A Case Report on IgG4-Related Sclerosing Cholangitis – A Challenging Diagnosis of Obstructive Jaundice
A Case Report on IgG4-Related Sclerosing Cholangitis – A Challenging Diagnosis of Obstructive Jaundice
B. Tan*
*Correspondence to: B. Tan, UK.
Copyright
© 2024 B. Tan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 January 2024
Published: 06 February 2024
Abstract
An 83- year old male of English origin was referred for investigation of obstructive jaundice. He also reported frequent symptoms of intermittent upper abdominal pain, with no other red flag symptoms. He has a past medical history including previous gallstones with endoscopic retrograde cholangio pancreatography (ERCP) and sphincterotomy, asthma, glaucoma, chronic back pain, type 2 diabetes mellitus, pyogenic granuloma, pemphigus vulgaris, and chronic kidney disease. There was no significant family history. Examination revealed normal BMI, peripheral jaundice, mild right upper quadant and epigastric tenderness with absence of stigmata of chronic liver disease.
His blood tests were unremarkable apart from deranged liver function tests (LFTs) with obstructive pattern, positive anti-mitochondrial antibodies, ANA, anti-Ro antibody, extractable nuclear antigen and raised IgG. The tumor markers and infection screen were all negative. Abdominal ultrasound revealed distended gallbladder wall and subsequent computed tomography (CT) demonstrated a renal pseudotumor. A magnetic resonance chloangiopancreatography (MRCP) showed dilated common bile duct (CBD) of 15mm with gallstone and features suspicious of PSC. He underwent ERCP with stent insertion and it showed normal biliary duct. Unfortunately, his symptoms persisted. Given the absence of red flag symptoms, tumor on imaging, and normal tumor markers, this rules out hepatobiliary malignancy. The normal bile duct on ERCP, age of presentation, and lack of risk factors excludes primary sclerosing cholangitis and primary biliary cirrhosis.
The presence of raised IgG levels, multi-organ involvement including CKD, pseudotumor, pemphigus vulgaris and pyogenic granulatoma raised the suspicion of IgG4-sclerosing cholangitis (IgG4-SC). He was therefore tested for IgG4 level which was more than 10x above the upper limit of normal. Following a trial of oral Budesonide 3mg twice daily, he reported rapid response to steroid treatment and further improvement in his LFTs. On follow up reviews after 2, 4, and 6 months, the patient remains asymptomatic and Budesonide was gradually weaned and stopped. Given the remarkably raised IgG4 level, dramatic response to steroid treatment and presence of IgG4 multi-organ involvement, this points towards IgG4-SC.
A Case Report on IgG4-Related Sclerosing Cholangitis – A Challenging Diagnosis of Obstructive Jaundice
Background
This is a rare presentation of the IgG4-SC which is characterized by raised serum IgG4 level, infiltration of IgG4-positive lymphoplasmacytic cells with storiform fibrosis and/or obliterative phlebitis which responds dramatically to steroid treatment.3,4 The main lesson learnt is that it is important to take a thorough history including past medical history, physical examination, test for relevant biochemical analysis, and exclude secondary causes. It is also crucial to understand that not every patient requires invasive intervention to arrive at a diagnosis. Approximately 15 % of patients who underwent resection for presumed CCA had benign tumor histology.1,2 Delay in diagnosis and management of IgG4-SC may lead to prolonged hospital stay, increased morbidity and mortality due to delay in steroid treatment, and unnecessary investigations which may cause anxiety in patients.4 On the other hand, misdiagnosis of cholangiocarcinoma may put the patient at risk of unnecessary surgery.1,2
Here, we will review the pathophysiology, diagnostic criterias and management currently available for IgG4-SC. Despite its diagnostic challenge and rarity, it is essential to distinguish IgG4-SC from other benign diseases and malignancy and minimize invasive interventions.
Case Report
An 83-year-old Caucasian male patient presented himself to our medical unit complaining of non-radiating intermittent upper abdominal pain and jaundice associated with nausea and vomiting ongoing in the last 2 months. He did not have any history of pale stools, dark urine, pruritus or altered bowel habit. His pain was not associated with any food, no radiation and no triggering factor. He noticed he became increasingly jaundiced, worsening nausea and vomiting for a few weeks before he presented to A&E, thus, admitted to the hospital. He denied any symptoms of fever, night sweats, malaise, weight loss, dysphagia, hematochezia, haemetemesis, malaena or bloody stool. His past medical history comprises of gallstones 7 years ago for which he had an ERCP with sphincterotomy, asthma, glaucoma, chronic back pain, type 2 diabetes, pyogenic granuloma, pemphigus vulgaris, and chronic kidney disease. There was no significant family history associated with malignancy or gastrointestinal diseases. He denied any other risk factors of hepatitis such as intravenous drug use, sexual orientation, blood transfusion, needlestick injury or sharing.
