Transient Cortical Blindness Post Coronary Angiography: A Case Report
Transient Cortical Blindness Post Coronary Angiography: A Case Report
Tarik Abu Saad 1, Kamal Matli *1,2, Christina Baroudy 1, Antoun Yazbek 1, George Ghanem 1
1.Cardiology, Lebanese American University Medical Center-Rizk Hospital, Beirut, Lebanon.
2.Division of Cardiology, Department of Medicine, University of Montreal Hospital Centre, Montreal, Quebec, Canada.
*Correspondence to: Kamal Matli, Department of Medicine, University of Montreal Hospital Centre, Montreal, Quebec, Canada.
Copyright
© 2024 Kamal Matli. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received:02 February 2024
Published: 15 February 2024
DOI: https://doi.org/10.5281/zenodo.10664550
Abstract
Temporary blindness, also known as transient cortical blindness (TCB), is a rare condition characterized by vision loss after the injection of contrast dye during cerebral and coronary angiography. Although this condition is impermanent, it carries a great deal of stress and discomfort to patients and health care providers. In this report, we present a case of completely reversible TCB post native coronary angiography along with the absence of symptom re-emergence after a downstream rechallenge with contrast dye for a TAVI procedure.
Transient Cortical Blindness Post Coronary Angiography: A Case Report
Introduction
Transient cortical blindness (TCB) refers to the loss of vision secondary to lesions affecting the geniculocalcarine visual pathways [1], and it was first reported as an unusual complication post coronary angiography in 1970 [2]. While the incidence of TCB is rare in cerebral and vertebral angiography, constituting 0.31% [3], it is even lower in coronary angiography with an estimated incidence rate of 0.05% [4]. The exact pathophysiology remains unknown and has mostly been attributed to a toxic reaction of the contrast agent as it penetrates the brain parenchyma through the blood-brain-barrier. Symptoms of TCB may appear immediately during the procedure or up to 12 hours after the procedure, and it tends to show complete resolution within 24 to 48 hours. On brain imaging, there is contrast enhancement in the occipital lobe which can be seen by both magnetic resonance imaging (MRI) and computed tomography (CT) scan, and repeated imaging upon follow-up reveals complete resolution of the contrast [5].
Case Report
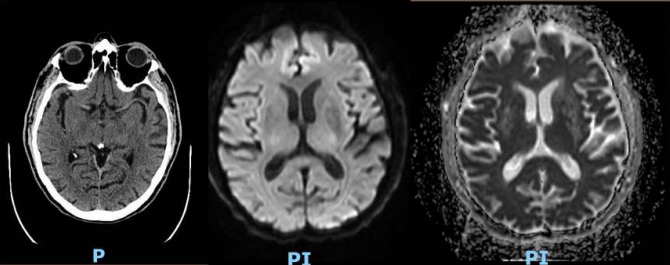
Our patient is an 80 year old gentleman with a prior history of coronary artery disease with previous coronarography 5 years ago on Clopidogrel 75 mg orally once daily, hypertension on Valsartan 80 mg orally once daily, dyslipidemia on Atorvastatin 40 mg orally once daily, allergy to penicillin, and severe symptomatic aortic stenosis stage D1 (high flow-high gradient), presented for coronary angiography in preperation for Transcatherter Aortic Valve Implantation (TAVI). Patient arrived to the catheterization lab hemodynamically stable with a normal creatinine clearance and creatinine level of 0.83 mg/dL. Midazolam 1mg, fentanyl 25 mcg, and heparin 3,500 units were administered intravenously (IV). Radial access technique was adopted. The procedure lasted 25 minutes, and it was smooth and uneventful. Overall, 50 mL of contrast agent, Iodixanol (VISIPAQUE 320 mg/mL) was administered intra-arterially. Findings of the coronary angiography were consistent with diffuse aneurysmal atherosclerosis with some sluggish flow but no significant lesion. In the medical ward, 2 hours after the procedure, the patient started to develop disorientation and attention deficit, progressing rapidly into nausea, bitemporal headache and complete vision loss. Vital signs were in normal ranges and neurological examination revealed intact cerebellar, sensory, motor and reflex powers with normal bilateral pupil reactivity to light. Fundoscopic examination showed normal cup/disk ratio of the optic nerve head with good color and normal clear neuroretinal rim, flat macula with bright reflex and normal color, normal retinal vessels with no hemorrhage and no signs of arterial or venous occlusion, and no retinal detachments or tears. Patient was transferred for an urgent CT and MRI (figure 1) of the brain, which showed minimal small vessel disease and age-related parenchymal atrophy, no acute ischemic or hemorrhagic process identified, and no evidence of retained contrast material.
