Ovarian PRP (Platelet-Rich Autologous Plasma) as a Patient-Oriented Strategy to Improve ART Treatment Outcomes Amongst Patients with Low Prognosis
Ovarian PRP (Platelet-Rich Autologous Plasma) as a Patient-Oriented Strategy to Improve ART Treatment Outcomes Amongst Patients with Low Prognosis
Dr. Nahla Kazim*
*Correspondence to: Dr Nahla Kazim MD, MSc, PhD (UAE). Consultant/ Reproductive Medicine and Infertility. Director of Fertility Preservation (Bourn Hall Fertility Clinic, UAE). Adjunct Associate Professor (UAE University).
Copyright
© 2024 Dr. Nahla Kazim. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 December 2023
Published: 17 January 2024
Ovarian PRP (Platelet-Rich Autologous Plasma) as a Patient-Oriented Strategy to Improve ART Treatment Outcomes Amongst Patients with Low Prognosis
Background
Patients who have low prognosis in ART often have reduced oocyte number, which ultimately affect the number of generated embryos, hence reducing the cumulative live birth rate.
As part of individualized ART treatment plan, patients with low prognosis stratified using the novel POSEIDON classification system, have undergone ovarian rejuvenation using PRP 1-3 months prior to undergoing ovarian stimulation to maximize the chances of retrieving the number of oocytes needed to obtain at least one euploid blastocyst for transfer in each patient. We test if such an intervention has a positive effect on reproductive success and reduce in the time to live birth.
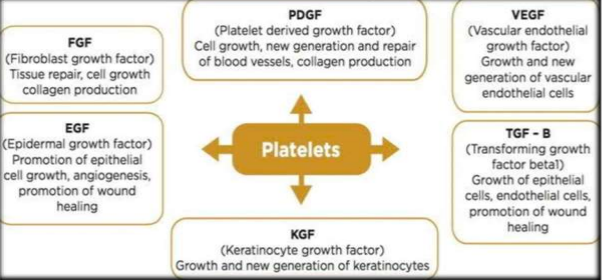
Autologous ovarian platelet-rich plasma treatment is reported to promote the development of isolated human primordial and primary follicles to the preantral stage. Platelets are Procoagulant, a rich source of growth factors and cytokines including platelet-derived growth factor αβ (PDGF-αβ), transforming growth factor β1 (TGF-β1) and vascular endothelial growth factor (VEGF). These biologically active proteins accelerate angiogenesis, cell migration, differentiation, and proliferation, enabling ovarian tissue regeneration. Dysregulation of these factors has been associated with infertility or ovarian diseases including diminished ovarian reserve, PCOS, endometriosis.
Design
Retrospective Case Study
Case Report
10 women ( aged 34- 45 years) with low prognosis have undergone ovarian PRP treatment prior to starting ovarian stimulation towards IVF/ICSI. All patients had multiple previous failed IVF/ICSI cycles. The FSH, LH, E2 and AMH levels were determined before the PRP treatment and at monthly intervals post PRP to monitor the ovarian function. The IVF/ ICSI cycle was started within 3 months post PRP and its outcomes were reported (number of MII oocytes, 2PN embryos, cleavage stage embryos, number of Euploid embryos)
Results
Exposure of ovarian tissues to autologous PRP treatment showed improvement of the ovarian reproductive function resulting in improved endocrinal status and parameters of IVF/ICSI cycle outcomes.
Conclusion
Ovarian PRP may be included as one of the patient-oriented strategies to help in achieving the individualized oocyte number needed to obtain euploid blastocyst amongst poor responders. Future studies with larger sample size and randomized prospective study design will be necessary to determine whether this intervention truly results in improved clinical outcomes and take-home baby rate.
Introduction
Platelet-Rich Plasma (PRP) is a sample of autologous plasma with platelet concentrations above baseline values, which is typically 150 000/µL to 450 000/µL. PRP is defined as having a minimum platelet concentration of 1000,000/µL, or approximately a five to eightfold increase in platelets from baseline. Platelets are a procoagulant, rich source of growth factors and cytokines, such as platelet-derived growth factor αβ (PDGF-αβ), transforming growth factor β1 (TGF-β1), and vascular endothelial growth factor (VEGF). These factors accelerate angiogenesis, cell migration, differentiation, and proliferation. Dysregulation of these factors is associated with infertility or ovarian diseases like diminished ovarian reserve, PCOS, and endometriosis.
The theory of "No new eggs" has been challenged by studies in animal models and humans. Detection of ovarian stem cells, germline stem cells, and embryonic-like stem cells in human ovarian surface epithelium has created the basis for ovarian PRP, which could give birth to new primary ovarian follicles and antral follicles. PRP has a potential therapeutic nature, enabling ovarian tissue regeneration, triggering or enabling differentiation of ovarian stem cells, and playing a role in neoangiogenesis.