On examination, the patient appeared visibly jaundiced, with no other peripheral stigmata suggestive of chronic liver disease. He has normal body mass index (BMI) of 23 (normal range 18.5-25) and did not appear cachectic. Abdomen was soft and mildly tender in the right upper quadrant, with no masses felt and there was no abdominal distension. Shifting dullness test was negative. There were no other abnormal findings on clinical examination.
His blood tests on admission revealed deranged liver function tests consistent with obstructive jaundice: total bilirubin 56 umol/L, alkaline phosphatase (ALP) 765 U/L, alanine aminotransferase (ALT) 81U/L, aspartate aminotransferase (AST) 51 U/L and gamma-glutamyl transpeptidase (GGT) 128U/L. The tumor marker Ca 19-9 and AFP were within the normal range. His full blood count revealed an increased WCC (16.9x109/L) with normal eosinophils (0.2x109/L) and rest of his bloods were all within normal range.
A liver screen including autoimmune profiles and viral serology revealed no abnormalities apart from positive M2 anti-mitochondrial antibodies (AMA), raised anti-nuclear antibodies (ANA) >200 CU, positive anti-Ro antibody, positive extractable nuclear antigen (ENA) screen and raised IgG of 26.4 g/L. In view of the positive AMA, primary biliary cirrhosis (PBC) formed part of the differential diagnosis.5
We then ordered a set of imaging investigations as part of the diagnostic workup. An abdominal ultrasound sonography (USS) test demonstrated an over-distended gallbladder containing sludge, patchy and irregular border of liver with simple renal cysts of both kidneys. There were no gallstones, focal lesions or hepatic duct dilatation. A contrast-enhanced CT of chest, abdomen and pelvis revealed an enlarged, irregularly calcified tail of pancreas, which was initially suspected to be a neoplastic lesion. Pneumobilia was also noted in keeping with previous sphincterotomy, with filling defects in the dilated common bile duct (CBD) probably secondary to his previous gallstones. It was also reported that there was an unusual appearance of both renal pedicles, and visible soft tissue mass in the proximal ureters that may suggest renal cell carcinoma.
A subsequent multidisciplinary team discussion decided based on imaging that an infiltration of the ureters is unlikely due to malignancy and that the pancreatic tail lesion was unlikely neoplastic.
A magnetic resonance chloangiopancreatography (MRCP) demonstrated a dilated CBD of 15mm diameter with 13mm filling defect indicating obstructive gallstones. Intrahepatic ducts showed biliary strictures, which may suggest primary sclerosing cholangitis (PSC), and irregular liver contours indicating chronic liver disease. A fibroscan result was 14kPA, consistent with liver cirrhosis. An endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and stenting was performed for removal of the gallstones. It also demonstrated a normal appearance of the biliary ducts with no suspicious areas hence biopsies were not performed. A second ERCP followed for stent and further gallstone removal. Unfortunately the patient’s symptoms did not improve. A subsequent abdominal USS demonstrated a persistently dilated CBD, unchanged in appearance from the previous scans.
In view of the above biochemistry and imaging results, there are a few differential diagnoses we can consider at this point. Negative viral serology meant we can exclude viral hepatitis. Primary biliary cirrhosis (PBC) could be possible with the positive AMA test and primary sclerosing cholangitis (PSC) as the other differential. However, it is unlikely PBC or PSC given his age of presentation and lack of risk factors for both PBC and PSC including family history, autoimmune diseases, non-smoker, and male gender. He also does not have any symptoms suggestive of inflammatory bowel disease which is often associated with PSC.22
He has only low risk factors for cholangiocarcinoma including older age, gallstones and type 2 diabetes mellitus. There was no history of smoking, family history of hepatobiliary and pancreatic malignancy, minimal alcohol intake, and absence of IBD, infection and PSC. Despite the presence of these risk factors, MRCP and ERCP did not reveal any evidence of malignancy. Absence of red flag symptoms and normal tumor markers further support the unlikelihood of malignancy.