Patient received 200 mg of hydrocortisone IV once and 500 mL normal saline IV as hydration (given his severe aortic stenosis condition). After 4 hours of his initial symptoms, patient regained his full vision (20/20 in both eyes) with residual color deficit of 25/38 and 30/38 by Ishihara test of right and left eye, respectively. 18 hours after symptom onset, the patient’s vision returned completely back to normal.
A clinical follow-up at one month and three months post-coroangiography showed no recurrance of symptoms; no imaging was done on follow-up because of the normal findings of the initial tests. Moreover, at one month post-coroangiography, the patient underwent TAVI and CT TAVI, and we administered premedications that consisted of intravenous steroids (i.e. hydrocortisone) before rechallenging the contrast agent that is indicated for said procedures. The patient did not experience any sequelae or complications afterwards.
Figure 1: A- Axial cut of CT scan without contrast. B- Axial Diffusion-weighted imaging. C- Apparent diffusion coefficient map
Discussion
Diagnostic coronary angiography is considered a low risk invasive procedure with possible complications divided into coronary vascular injury, other vascular events, and systemic nonvascular events. Major adverse cardiac and cerebrovascular events include death, stroke, and myocardial infarction. Additional complications include bleeding, nephropathy, atheroembolism, allergic reactions, and arrhythmia [6]. TCB is one of the rarest, but recognized complication following coronary angiography. It is the first case to be reported at our catheterization laboratory.
While the exact mechanism and pathophysiology remain unknown, it has mostly been attributed to a toxic reaction of the contrast agent as it penetrates the brain parenchyma through the blood-brain-barrier. It has been reported that the intrinsic vulnerability of the occipital cortex, secondary to reduced sympathetic innervation and lack of protective sympathetic mediated arteriolar vasoconstriction, may account for the increased frequency of its involvement [7].
While the amount of contrast administered might be a debatable risk factor for TCB incidence; the hyperosmolarity, viscosity, and solubility characteristics of the contrast agent are more likely thought to contribute to the increased neurotoxicity of the dye [8]. Iodixanol (Visipaque) that the patient received has a lower osmolality and causes less disruption to the blood-brain-barrier. Other contrast agents have higher incidence of neurotoxicity [9]. The adverse drug reaction of the contrast is considered to be direct idiosyncratic neurotoxicity [10], and it is associated with the following risk factors: uncontrolled hypertension, hypoventilation, immunological mechanisms, and renal insufficiency [11]. LIMA to LAD graft was also identified as another risk factor for TCB [12]. However, in our case, the patient has a history of a previous uncomplicated coronarography and a previous exposure to contrast; hence, these factors do not seem to prevent the development of TCB in a repeated administration of the dye [5,11,13].
Symptoms of TCB may appear immediately during the procedure or up to 12 hours after the procedure. Symptoms consists of blurry vision, headache [14], disorientation [13], retrograde amnesia [15], nausea, vomiting, decreased level of consciousness, reaching sudden complete blindness [16]. An additional complication that was witnessed in our case was color blindness (red and green) of 25/38 right and 30/38 left as assessed by Ishihara test that completely resolved within 14 hours. An acute ischemic process, whether it is embolic or secondary to hypoperfusion to watershed areas in the brain, is high on the differential, especially in patients undergoing cardiac catheterization where there is risk of microembolization [17]. Embolic complications can either present silently or with neurological deficit8 which is not our case. The presence of normal fundoscopic examination, lack of neurological deficit, absence of ischemic process on MRI, and rapid resolution of the symptoms, suggests the absence of anterior or posterior ischemic optic neuropathy (AION/PION) or any other optic nerve or paranchymal ischemic process.
MRI is considered the diagnostic imaging of choice to detect ischemic changes in early stages, particularly in cases of periprocedural cortical blindness. In TCB, there is contrast enhancement in the occipital lobe which can be seen by both MRI and CT, and repeated imaging on follow up reveals complete resolution of the contrast [11]. However, a normal brain imaging does not rule out the diagnosis since there are multiple reports of TCB with negative imaging findings [18,19,20].
Although the rate of recurrance of TCB is not well established, it is advised to premedicate patients with a history of TCB using steroids and minimize the amount of dye in future re-exposure [5,12], which is what we did for our patient, before both CT TAVI and TAVI procedures.
Conclusion
TCB is a rare post coronary angiographic complication, that presents with complete resolution of the symptoms within 24 to 48 hours. It is a clinical diagnosis guided by signs of contrast enhancement in the occipital area by brain imaging, which is crucial to rule out other causes such as ischemic process or bleed. However, in our case, the patient presented with temporary blindness with negative brain imaging findings; his symptoms recovered completely within 18 hours. Although there appears to be no increased risk on future exposure[13], a plausible prevention for recurrence is to premedicate with steroids and reduce contrast agent volume administration.
