A Case of Early Duodenal Perforation after Placement of a Biliary Stent. Review of Literature and Case Report
A Case of Early Duodenal Perforation after Placement of a Biliary Stent. Review of Literature and Case Report
Okoli, Fidelis, M.D.1; Golfeyz, Shmuel, M.D.2; Hamshow, Mohammad, M.D., MRCS, FACS3; Mayer, Ira, M.D., FACP, FACG, AGAF2, NYSGEF; Iswara, Kadirawel, M.D., FACP, FACG, AGAF2
1. Division of Gastroenterology, Hepatology and Nutrition, Department of Internal Medicine, New York University Langone Hospital, Long Island. New York.
2. Department of Internal Medicine, Division of Gastroenterology and Hepatology, Maimonides Medical Center, Brooklyn, New York.
3. Department of Surgery, Division of Hepatobiliary Surgery, Maimonides Medical Center, Brooklyn, New York.
*Correspondence to: Okoli, Fidelis, M.D, Email Address: okoli.fidel@gmail.com
Copyright
© 2024 Okoli, Fidelis, M.D. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 December 2023
Published: 17 January 2024
Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) with biliary stent placement is a common procedure performed to reestablish bile flow for conditions in which there is obstruction of the common bile, hepatic and pancreatic ducts. Stent migration is a common occurrence and many measures, such as creation of internal flanges and pigtails, have been taken to mitigate this from happening. Stent migration with intestinal perforation is a rare but well recognized life-threatening late complication. Herein, we report a case of a biliary stent causing a duodenal perforation that was diagnosed laparoscopically four days after stent placement. Additionally, we will review the literature on presentation, diagnosis and management of intestinal perforation from biliary stent placement.
KeyWords: Endoscopic Retrograde Cholangiopancreatography, Biliary stent, Intestinal perforation, Abdominal pain, Primary sclerosing cholangitis.
A Case of Early Duodenal Perforation after Placement of a Biliary Stent. Review of Literature and Case Report
Introduction
Since its introduction in the late 1970’s, the use of biliary stents for both benign and malignant conditions, has become the standard of care in reestablishing bile flow [1, 2]. Complication rates are approximately 8-10% and the mortality rate is less than 1% [3-5]. Complications include cholangitis, bleeding, cholecystitis, pancreatitis, stent occlusion, stent fracture, stent migration and intestinal perforation [6]. Migration of endoscopically placed biliary stents is a well-recognized complication which leads to intestinal perforation in less than 1% of cases. It is important to be aware of complications stemming from biliary stent placement and keep a high index of suspicion for this when appropriate [7]. The following case highlights an unusual presentation of early duodenal perforation diagnosed later while the patient was undergoing a laparoscopic cholecystectomy.
Figure 1A, Figure 1B
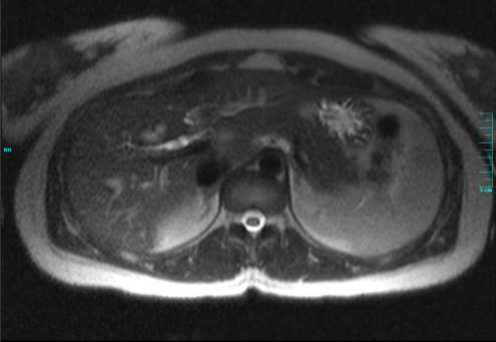
Figure 1A and 1B – MRCP showing the beading of the intrahepatic biliary tree with high grade strictures of the right and left hepatic ducts, suggestive of Primary Sclerosing Cholangitis
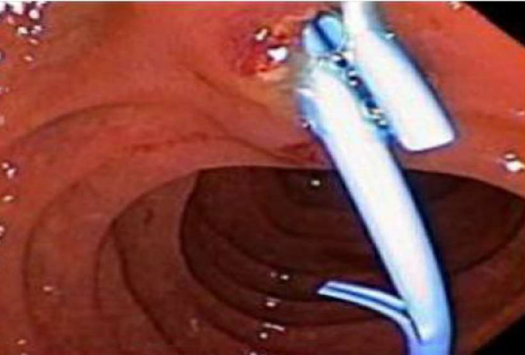
Figure 2 showing the straight plastic stents deployed in the right and left intrahepatic ducts.