He had unremarkable drug history that would raise concerns of drug-related hepatotoxicity and he has no history of alcohol excess. It is unlikely that he has lymphoma associated sclerosing cholangitis as he did not have any B symptoms such as fever, weight loss, or night sweats. His HIV screen was also negative which rules out AIDS cholangiopathy and he did not have any surgery or chemotherapy which can result in secondary cause of sclerosing cholangitis.
He was then found to have raised serum IgG level at 26.4 (normal range 7.23-16.85 g/L) and markedly raised at 14.1 g/L (upper limit of normal 1.3 g/L). He also has risk factors of IgG4-SC including male gender, older age, and co-existent history of IgG4-related disease. He fulfils majority of the HISORTs criteria to diagnose IgG4-SC which includes CKD, kidney pseudotumours, pemphigus vulgaris and pyogenic granulom. We therefore considered the possibility of IgG4 sclerosing cholangitis (IgG4-SC), a hepatic manifestation within the wider spectrum of IgG4-related disease.6,7,8
We therefore commenced the patient on oral Budesonide 3mg twice daily (6mg per day) as it has less systemic effects than traditional glucocorticoids.9 On reassessment 2 weeks after initiation of steroids, his liver function tests had dramatically improved. His total bilirubin had normalized to 10 umol/L, ALP levels dropped to 295 U/L and ALT reduced to 76 U/L. Patient also remains completely asymptomatic since initiation of his steroid treatment, which would not have been the case if it were cholangiocarcinoma, PBC or PSC. On follow up review after 4 months, his liver function tests continued to improve, and patient remains asymptomatic. His Budesonide dose was weaned down to 4mg on the following week, 2 mg the week after and subsequently stopping his steroid medication. The dramatic response to steroid treatment further supports the diagnosis of IgG4-SC.
Figure1, Figure2, Figure 5
Discussion
IgG4 sclerosing cholangitis (IgG4-SC) is a rare benign biliary disease, characterised by raised serum IgG4 levels, presence of IgG4+ve plasma cells, storiform fibrosis, obliterative phelibitis, and most importantly, good response to steroids.3 IgG4 sclerosing cholangitis often associated with autoimmune pancreatitis (AIP), and it is currently accepted to be the hepatic manifestation of the wider IgG4-related disease spectrum. However, isolated sclerosing cholangitis without AIP with IgG4-related disease has been referred as “isolated IgG4-SC”.19 IgG4-SC can be associated with multiple organ systems including salivary gland disease, orbital or renal pseudotumors, chronic periaortitis, tubulointerstitial nephritis mimicking chronic kidney disease, skin involvement including pemphigus vulgaris and foliaceus.4,6,7,8,10 Our patient has the characteristic manifestation of disease related to IgG4 including renal pseudotumor, pemphigus vulgaris and plasma cell granuloma.4,6,7,17,18
There are several hypothesis postulated in the pathogenesis of IgG4-SC. Antibodies play a critical role in our innate immune system, especially mediating pro-inflammatory responses. IgG4 is a very dynamic antibody consisting of a light chain and heavy chain and is a critical event in IgG4-related disease.11,12,24 It has been reported that IgG4 hyperproduction can be caused by increased T-helper (Th2) dominated cytokine and T regulatory cells.15,25, There are four subclasses of IgGs, mainly dominated by IgG1 and least dominated by IgG4.26 IgG4 is a stable four- chain molecule which does not exchange half-molecule in a standard environment. When it is catalysed in-vivo, half-molecule exchange occurs due to flexible hinge allowing formation of intrachain cyclized disulphide. This leads to production of half-antibodies, which are non-covalently linked heavy chains that allow exchange of Fab arms by swapping a heavy chain and attached light chain. This forms bispecific antibodies that has functional monovalency.26 Rispens et al. also performed a research study using quantitative real-time FRET assays demonstrating that IgG4 can undergo a half-molecule exchange ‘Fab-arm