Case Report-1
A 40-year-old Emirati woman with 8 years of secondary infertility attended an IVF cycle in September 2019. She had 16 previous IVF cycles in the UAE and abroad from 2012-2019, with 6 embryo transfers (Day 2-3) during earlier years. The patient's ovarian response declined from 12-15 eggs to 4-7 eggs in the UK over the years. No embryo transfer was performed in later years, due to embryo arrest and genetic abnormalities in screened embryos. The patient had hypothyroidism on Thyroxin replacement for 3 years. The patient had normal thrombophilia screening and had bilateral ovarian platelet rich plasma injections under GA. She had 4 ICSI cycles with 6x D3 embryo pooling from March 2020September 2020. In October 2020, six day 3 embryos were thawed and 3 embryos that reached Blastocyst were biopsied for NGS screening and refrozen. One normal Male found, however patient opted to go for another cycle.
In November 2020, she had 4 eggs collected from antagonist cycle , 4 were mature and injected, 3 fertilized, and one Blastocyst was biopsied for NGS screening and found to be normal. In March 2021, she had a modified natural cycle FET cycle with 2 normal embryo transfer. Patient had biochemical pregnancy.
Case Report 2
A 35-year-old Yemeni woman with 9 years of primary infertility experienced two failed IUI and four ICSI cycles, elsewhere. She had hyperthyroidism on Thyroxin replacement for 7 years and had anti-TPO positive. She had normal thrombophilia screening and had normal ovarian and endometrial platelet-rich plasma. In September 2020, she had her first ICSI post PRP, with an antagonist regimen. She had three eggs collected and fertilized, with 2 reaching to Blastocyst and biopsied then frozen. Both were found to be normal. In November 2020, she had a successful pregnancy following modified FET of two normal Embryos. Unfortunately, shortly after being diagnosed with COVID-19 infection, the patient had spontaneous preterm delivery at 35 weeks, with one male fetus was still born, and the female was discharged from the NICU two months later.
Results
The bioactive factors in platelet-rich plasma (PRP) varies depending on the protocols and preparation methods used. A systematic review found that platelet concentration in 33 commercially available PRP systems is directly correlated with collected blood volume, device centrifugal force, and additives used. There is a lack of information on the effects of WBCs (neutrophils, lymphocytes, and monocytes) on ovaries post PRP infusion. Neutrophils can cause inflammation by degrading tissue through releasing oxygen-free radicals and matrix metalloproteinases. Adequate centrifugation and preparation methodology are needed to avoid hemolysis and eryptosis due to the presence of pro-inflammatory cytokines in red blood cells. The optimal platelet concentration for PRP has not been identified, and too high can be detrimental to the healing process. Intranovarian infusion into atrophic ovaries is technically challenging, and there are risks including pain, infection, and bleeding. Combining PRP with aspirin and NSAIDs may potentially affect patient outcomes. No data on intra and post procedural antibiotic coverage is available. Careful interpretation of data post PRP is crucial, especially among poor responders with RIF.
Conclusion
Intraovarian PRP is an affordable, simple, and easily performed therapeutic modality for diminished ovarian reserve, poor ovarian response, and premature ovarian failure. However, there is limited research and data on its impact on pregnancy characteristics. To improve knowledge on PRP's mode of action, research on cellular and molecular levels, standardization of PRP preparation methods, a well-designed, large RCT, patient counseling, and long-term outcomes are needed.
Reference
1.Yamaguchi R , Terashima H , Yoneyama S , et al . Effects of platelet-rich plasma on intestinal anastomotic healing in rats: PrP concentration is a key factor. Journal of Surgical Research 2012;173:258–66.doi:10.1016/j.jss.2010.10.001
2.Fadadu, P.P.; Mazzola, A.J.; Hunter, C.W.; Davis, T.T. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: A call for PRP standardization. Reg. Anesth. Pain Med. 2019
3. Panda S R, Sachan S, Hota S (December 12, 2020) A Systematic Review Evaluating the Efficacy of Intra-Ovarian Infusion of Autologous PlateletRich Plasma in Patients With Poor Ovarian Reserve or Ovarian Insufficiency. Cureus 12(12): e12037. DOI 10.7759/cureus.1203
4.Panda S R, Sachan S, Hota S (December 12, 2020) A Systematic Review Evaluating the Efficacy of Intra-Ovarian Infusion of Autologous PlateletRich Plasma in Patients With Poor Ovarian Reserve or Ovarian Insufficiency. Cureus 12(12): e12037. DOI 10.7759/cureus.1203
5.Panda S R, Sachan S, Hota S (December 12, 2020) A Systematic Review Evaluating the Efficacy of Intra-Ovarian Infusion of Autologous PlateletRich Plasma in Patients With Poor Ovarian Reserve or Ovarian Insufficiency. Cureus 12(12): e12037. DOI 10.7759/cureus.1203
6.Vo, T.K.C.; Tanaka, Y.; Kawamura, K. Ovarian Rejuvenation Using Autologous Platelet-Rich Plasma. Endocrines 2021, 2, 15–27.