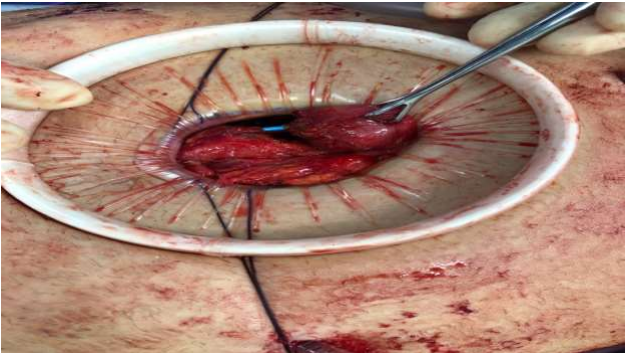
Figure 3 showing the stent eroding through the duodenum
Case Report
A 23-year-old Albanian woman presented with two days of severe, intermittent epigastric and right upper quadrant abdominal pain. The pain had been ongoing over the past year but worsened two weeks prior to admission. She admitted to dark urine and light-colored stools but denied diarrhea, constipation, blood in the stool, fevers, chills, night sweats, or weight loss. She was afebrile, normotensive with a normal heart and respiratory rate. She was noted to be in moderate distress and ill-appearing with scleral icterus. Abdominal examination revealed mild epigastric tenderness without guarding or rebound. Complete blood count was within normal limits with a normal platelet count as well as a normal INR and prothrombin time. Liver panel demonstrated a total bilirubin of 4.5mg/dL, direct bilirubin of 2.8mg/dL, alanine aminotransferase 354mg/dL, aspartate aminotransferase 174mg/dL, and alkaline phosphatase 118mg/dL. Hepatitis serologies were negative. Her CA 19-9 level was elevated to 143U/ml. Abdominal ultrasound revealed multiple gallstones within the dependent portion of a normal gallbladder, the largest measuring 0.6cm, and a prominent distal common bile duct (CBD) within the pancreatic head. Magnetic resonance cholangiopancreatography (MRCP) revealed beading of the intrahepatic biliary tree with high grade strictures of the right and left hepatic ducts, suggestive of Primary Sclerosing Cholangitis (PSC), cholelithiasis, and a small stone in the distal CBD with mild dilatation of the CBD and the intrahepatic biliary ducts [figure 1A and 1B]. She underwent ERCP where brushings were obtained from the strictured portions and sent for cytology. Additionally, a sphincterotomy was performed and stones and sludge were extracted from the bile ducts. A 7Fr x 9cm straight plastic stent was placed into the right intrahepatic system and a 7Fr x 15cm straight plastic stent was placed into the left intrahepatic system, [figure 2] though this stent was seen extending slightly within the duodenal lumen. The evening after the procedure, the patient developed an episode of vomiting and abdominal pain however her physical examination appeared stable from prior examinations. Labs obtained at that time revealed mildly elevated lipase with a mild leukocytosis so her symptoms were attributed to post-ERCP pancreatitis and she was made nil per os (NPO) and treated with intravenous fluids and analgesia. Her nausea and epigastric pain subsided by the next morning but she subsequently developed right lower quadrant abdominal pain. She was scheduled to undergo laparoscopic cholecystectomy the following day so the decision was made to also perform laparoscopic evaluation for the right lower quadrant pain and possible acute appendicitis, during the procedure. The laparoscopy revealed significant bilious fluid in the right paracolic gutter associated with inflammation. Upon further evaluation, the biliary stent was noted to be eroding through the duodenum at the junction of the second and the third portions [figure 3]. The duodenal perforation was repaired and reinforced with a Graham patch. Due to the extensive inflammation, a right hemicolectomy with ileocolic anastomosis was performed with copious lavage of the peritoneal cavity. The patient did well postoperatively and was discharged on the sixth postoperative day. Cytology from the biliary stricture brushings demonstrated reactive cells without evidence of malignant cells. Pathology from the surgical specimens demonstrated a segment of small and large intestine with marked acute and chronic inflammation involving peri-intestinal fat, with abscess, hemorrhage, fat necrosis and fibrinopurulent serosal exudates. The margins of the resection appeared viable.
