Uncovering the Impact: Exploring the Frequency, Risk Factors, and Results of Clinical Unconjugated Hyperbilirubinemia in Newborns
Uncovering the Impact: Exploring the Frequency, Risk Factors, and Results of Clinical Unconjugated Hyperbilirubinemia in Newborns
Dr. Rand Abdulghafoor*, Dr. Ahmad Elmelhat, Dr. Lama Almikati, Dr. Fatima Salah, Dr. Laila Ghazal, Dr. Marwa Alchar, Dr. Mohamed Elgharib, Dr. Mohammad Abunawas, Dr. Sara Jarrad, Dr. Sara Osman
*Correspondence to: Dr. Rand Abdulghafoor.
Copyright
© 2024: Dr. Rand Abdulghafoor. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 January 2024
Published: 01 February 2024
Uncovering the Impact: Exploring the Frequency, Risk Factors, and Results of Clinical Unconjugated Hyperbilirubinemia in Newborns
Introduction
The term jaundice is derived from the French word ‘jaune’ which means yellow. Neonatal jaundice is characterized by the appearance of yellowish color in skin as well as eyes (sclera and conjunctiva) (1). Hyperbilirubinemia is the most common cause of neonatal hospitalization (2). Although most newborns with hyperbilirubinemia have a good prognosis (3), approximately 8–11% maintain a high bilirubin level, which may lead to severe complications, including lifelong disability such as growth retardation, encephalopathy, autism and hearing impairment (4,5).
The incidence of pathological jaundice is 1% without risk factors of hyperbilirubinemia, whereas it is 59% with risk factors (6).
An imbalance between bilirubin production and conjugation is the main mechanism of jaundice, which leads to an increase in bilirubin levels. This imbalance often occurs due to the immature liver and the rapid breakdown of red blood cells, which may be involved with several factors (7,8).
There are a number of predisposing factors in the occurrence of this disease, including maternal diabetes, race, prematurity, height, polycythemia, male sex, cephalohematoma, medications, Trisomy 21, weight loss, breastfeeding, delayed meconium passage and family history of jaundice (9).
The most common cause of jaundice can be ABO incompatibility. Rh incompatibility and type of delivery can be among the controversial factors. Furthermore, some factors may contribute to jaundice, such as congenital infections (Syphilis, CMV, rubella, toxoplasmosis), and age more than 25 years (10).
The present study is aimed to investigate the predisposing factors (maternal and neonatal risk factors) in the incidence of jaundice in newborn infants admitted to HMS Mirdif Hospital, Dubai, UAE. Identifying predisposing factors in predicting the occurrence and prevention of such risks in neonates is important to reduce the morbidity and mortality of hyperbilirubinemia.
Keywords: Hyperbilirubinemia, newborn, NICU, neonatal, G6PD, phototherapy
Material and Methods
Study Design
This is an epidemiological retrospective case-control study.
Patient Selection
During the study period from March 2021 to December 2022, all neonates born at HMS Mirdif Hospital in Dubai, UAE, were included. They were divided into two groups: the study group, which consists of newborns diagnosed with clinical unconjugated hyperbilirubinemia, and the control group, which comprises newborns without a jaundice diagnosis.
Data Collection
The data for this study were obtained from the computerized registry database. To diagnose clinical hyperbilirubinemia, newborn babies underwent a clinical evaluation, and their bilirubin levels were measured transcutaneous and confirmed through laboratory testing. Additionally, detailed antenatal and maternal history, including factors such as nationality, maternal age, maternal and baby's blood group, parity, birth weight, multiple pregnancies, mode of delivery, and sex, were collected through a review of maternal and labor ward records.
Other Data Collection:
Data regarding maternal history of disease, medications taken during pregnancy, and type of feeding were also gathered. In the study group, additional information concerning the onset and duration of jaundice was included. Subgroup analysis was conducted to compare the risk factors and outcomes between local UAE nationals and non-UAE nationals to determine if there were any differences between the two groups.