exchange’ which leads to formation of asymmetrical and bispecific antibodies.12 Upon contact with antigen presented by B-cells, IgG4/IgE class-switch probably occurs due to influence of cytokines released by activated Th2 and Treg cells.27,28 This forms small and harmless immune complexes.26 CD4+ T-cells are thought to produce profibrotic cytokines such as interleukin-4 (IL-4), IL10, IL13, and TGF-β, whereas, IgG4 may have profibrotic action via IL-6.28 Although IgG4 has anti-inflammatory effect, however, when a strong IgG4 with IgE response occurs in the presence of an antigen presented by B-cell, the response may lead to antigen capture by innate immune cells via Fc receptor binding and presentation to T-cells.28 This sequence of events can ultimately lead to fibroblast activation, increased myofibroblasts and extracellular matrix deposition. However, it is unknown if this contributes to fibroinflammatory infiltrate in IgG4-related diseases.28
Subsequent studies have demonstrated that IgG4 are capable in immune complex formations in multi-organ systems including the renal, meninges, skin, orbitals, excretory glands, pharynx, lymph nodes, cardiorespiratory, gastrointestinal, genitourinary and musculoskeletal systems.4,6,7,8,13
Other hypothesis also suggested that it is an autoimmune cause. This was supported with evidence of injection of IgG from patients with autoimmune pancreatitis (AIP) into neonatal mice induces pancreatic injury.29 Detection of autoantibodies in patients with IgG4-SC with HLA haplotypes for AIP, with good response to steroids further supports this hypothesis.30,31
One suggests the production of antibodies against the plasminogen-binding protein of Helicobacter Pylori can act as molecular mimicry leading to antigen exposure. It was postulated that this perpetuates immune reaction found in autoimmune pancreatitis.32 This association, however, is still heavily disputed with a recent study by Culver et al in 2017 demonstrating no difference in immunological memory of Helicobacter pylori between IgG4-RD patients compared to controls.33
Other potential hypothesis include allergy, paraneoplastic syndrome and immune complex deposition.34,35
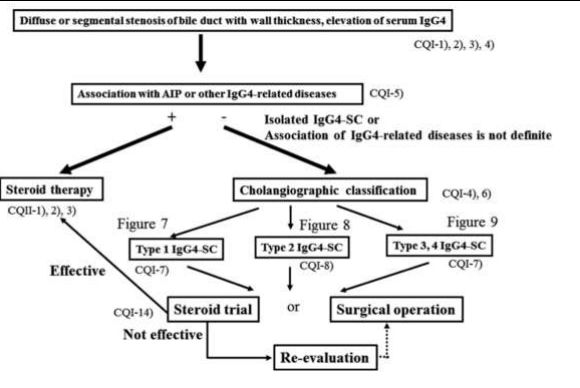
Figure 3: Diagnostic algorithm for IgG4-SC, adapted from Kamisawa et al.19
Kamisawa et al. recommended a diagnostic algorithm for IgG4-SC.19 After excluding other causes cholestatic jaundice, PSC, malignancy, and secondary sclerosing cholangitis as discussed in the case report with accurate history taking and examination, blood tests, imaging and tumor markers, we then consider the differential diagnosis of IgG4-SC. In our case, the patient fits in 4 out of 5 HISORt criteria and definite diagnosis in the Japanese clinical diagnostic criteria as outlined below. This includes the presence of stricture of intrahepatic duct on MRCP, positive IgG4 level above upper limit of normal, multi-organ involvement including renal and skin as well as good response to steroids.10,36,37 Kamisawa et al. recommended trial of steroid therapy in the presence of bile duct stricture on imaging, elevated serum IgG4 and other IgG4-related diseases. The diagnosis of IgG4-SC is further supported with dramatic response to steroid treatment.19,23
HISORt (histology, imaging, serology, other organ involvement and response to therapy) was adapted from the Mayo clinic originally developed for autoimmune pancreatitis and subsequently adapted by Ghazale and Culver et al to diagnose IgG4-SC.10,36
In addition, the Japanese Biliary Association also suggests clinical diagnostic criteria for IgG4-SC based on serum IgG4, biliary tract imaging, multi-organ involvement, histopathology or steroid therapy. It classifies IgG4-SC as definite, probable and possible diagnosis.10,37
Figure 6
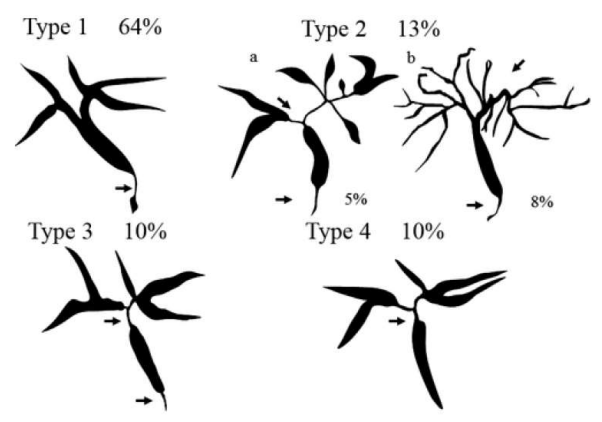
Figure 4 demonstrates the classification of SC with autimmune pancreatitis by cholangiography. Type 1: stenosis in lower common bile duct (CBD). Type 2: stenosis in intra and extrahepatic bile ducts, with 2a has prestenotic dilation and 2b without prestenotic dilation and reduced number of bile duct branches. Type 3: stenosis in both hilar hepatic lesions and lower CBD. Type 4: stenosis only in hilar hepatic lesions. Adapted from Kamisawa et al.19, 38