Discussion
In 1980 Soehendra et al [8] introduced trans-papillary biliary drainage using a plastic biliary stent. Since then, endoscopic placement of biliary stents has become the standard of care in management of biliary obstruction from both benign and malignant conditions [9]. Stent migration occurs approximately 8-10% [2-4]. Stents can migrate proximally or distally. Johanson et al. reported the rates of proximal and distal stent migration to be 4.9% and 5.9% respectively [3]. Malignant strictures, larger diameter stents, and short stents are known to be associated with proximal biliary stent migration [10], whereas diverticular disease, previous intra-abdominal surgery, hernia and straight plastic stents are associated with distal stent migration [11]. Benign biliary strictures were associated with a higher risk of migration than malignant strictures [11] whereas placement of multiple biliary stents seems to reduce the incidence of stent migration. Arhan et al [5] reviewed 204 cases of plastic biliary stents placed for benign biliary disease and reported a migration rate of 13.4% with an equal proportion of stents found in the proximal and distal gastrointestinal tract. Of all migrated stents, approximately 43% pass spontaneously without complication [4, 5].
Migrated stents can typically be retrieved without issue. Unfortunately, stents may occasionally lodge into fixed portions of the intestine, leading to intestinal perforation. Intestinal perforation most commonly occurs in the duodenum [5, 12-14]. There have been reports of perforations in the liver, sigmoid colon, cecum and pancreas [9, 15]. Rare cases of biliary stents causing intestinal perforation have been reported in incarcerated bowel loops in a hernia sac as well as in duodenal diverticula [16, 17]. Additionally, inappropriately long stents may exert pressure on the duodenal wall causing tissue necrosis and perforation whereas curved stent or a double pigtail biliary stent may be associated with less migration and perforation [10]. Perforations can be retroperitoneal, such as in duodenal perforations and cause a bilioma, or intraperitoneal leading to biliary peritonitis [18, 19]. A plain abdominal radiograph or computed tomography (CT) scan are imaging modalities which are helpful in locating migrated stents and diagnosing perforation. Surgery is the treatment of choice for such complications [10].
Our patient had previous caesarean section and underwent straight plastic stent placement which was extending into the duodenal lumen, all which are risk factors for perforation. Our case is unique in that the stent perforation occurred early on after placement, as opposed to later, which is commonly described in the literature. Our patient experienced abdominal pain after the ERCP which was consistent with a picture of post-ERCP pancreatitis which is why further imaging wasn’t obtained earlier.
Conclusion
With the increased use of biliary stents in both benign and malignant conditions, it is important for physicians to be aware of the many different complications that may potentially arise. Although there are some well-established common complications, an astute physician will consider atypical presentations as cause for concern and further evaluation. Biliary stent migration leading to duodenal perforation, though rare, is a serious life-threatening complication requiring early diagnosis and treatment. Though it is commonly a later complication, our case highlights the fact that it can occur earlier on as well. Consideration of indication, condition, size and other risk factors is important when assessing what type of stent to use with biliary stenting, to reduce and mitigate complication rates. A high index of suspicion may lead to earlier diagnosis especially in a patient with abdominal pain and tenderness after stent placement.
Disclosures:
Conflict of Interest: Dr. Okoli, Dr. Golfeyz, Dr. Waintraub, Dr. Hamshow and Dr. Mayer have no conflict of interest to report. Dr. Kadirawel Iswara is a consultant speaker for Gilead, Abbvie and Pfizer.
Human/Animal Rights: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008(5).
Informed Consent: Informed consent was obtained from the patient in the case report.
