Soft Tissues Converting into Bones
Soft Tissues Converting into Bones
Dr. Kassem El Houcheimi*1
*Correspondence to: Dr Kassem El Houcheimi, FACS, MBA, Orthopedic surgeon, Clemenceau Medical Center Dubai.
Copyright
© 2020 Dr. Kassem El Houcheimi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 July 2020
Published: 01 August 2020
DOI: https://doi.org/10.5281/zenodo.10603124
Abstract
Fibrodysplasia ossificans progressiva (FOP) is a rare disorder in which skeletal muscles and connective tissues are gradually replaced by bones, occurring in about 1 in 2,000,000 newborns and about 834 people worldwide are known to have FOP. (1) Owning to the rarity of the disease there is often delay in diagnosis or misdiagnosis which significantly affects the quality and duration of life of this patient.
Soft Tissues Converting into Bones
Introduction
Fibrodysplasia Ossificans Progressiva (Myositis Ossificans Progressiva) was first described by Guy Patin in 1692 (2). It is a rare progressively disabling disorder characterized by short great toes and progressive extraskeletal ossification generally starting from the head and neck and progressing slowly to involve the thorax, abdomen and limbs. This results in restriction of movements and eventually immobility and untimely early death due to cardiorespiratory distress around the fourth decade of life. (3)
It is an extremely rare disease and according to International Fibrodysplasia Ossificans Progressiva Association (IFOPA) it is found in about 1 in 2,000,000 newborns occurring without any biases to gender, race or ethnicity. It is an autosomal dominant disorder, but most patients have denovo mutation in the bone morphogenic protein type 1 receptor (ACVR1). This leads to activation of osteogenesis in ectopic sites without ligand binding. (4)
Birth history is often uneventful except great toe abnormality like hallux valgus, shortened great toe, sharpening of the first metatarsal bone. Child usually presents in the first decade of life with complaints of intermittent episodes of painful soft tissue swelling which gradually hardens and becomes painless. These episodes are triggered by trauma, invasive medical procedure, or a viral illness. Hence biopsy is a contraindication in these patients.
If the disease is diagnosed early in life, then with proper precautions and counselling, the progression of the disease can be slowed down and quality of life of the patient can be improved.
Case Report
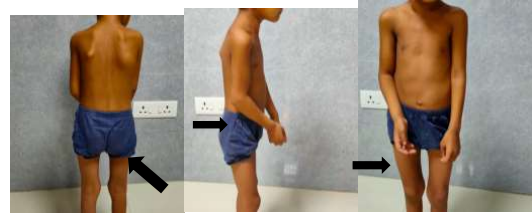
A 5 year old female child, 2nd child born of non consanguineous marriage presented with pain and swelling over bilateral upper chest, back, right lateral aspect of neck and right elbow for last 20 days. There was history of similar episodes in the past. On examination child was hemodynamically stable with swelling and tenderness present on lateral wall of chest on both sides and back associated with indurated redness of the overlying skin. (Figure 1) There was also swelling and tenderness of right elbow with local rise of temperature. This was associated with restriction of movement at both shoulder joint and right elbow joint.
Figure 1: It shows swelling on the back on right side, right side of neck and flexed posture of right hand due to ossification and inability to extend it.
Ultrasound done was suggestive of inflammatory changes in the anterior chest wall involving skin, subcutaneous tissue and muscular planes and CT chest done was suggestive of inflammatory myopathy with fatty atrophy. Child was initially kept as a case myositis with cellulitis although inflammatory markers were negative. A possibility of polymyositis was also kept in mind and workup done in which ANA profile was negative and eye evaluation was normal.
As the inflammation subsided it was noticed that the restriction of movement increased instead of improving and plain radiograph showed extraskeletal ossification. On further evaluation child was found to have short B/L 1st metatarsal which on plain radiograph of bilateral foot showed only one phalanx of the great toe. (Figure 2) MRI showed edema and enhancement along the muscle fibers and fat planes of bilateral shoulder girdle, arms and right side of neck with areas of ossification within, along with hyper-enhancing pre-osseous soft tissue in left paraspinal/scapular region extending along left chest wall. Based on these findings child was now thought to be a rare case of Fibrodysplasia Ossificans Progressiva and genetic workup for the same sent which confirmed mutation of ACVR1 gene on exon 6 and hence confirming the diagnosis beyond doubts.