Kamisawa et al. recommends contrast-enhanced CT and MRCP are vital to aid the diagnosis of IgG4-SC as transmural biliary inflammation often occurs in IgG4-SC, whereas PSC often affects the luminal and epithelium. On the other hand, cholangiocarcinoma arises from epithelial layer and it has an invasive nature. Kamisawa et al. also divides IgG4-SC into 4 types of classifications. Unfortunately, our ERCP was normal. Hence, no biopsies were taken.19 The author also advised for endoscopic ultrasound (EUS) to identify the thickening of bile duct wall. However, it will be challenging to try to differentiate IgG4-SC from PSC or choalangiocarcinoma based on EUS.38 Liver biopsy or intraductal ultrasound of the pancreaticobiliary ductal system can also be obtained when the diagnosis is uncertain.19
Steroids is the first line of treatment for IgG4 as it has remission rate of 90% and current consensus recommended for oral prednisolone .19, 39, 40,41 Current consensus recommended oral prednisolone 0.6mg/kg/day (30-40mg/day) for first 2-4 weeks as an initial remission-induction therapy, then gradually wean 5mg every 102 weeks after induction of remission and stay on maintenance dose of 5mg/day for 3 years before consideration of reducing or discontinuing steroid therapy.19 Response to steroid treatment should be assessed via laboratory tests and imaging.19 In our case, budesonide of 6mg per day was a preferred option as budesonide has less systemic effect, fast hepatic metabolism and a good alternative for systemic corticosteroids and he was weaned to 3mg after 4 weeks.45 His blood sugar was regularly monitored given his background of diabetes and his blood sugar remained within the target range. However, there is lack of published guideline to advise on the maintenance dose of Budensonide for IgG4-SC. He is currently on low dose of Budesonide of 2mg once daily and continued to maintain in remission after 4 months. Approximately 16 to 53% of relapse rates of biliary stricture reported after tapering steroid treatment.42,43 Relapsed IgG4-SC can be treated by reintroducing and increasing dose of steroids, rituximab or immunomodulatory drugs such as azathioprine, 6-mercaptopurine, mycophenolate mofetil, and methotrexate. 46,47,48,49,50,51. Good disease response has been reported in 80-90% of IgG4-SC with Rituximab (a mono-clonal anti-CD20 antibody). Rituximab is also a good alternative in steroid-resistant IgG4-SC.51,52,53,54 Recent evidences also recommended for biliary drainage in cases of moderate to severe obstructive jaundice and our patient underwent ERCP to relieve biliary obstruction prior to initiation of steroids.19, 44
Conclusion
IgG4-SC is a rare condition characterised by raised serum IgG4 level and infiltration of IgG4-positive lymphoplasmacytic cells within the bile duct that leads to symptoms of obstructive jaundice. Secondary causes of obstructive jaundice, PSC, PBC, malignancy and drug-induced causes need to be excluded prior to confirming IgG4-SC. Diagnosis and evaluation of IgG4-SC can be undertaken with serum IgG4-level, characteristic finding on imagings, and possible liver biopsies. Successful treatment of IgG4-SC relies on the compliance to steroid therapy, careful monitoring of blood sugar and side effects of steroids. Alternative treatment may need to be considered in cases of steroid-resistant IgG4-SC. Accurate diagnosis is crucial to avoid delay in diagnosis and treatment, prolonged hospital stay, and risk of unnecessary surgery.
Reference
1. Scheuermann U, Widyaningsih R, Hoppe-Lotichius M, Heise M, Otto G. Detection of benign hilar bile duct stenosis – A retrospective analysis in 250 patients with suspicion of Klatskin tumor. Annals of Medicine and Surgery. 2016; 8: 43-49.
2. Gerhards MF, Vos P, Van Gulik TM, Bosma A, Gouma DJ. Incidence of benign lesions in patients resected for suspicious hilar obstruction. British Journal of Surgery. 2001; 88: 48-51.