Acknowledgment:
We would like to thank the radiology department for helping to obtain the films. We would also like to thank the pathology department for their help in obtaining the pathology slides.
Thank you, Daniel Oyinloye, for editing. Finally, many thanks to my beautiful wife Cuericka Okoli for her encouragement, support and for helping edit the material to the required specifications.
Reference
1.Lammer J, Neumayer K: Biliary drainage endoprostheses: experience with 201 placements. Radiology 1986, 159 3:625-629.
2.Mueller PR, Ferrucci JT, Jr., Teplick SK, et al.: Biliary stent endoprosthesis: analysis of complications in 113 patients. Radiology 1985, 156 3:637-639.
3.Johanson JF, Schmalz MJ, Geenen JE: Incidence and risk factors for biliary and pancreatic stent migration. Gastrointestinal endoscopy 1992, 38 3:341-346.
4.Chaurasia OP, Rauws EA, Fockens P, et al.: Endoscopic techniques for retrieval of proximally migrated biliary stents: the Amsterdam experience. Gastrointestinal endoscopy 1999, 50 6:780-785.
5.Arhan M, Odemis B, Parlak E, et al.: Migration of biliary plastic stents: experience of a tertiary center. Surgical endoscopy 2009, 23 4:769-775.
6.Yaprak M, Mesci A, Colak T, et al.: Biliary stent migration with duodenal perforation. The Eurasian journal of medicine 2008, 40 3:154-156.
7.Namdar T, Raffel AM, Topp SA, et al.: Complications and treatment of migrated biliary endoprostheses: a review of the literature. World journal of gastroenterology 2007, 13 40:5397-5399.
8. Soehendra N, Reynders-Frederix V: Palliative bile duct drainage - a new endoscopic method of introducing a transpapillary drain. Endoscopy 1980, 12 1:8-11.
9.Belyaev O, Muller CA, Uhl W: Double sigmoid colon perforation by a migrated biliary stent. Acta chirurgica Belgica 2008, 108 1:125-126.
10.Issa H, Nahawi M, Bseiso B, et al.: Migration of a biliary stent causing duodenal perforation and biliary peritonitis. World journal of gastrointestinal endoscopy 2013, 5 10:523-526.
11.Rasalkar DD, Paunipagar BK, Sonavane B: Migrating biliary stent with final destination at the ileocecal junction causing intestinal obstruction and obstructive biliopathy. The Indian journal of radiology & imaging 2010, 20 4:304-306.
12.Diller R, Senninger N, Kautz G, et al.: Stent migration necessitating surgical intervention. Surgical endoscopy 2003, 17 11:1803-1807.
13.Miller G, Yim D, Macari M, et al.: Retroperitoneal perforation of the duodenum from biliary stent erosion. Current surgery 2005, 62 5:512-515.
14.Saranga Bharathi R, Rao P, Ghosh K: Iatrogenic duodenal perforations caused by endoscopic biliary stenting and stent migration: an update. Endoscopy 2006, 38 12:1271-1274.
15.Barut I, Tarhan OR: Cecum perforation due to biliary stent migration. Saudi medical journal 2014, 35 7:747-749.
16.Akimboye F, Lloyd T, Hobson S, et al.: Migration of endoscopic biliary stent and small bowel perforation within an incisional hernia. Surgical laparoscopy, endoscopy & percutaneous techniques 2006, 16 1:39-40.
17.Mastorakos DP, Milman PJ, Cohen R, et al.: An unusual complication of a biliary stent-small bowel perforation of an incarcerated hernia sac. The American journal of gastroenterology 1998, 93 12:2533-2535.
18.Storkson RH, Edwin B, Reiertsen O, et al.: Gut perforation caused by biliary endoprosthesis. Endoscopy 2000, 32 1:87-89.
19.Roses LL, Ramirez AG, Seco AL, et al.: Clip closure of a duodenal perforation secondary to a biliary stent. Gastrointestinal endoscopy 2000, 51 4 Pt 1:487-489.