Asbestosis Situation and Severity in the Era of COVID-19 Pandemic : A Systematic Review and Meta-Analysis
Asbestosis Situation and Severity in the Era of COVID-19 Pandemic : A Systematic Review and Meta-Analysis
Ruangrong Cheepsattayakorn1, Attapon Cheepsattayakorn 2,3,4,5*, Porntep Siriwanarangsun 3
1. Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
2. Faculty of Medicine Vajira Hospital, Navamindradhiraj, Bangkok, Thailand
3. Faculty of Medicine, Western University, Pathumtani Province, Thailand.
4. 10th Zonal Tuberculosis and Chest Disease Center, Chiang Mai, Thailand.
5. Department of Disease Control, Ministry of Public Health, Thailand.
Correspondence to: Attapon Cheepsattayakorn, 10th Zonal Tuberculosis and Chest Disease Center, 143 Sridornchai Road Changklan Muang Chiang Mai 50100 Thailand Tel : 66 53 140767 ; 66 53 276364 ; Fax : 66 53 140773 ; 66 53 273590 ; Email : Attapon1958@gmail.com.
Copyright
© 2024 Attapon Cheepsattayakorn. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 February 2024
Published: 27 February 2024
Abstract
A comprehensive search was carried out in mainstream bibliographic databases or Medical Subject Headings, including ScienDirect, PubMed, Scopus, and ISI Web of Science. The search was applied to the articles that were published between 2003 and early 2024. With strict literature search and screening processes, it yielded 3 articles from 64 articles of initial literature database. Asbestos, a heterogenous group of hydrated magnesium silicate minerals with a tendency of fiber separation. Asbestos-associated pleural fibrosis (pleural plaque or diffuse plural fibrosis), pleural thickening, or asbestosis are the majority of nonmalignant-asbestos-associated-disease conditions. Nevertheless, there is close association between of the nonmalignant-disease presence and the malignancy risk, particularly, lung cancer (complicated with pleural or peritoneal mesothelioma and cigarette smoking). One of search study clearly demonstrated rising trend of mortality in people aged 80 years and older among the three search studies, whereas COVID-19 pneumonia patients requiring respiratory support were higher among patients with history of asbestos exposure or asbestosis, compared to unexposed-asbestos patients (p = 0.015).
In conclusion, The detection of an independent relation in small sample of subjects may be precluded by confounding covariables, such as smokers, having more comorbidity, more frequently male, and older age. In occupational asbestos exposure, respiratory support was required higher, compared to unexposed-asbestos patients. Proactive and cooperative participation can protect people with asbestos exposure from COVID-19 comorbidity.
Keywords: asbestos, asbestosis, COVID-19, situation, severity, exposure, SARS-CoV-2
Asbestosis Situation and Severity in the Era of COVID-19 Pandemic : A Systematic Review and Meta-Analysis
Abbreviations : COVID-19 : Coronavirus-2019, FEV1 : Forced Expiratory Volume in one second, FVC: Forced Vital Capacity, ILDs : Interstitial Lung Diseases, IPF : Idiopathic Pulmonary Fibrosis, p : Probability, SARS-CoV-2 : Severe Acute Respiratory Syndrome-Coronavirus-type 2, US : United States, USA : United States of America
Objectives of the Study
The objectives of this study are to identify the better understanding on the situation and severity of asbestosis and asbestos exposure in the era of COVID-19 pandemic.
Introduction
Asbestos, a heterogenous group of hydrated magnesium silicate minerals with a tendency of fiber separation [1]. Asbestos-associated pleural fibrosis (pleural plaque or diffuse plural fibrosis), pleural thickening, or asbestosis are the majority of nonmalignant-asbestos-associated-disease conditions [1]. Nevertheless, there is close association between of the nonmalignant-disease presence and the malignancy risk, particularly, lung cancer (complicated with pleural or peritoneal mesothelioma and cigarette smoking) [1]. Without obvious clinical signs of nonmalignant asbestos-associated diseases, increased personal cancer risk with prolonged asbestos exposure can be occurred, implying a lifelong increased asbestos-associated-cancer risk [1]. From the general diagnostic-asbestosis criteria established in 1986, they were slightly modified as the following : 1) evidence of structural pathology consistent with asbestos-associated disease as evidenced by histology or imaging; 2 evidence of causation by asbestos as documented by the environmental and occupational history, exposure markers (majority of pleural plaques), and recovery of asbestos bodies, or other means; and 3) exclusion of alternative plausible causes for the findings [1]. It was noticed that during COVID-19 pandemic, chronic-lung-disease patients with comorbidities had tendency to have more severe COVID-19 and more complications [2]. Interstitial lung diseases (ILDs) can result from drug, environmental, or occupational exposures and can be manifested in an underlying systemic diseases [2], especially, idiopathic pulmonary fibrosis (IPF) is related to viral infections and thoracic surgical procedures with acute exacerbation and high mortality rates of 35 %-70 % [3]. Approximately, 1.4 % of global prevalence of ILDs among global COVID-19 patients was seen [4]. ILD patients with non-survival COVID-19 had high mortality rates (two times), compared with non-ILDs [4]. In idiopathic pulmonary fibrosis (IPF), the fibroblastic foci are characterized, but are infrequent in asbestosis [5]. Whereas mild fibrosis of the visceral pleura is commonly accompanied in asbestosis, this feature is rare in IPF [5]. Very little inflammation is identified in interstitial fibrosis of asbestosis whereas it is better found in IPF [5].