3. Okazaki K, Uchida K, Koyaku M, Miyoshi H, Ikeura T, Takaoka M. IgG4- cholangiopathy – Current concept, diagnosis and pathogenesis. Journal of Hepatology. 2014; 61: 690-695.
4. Geary K, Yazici C, Seibold A, Guzman G. IgG4-related cholangiopathy and its mimickers: A case report and review highlighting the importance of early diagnosis. International Journal of Surgical Pathology. 2017; 26: 165-173.
5. Yamagiwa S, Kamimura H, Takamura M, Aoyagi Y. Autoantibodies in primary biliary cirrhosis: Recent progress in research on the pathogenetic and clinical significance. World Journal of Gastroenterology. 2014; 20: 2606-2612.
6. Cai Y, Li HZ, Zhang YS. IgG4-related pseudotumor of the kidney mimicking renal cell carcinoma: A case report. Oncology Letters. 2016; 11: 3438-3440.
7. Futei Y, Amagai M, Ishii K, Kuroda-Kinoshita K, Ohya K, Nishikawa T. Predominant IgG4 subclass in autoantibodies of pemphigus vulgaris and foliaceus. Journal of Dermatological Science. 2001; 26: 55-61.
8. Luu N, Vigil D, Konstantinov KN, Tzamaloukas AH, Sun Y. Tubuloinsterstitial nephritis masquerade as chronic kidney disease. American Journal of Kidney Diseases. 2014; 63: B74.
9. O’Donnell S, O’Morain CA. Therapeutic benefits of budesonide in gastroenterology. Therapeutic advances in Chronic Disease. 2010; 1: 177-186.
10. Culver EL, Barnes E. IgG4-related sclerosing cholangitis. Clinical Liver Disease. 2010; 10: 9-16.
11. Kolfschoten MVD, Schuurman J, Losen M, Bleeker WK, Martinez PM, Vermeulen E, Bleker THD, Wiegman L, Vink T, Aarden LA, Baets MHD, Winkel VD, Aalberse RC, Parren PWHI. Anti-inflammatory activity of Human IgG4 antibodies by dynamic Fab arm exchange. Science. 2007; 317: 1554-1557.
12. Rispens T, Heer POD, Bende O, Aalberse. Mechanism of Immunoglobulin G4 Fab-arm Exchange. Journal of the American Chemical Society. 2011; 133: 10302-10311.
13. Salvadori M, Tsalouchos. Immunoglobulin G4-related kidney diseases: An updated review. World Journal of Nephrology. 2018; 6: 29-40.
14. Guarneri F, Guarneri C, Benvanga S. Helicobacter pylori and autoimmune pancreatitis: role of carbonic anhydrase via molecular mimicry? Journal Cell of Molecular Medicine. 2005; 9: 741-744.
15. Zen Y, Fujii T, Harada K, Yamada K, Takahira M, Nakanuma Y. Th2 and regulatory immune reactions are increased in immunoglobulin G4-related sclerosing pancreatitis and cholangitis. Hepatology. 2007; 45: 1538-1546.
16. Saekia T, Kawano M. IgG4-related kidney disease. Kidney International. 2014; 85: 251-257.
17. Rock B, Martins C, Argyrios N. The pathogenic effect of IgG4 autoantibodies in endemic pemphigus foliaceus. New England Journal of Medicine. 1989; 320: 1463-1469.
18. Forcucci J, Butler-Williams S, Miller N, Lazarchick K. Plasma cell granuloma: An entity within the spectrum of IgG4-related disease. Annual clinical lab science. 2015; 45: 340-343.
19. Kamisawa T, Nakazawa T, Tazuma S, Zen Y, Tanaka A, Ohara H, Muraki T, Inui K, Inoue D, Nishino T, Naitoh I, Itoi T, Notohara K, Kanno A, Kubota K, Hirana K, Isayama H, Shimizu K, Tsuyuguchi T, Shimisegawa T, Kawa S, Chiba T, Okazaki K, Takikawa H, Kimura W, Unno M, Yoshida M. Clinical practice guidelines for IgG4-related sclerosing cholangitis. Journal of Hepato-biliary-pancreatic Sciences. 2019; 26: 9-42.
20. Mittlestaedt A, Meier PN, Dankoweit-Timpe E, Christ B, Jaehne J. IgG4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma (Klatskin tumor): a case report of challenging diagnosis and review of the literature. Innovative Surgical Sciences. 2018; 3: 157-163.
Please view attached pdf to view complete references