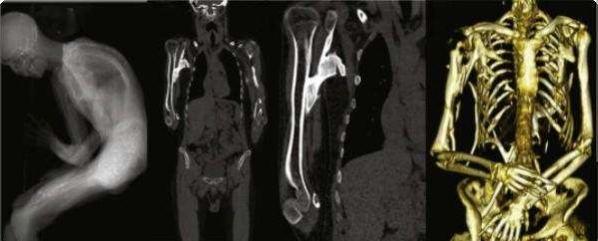
Figure 2: A) Plain radiograph showing hallux valgus and only one phalanx of the great toe resulting in short great toe bilaterally. B and C) Plain radiograph showing heterotopic ossification in the soft tissues.
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Figure 8
Figure 9
The child was then managed with analgesics and oral prednisolone and parents were counselled regarding the nature of disease and its future implications and to visit a doctor at first sign of trauma or inflammation to start prednisolone.
Discussion
Fibrodysplasia ossificans progressive is an ultra rare disease with peculiar and diagnostic features of extraskeletal new bone formation and great toe abnormality. Our patient also had a single phalanx of great toe bilaterally which has not been mentioned in literature before.Owing to the rarity of the disease it is not surprising that the diagnosis was delayed and was not made at initial presentations.
According to a survey done by Kitterman et al (5) which included patients from 5 continents showed that the patients are misdiagnosed in 90% cases and about 67% of the patients are subjected to harmful invasive diagnostic procedures like biopsy before arriving at the diagnosis. Spreading awareness about the disease amongst the medical practitioners is the key to prevent harm to the patient and timely diagnosis and adequate treatment. Although being a rare disease the uniqueness of the clinical features and the availability of genetic testing makes the diagnosis easier if a possibility of FOP is kept in mind. Genetic testing being a confirmatory test prevents unnecessary invasive workup which could be detrimental for the patient.
It is possible to confuse similar presentation with a diagnosis of myositis or cellulitis, but on probing into history look for similar episodes in the past which resulted in hardening of the swellings and also any trigger factor before each flareup. Signs of heterotopic ossification on plain radiograph and great toe deformity will help you clinch the diagnosis before rushing into any invasive procedures and doing harm to the patient.
A few cases have been reported in India who have presented between the age of 5-10 years and most of them have been exposed to invasive diagnostic procedures. In a case reported by Kumar A. et al(6), who was followed up for 20 years when the patient was in her third decade and had become wheelchair bound with jaw ankylosis and thoracic insufficiency syndrome hence having a grave prognosis and poor quality of life. Thus signifying how important is early diagnosis and preventive interventions to improve the patients quality of life.
FOP is caused by a mutation of a gene on chromosome 2 (2q23-24) for a transmembrane receptor in the BMP signaling pathway called ACVR1. BMPs are members of the transforming growth factor- beta superfamily and play a role in the development of bone and other tissues. This mutation leads to heterotopic ossification in soft tissues including muscle planes and ligaments.
Current mainstay of treatment is steroids and non steroidal anti-inflammatory drugs given at the onset of flare-up, avoiding trauma and invasive procedures. However there is no curative options for FOP, but studies are underway and Activin receptor-like kinase-2 (ALK2) inhibitor has come up as a promising option and therapeutic trials are underway. (7)
Reference
1. Examining Quality of Life and treatment options for Fibrodysplasia Ossificans Progressiva and Multiple Osteochondromas, AJMC. 2019
2. Baidoo RO, Dayie MS. Fibrodysplasia ossificans progressiva: a case report. Ghana Med J. 2016;50(4):248-50.
3. Kaplan F, Zassloff M ,Kitterman J, Shore E, Hong C, Rocke D. Early Mortality and Cardiorespiratory Failure in Patients with Fibrodysplasia Ossificans Progressiva. J Bone Joint Surg Am. 2010 ; 92(3): 686–91
4. Pignolo R, Kaplan F. Pediatric Fibrodysplasia Ossificans Progressiva. E-medicine. 2009; http://emedicine.medscape.com/article/1007104-overview.
5. Kitterman JA, Kantanie S, Rocke DM, Kaplan FS. Iatrogenic harm caused by diagnostic errors in fibrodysplasia ossificans progressiva. Pediatrics. 2005 Nov;116(5):e654-61.
6. Abhishek K, Jain S, Khadgawat R. A case of fibrodysplasia ossificans progressiva: 20 years of follow-up. Neurol India 2016;64:354-6
7. Sekimata K, Sato T, Sakai N. ALK2: A Therapeutic Target for Fibrodysplasia Ossificans Progressiva and Diffuse Intrinsic Pontine Glioma. Chem Pharm Bull (Tokyo). 2020;68(3):194-200.