Reference
1. Aldrich MS, Alessi AG, Beck RW, Gilman S. Cortical blindness: etiology, diagnosis, and prognosis. Ann Neurol. 1987;21(2):149-158. doi:10.1002/ana.410210207
2. Fischer-Williams M, Gottschalk PG, Browell JN. Transient cortical blindness. An unusual complication of coronary angiography. Neurology. 1970;20(4):353-355. doi:10.1212/wnl.20.4.353
3. Studdard WE, Davis DO, Young SW. Cortical blindness after cerebral angiography. Case report. Journal of neurosurgery. 1981;54:240-244.
4. Kinn RM, Breisblatt WM. Cortical blindness after coronary angiography: a rare but reversible complication. Cathet Cardiovasc Diagn. 1991;22(3):177-179. doi:10.1002/ccd.1810220305
5. Balasingam S, Azman RR, Nazri M. Contrast media induced transient cortical blindness. QJM. 2016;109(2):121-122. doi:10.1093/qjmed/hcv121
6. Bashore TM, Balter S, Barac A, et al. 2012 American College of Cardiology Foundation/Society for Cardiovascular Angiography and Interventions expert consensus document on cardiac catheterization laboratory standards update: A report of the American College of Cardiology Foundation Task Force on Expert Consensus documents developed in collaboration with the Society of Thoracic Surgeons and Society for Vascular Medicine. J Am Coll Cardiol. 2012;59(24):2221-2305. doi:10.1016/j.jacc.2012.02.010
7. Borghi C, Saia F, Marzocchi A, Branzi A. The conundrum of transient cortical blindness following coronary angiography. J Cardiovasc Med (Hagerstown). 2008;9(10):1063-1065. doi:10.2459/JCM.0b013e3282fe1718
8. Al-irr K, Transient Cortical Blindness Following Coronary Angiography, J Clin Exp Cardiolog. 2016; 7(4). doi: 10.4172/2155-9880.1000435
9. Pramod Theetha Kariyanna, Lyudmila Aurora, Amog Jayarangaiah, Sushruth Das, Jose Casillas Gonzalez, Sudhanva Hegde and Isabel M. McFarlane. Neurotoxicity Associated with Radiological Contrast Agents Used during Coronary Angiography: A Systematic Review. American Journal of Medical Case Reports. 2020; 8(2):60-66. doi: 10.12691/ajmcr-8-2-6
10. Mouine N, Ndom MS, El Hankari T, Zbir M. Transient cortical blindness after coronary angiography: report of 2 cases. Journal of Men's Health. 2010; 7(4):431-433. http://doi.org/10.1016/j.jomh.2010.09.224
11. Alp BN, Bozbuga N, Tuncer MA, Yakut C. Transient cortical blindness after coronary angiography. J Int Med Res. 2009;37:1246–51.
12. Frantz WM. Cortical blindness following coronary angiography in a patient with LIMA bypass graft and end stage renal failure; Proceedings of EuroPCR; Paris: 2006. May 21-24
13. Lara JG, Vázquez-Rodríguez JM, Salgado-Fernández J, et al. Transient cortical blindness following cardiac catheterization: an alarming but infrequent complication with a good prognosis. Rev Esp Cardiol. 2008;61:88–90.
14. Rama BN, Pagano TV, DelCore M, Knobel KR, Lee J. Cortical Blindness after cardiac catheterization: effect of rechallenge with dye. Cathet Cardiovasc Diagn. 1993;28:149–51.
15. Sticherling C, Berkefeld J, Auch-Schwelk W, Lanfermann H. Transient bilateral cortical blindness after coronary angiography. Lancet 1998;351:570.
16. Henzlova MJ, Coghlan HC, Dean LS, et al. Cortical blindness after left internal mammary artery to left anterior descending coronary artery graft angiography. Cathet Cardiovasc Diagn. 1988; 15(1): 37–39.
17. Tavakol M, Ashraf S, Brener SJ. Risks and complications of coronary angiography: a comprehensive review. Glob J Health Sci. 2012;4:65–93.
18. Baguma M, Younan N, London F, Ossemann M, Vandermeeren Y. Contrast-associated transient cortical blindness: three cases with MRI and electrophysiology findings. Acta Neurol Belg. 2017;117(1):195-199.
19. Oktaviono YH, Kawilarang MV, Kawilarang M et al. Case Report: Transient cortical blindness following coronary angiography [version 1; peer review: 1 approved with reservations]. F1000Research 2021, 10:439 (https://doi.org/10.12688/f1000research.50821.1)
20. Fernandes SIL, Carvalho RJR, Santos LMG, et al. Transient Cortical Blindness Following Coronary Angiography. JACC Case Rep. 2019;1(2):188-191. Published 2019 Aug 21. doi:10.1016/j.jaccas.2019.06.014.