Statistical Analysis
The collected data was revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (SPSS 26). Data was presented and suitable analysis was done according to the type of data obtained for each parameter.
i. Descriptive statistics:
1.Mean, Standard deviation [± SD] and range for parametric numerical data
2.Median and Interquartile range [IQR] for non-parametric numerical data.
3Frequency and percentage of non-numerical data.
ii. Analytical statistics:
1.Pearson’s R and Spearman correlation Tests were used to assess the statistical significance of the difference of a non-parametric variable between two study groups.
2.Chi-Square test was used to examine the relationship between two qualitative variables.
3.Fisher’s exact test was used to examine the relationship between two qualitative variables when the expected count is less than 5 in more than 20% of cells.
Outcome of the Study
The primary objective is to assess the prevalence of clinical unconjugated hyperbilirubinemia among newborns delivered at the HMS Mirdif hospital. The secondary objective is to examine the potential risk factors associated with this condition.
Results
Throughout the study period, a total of 607 babies were live born at our hospital, comprising 438 (72%) UAE nationals and 169 (28%) non-UAE nationals. Of these, 384 (57%) were included in the study group (babies diagnosed with clinical unconjugated hyperbilirubinemia), while 259 (43%) were categorized in the control group (babies not diagnosed with clinical jaundice). (Table 1)
The demographic characteristics encompassed in the study consist of gender, gestational age, weight for gestational age, maternal age, maternal and baby's blood group, parity, mode of delivery, type of gestation, gestational age, maternal diseases, medications taken during pregnancy, and type of feeding, as outlined in Table 2.
|
Nationality |
Study group |
Control group |
Percentage |
|
|
Valid |
UAE nationals |
253 |
185 |
72% |
|
Non-UAE nationals |
95 |
74 |
28% |
|
|
Total |
348 |
259 |
607 |
|
|
|
Percentage |
57% |
43% |
100% |
Table 1,
Table 2( Please click here to view table 2)
Gender distribution showed 52% males and 48% females. Among the sample population, preterm babies accounted for 21.6%, with 19.2% in the study group and 2.4% in the control group, while term babies represented 78.4%, with 38.2% in the study group and 40.2% in the control group. Majority infants were appropriate for gestational age 92.8%, followed by small for gestational age 5.8% and 1.4% were large for gestational.
The blood group "O" was the most prevalent among both mothers and babies, accounting for 66.2% and 44% respectively, while AB negative was the least common, representing 0.5% in both mothers and babies. Among maternal factors, Multiparas represented 66% while primigravida represented 34%. Nearly half of the maternal age group fell between 21 and 30 years old, comprising 49.3% of the total. Singleton pregnancies 96.5% compared to twin pregnancies 3.5%. Normal vaginal delivery (NVD) 63% was the highest mode of delivery observed.
Forty six percent of the sample group experienced complications related to pregnancy, with diabetes mellitus being the most prevalent at 17.2%. Additionally, 17% received different types of medications during pregnancy. Among the neonatal factors, mixed feeding was the most common at 60.1%, followed by artificial feeding at 20.3% and expressed breast milk at 19.6%.
