation of the knee. Aetiology and management. J Bone Joint Surg Br 69B 1987 (3):403–406.
10. Sud A, Chaudhry A, Mehtani A, Tiwari A, Sharma D. Functional outcome following quadriceps tendon lengthening in congenital dislocation of the knee, with special reference to extensor weakness. Strat Traum Limb Recon. 2009; 4:123–127
Please click here to view complete article