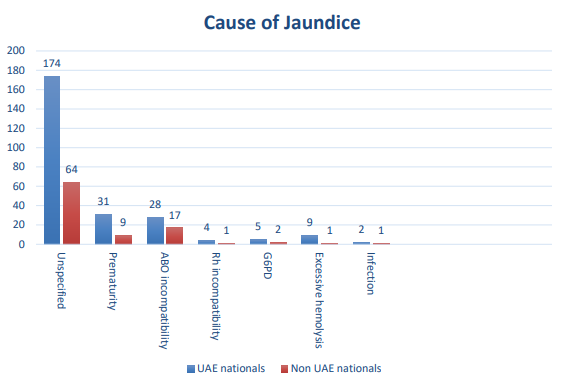
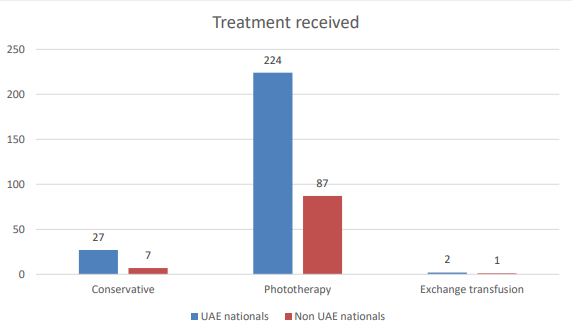
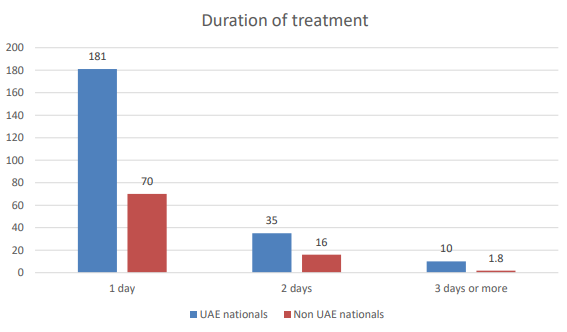
Figure 1 demonstrates the etiologies of clinical unconjugated hyperbilirubinemia, with neonatal jaundice unspecified comprising the highest percentage of cases at 62%. The majority of cases received phototherapy treatment, as indicated in Figure 2, with 89.4% undergoing this intervention. Moreover, Figure 3 illustrates the duration of hospital treatment, revealing that 72.1% of cases received treatment for one day.
Upon conducting subgroup analysis, no statistically significant difference was observed between the UAE nationals and non-UAE nationals in the study group with respect to the identified risk factors.
Figure 1 (Cause of jaundice):
Figure 2 (Treatment received):
Figure 3 (Duration of treatment)
Discussion
Our study findings contextualize the results within the existing body of knowledge on neonatal jaundice. The study identified several significant risk factors for neonatal jaundice, including small for gestational age, maternal blood group O positive, multiparity, singleton gestation, prematurity, mixed and artificial feeding, medications during pregnancy, and complications of pregnancy especially diabetes complicating pregnancy.
Firstly, the study's findings reveal a correlation between neonatal jaundice and specific risk factors. This sheds light on the complexity of neonatal health and emphasizes the need for targeted interventions for at-risk populations. The identification of these risk factors can aid healthcare professionals in early identification and appropriate management of infants at higher risk of developing clinical unconjugated hyperbilirubinemia.
Our findings align with those of Nima et al. regarding maternal blood group O and maternal diseases complicating pregnancy but differ in terms of the significance of the mode of delivery. In our study, the significance of the mode of delivery was not significant, whereas in Nima et al.'s study, it was found to be significant with normal vaginal delivery. (11)
The current study revealed a significant correlation between the incidence of unconjugated hyperbilirubinemia and being small for gestational age, prematurity, as well as maternal diseases, particularly diabetes and finally lack of breast feeding. These findings are consistent with those reported by Kahiya et al. (12)
In our study, the absence of breastfeeding was identified as a significant risk factor for the development of unconjugated hyperbilirubinemia. These results differ from those reported by Qun Lin et al., who found that exclusive breastfeeding was a significant risk factor for jaundice. (13)
Conclusion
In conclusion, the findings of this study underscore the importance of early recognition and management of risk factors for clinical unconjugated hyperbilirubinemia in newborns. By identifying and addressing these risk factors, healthcare providers can make significant strides in reducing the burden of neonatal jaundice and its associated complications. Future research endeavors should aim to further elucidate the complex interplay of risk factors and develop targeted interventions to improve the outcomes of infants affected by clinical unconjugated hyperbilirubinemia.
Recommendation
The implications of these findings are far-reaching. Understanding the risk factors associated with clinical unconjugated hyperbilirubinemia can inform prenatal care, discharge planning, and outpatient follow-up, leading to improved outcomes for newborns at risk. Moreover, healthcare providers can utilize this knowledge to develop targeted preventive strategies and patient education programs to reduce the incidence and severity of neonatal jaundice.
Limitation
It is essential to acknowledge the limitations of this study, including its retrospective design and potential selection bias. Future research should focus on conducting prospective studies to validate the identified risk factors and explore additional variables that may contribute to the development of clinical unconjugated hyperbilirubinemia in newborns. Another limitation of our study is the lack of consideration for other potential risk factors such as consanguinity and congenital anomalies.
Alternative explanations for the observed associations, such as the potential influence of genetic factors or environmental influences, should also be considered. However, our study's robust methodology and large sample size provide confidence in the validity of the identified risk factors.
References
1. Ebbesen F. The relationship between the cephalo-pedal progress of clinical icterus and the serum bilirubin concentration in newborn infants without blood type sensitization. Acta Obstet Gynecol Scand 1975;54:329-32.
2. Yu B, Hu F. Exploration of the pathogenic factors of neonatal jaundice and the clinical effect of blue phototherapy. Am J Transl Res 2021;13:6802-6.
3. Kuniyoshi Y, Tsujimoto Y, Banno M, et al. Neonatal jaundice, phototherapy and childhood allergic diseases: An updated systematic review and meta-analysis. Pediatr Allergy Immunol 2021;32:690-701. 10.1111/pai.13456
4. Okumura A, Ichimura S, Hayakawa M, et al. Neonatal Jaundice in Preterm Infants with Bilirubin Encephalopathy. Neonatology 2021;118:301-9. 10.1159/000513785
5. Kujabi ML, Petersen JP, Pedersen MV, et al. Neonatal jaundice and autism spectrum disorder: a systematic review and meta-analysis. Pediatr Res 2021;90:934-49. 10.1038/s41390-020-01272-x
6. Boskabadi H, Rakhshanizadeh F, Zakerihamidi M. Evaluation of Maternal Risk Factors in Neonatal Hyperbilirubinemia. Arch Iran Med 2020;23:128-40.
7. Adhikari M, Mackenjee H. Care of the newborn. In: Wittenberg DF, editor. Coovadia's paediatrics and child health. 6th ed. Cape Town, South Africa: Oxford University Press; 2010. pp. 129–130.
8. Kramer LI. Advancement of dermal icterus in the jaundiced newborn. Am J Dis Child. 1969;118(3):454–458. https://doi.org/10.1001/archpedi.1969.02100040456007.
9. Linn S, Schoenbaum SC, Monson RR, Rosner B, Stubblefield PG, Ryan KJ. Epidemiology of neonatal hyperbilirubinemia. Pediatrics. 1985;75(4):770–4. PMid:3982909.
10. Zarrinkoub F, Beigi A. Epidemiology of hyperbilirubinemia in the first 24 hours after birth. Tehran University Medical Journal. 2007;65(6):54–9.
11. Nima Dorji, Manish Raj Gurung, Dawa Gyeltshenc Krishna Singh Mongar, Sonam Wangmo and Tsheten. Epidemiology of neonatal jaundice at Punakha District Hospital, Punakha, Bhutan. International Health 2023; 15: 505–511.
12. Chiwoniso Mitchelle Kahiya; Abdoul Razak Mahaman Yacoubou; Mahamane Salissou Maibouge Tanko. Prevalence of Neonatal Jaundice and its Associated Risk Factors in Babies Born at Westend Hospital in Harare, Zimbabwe. Social Medicine 2023; Volume 16, Number 2.
13. Qun Lin, Daomou Zhu, Caihua Chen , Yonghong Feng , Fenfen Shen, Zhenkui Wu. Risk factors for neonatal hyperbilirubinemia: a systematic review and meta-analysis. Transl Pediatr 2022;11(6):1001-1009.