Methods of the Study
Search Strategy and Inclusion Criteria
A comprehensive search was carried out in mainstream bibliographic databases or Medical Subject Headings, including ScienDirect, PubMed, Scopus, and ISI Web of Science. The search was applied to the articles that were published between 2003 and early 2024. Our first involved performing searches of article abstract/keywords/title using strings of [(“ Asbestos ” or “ Asbestosis ”, “ SARS-CoV-2 ” or “ COVID-19 ” and “ Severity ” or “ Exposure ”, “ Plaque ” or “ Pleural Thickening ” or “ Pleural Calcification ”, “ Peritoneal Plaque ” or “ Peritoneal Calcification ”, “ Calcified Peritoneum ”)]. After a first approach of search, published articles focusing on asbestos-associated diseases or asbestosis were retained and the information on situation and severity and COVID-19 or SARS-CoV-2 comorbidity and severity was extracted for having a crude knowledge involving their themes. Another round of publication search was conducted for adding the missing published articles that were not identified by the first round.
All keywords combinations from one asbestos-associated disease type and COVID-19 or SARS-CoV-2 variables to bind the population of cases under consideration. Search string for asbestos-associated diseases included [ “ Pleural Plaque” or “ Pleural Thickening ” or “ Pleural Calcification ” or “ Peritoneal Plaque ” or “ Peritoneal Calcification ” or “ Lung Cancer ” or “ Nonmalignant asbestos-associated disease ” or “ Interstitial-Lung-Disease-Associated Asbestos Exposure ” or “ Occupational Asbestos Exposure ” or “ Environmental Asbestos Exposure ” ]. The initial literature databases were further manually screened with the following rules : 1) non-asbestos-exposure-associated-disease-related articles were excluded; 2) articles that did not report a result of asbestos-associated diseases or conditions related to COVID-19 exposure or comorbidity were not considered, such as commentary articles, or editorial; 3) non-peer reviewed articles were not considered to be of a scholarly trustworthy validity; and 4) duplicated and non-English articles were removed. The articles were carefully selected to guarantee the literature quality, which is a trade-off for quantity.
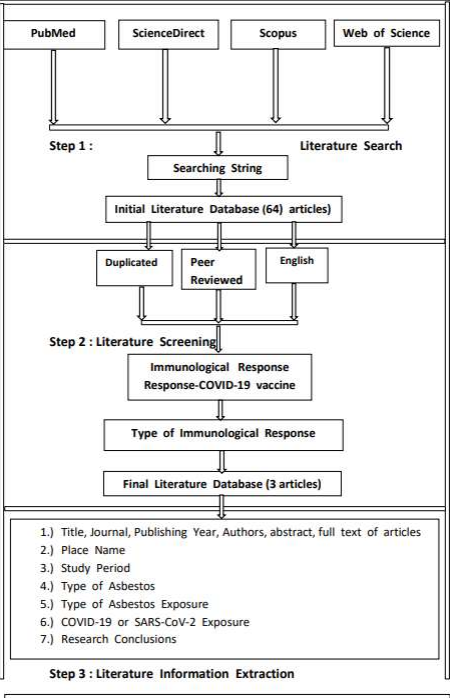
With strict literature search and screening processes, it yielded 3 articles from 64 articles of initial literature database. Needed article information was extracted from each article by : 1) direct information including journal, title, authors, abstract, full text documents of candidate studies, publishing year; 2) place name of the study area; 3) study period; 4) research method used; 5) types of asbestos variables studied; 6) types of asbestos exposure studied; 7) COVID-19 or SARS-CoV-2 comorbidity and situation; and 7) the conclusions made about the impacts of asbestos-associated diseases or conditions related to COVID-19 or SARS-CoV-2 comorbidity and situation. An overview of the information required for the present analysis that was captured by those themes was demonstrated in the Figure 1.
Figure 1: Literature Search and Screening Flow
Results
Table 1 : Demonstrating the asbestos-associated diseases or conditions impacted by COVID-19 or SARS-CoV-2 comorbidity (2021-to early-2024)
Please click here to view table
Discussion
One of the three search studies [6-8] clearly demonstrated rising trend of mortality in people aged 80 years and older [6], whereas COVID-19 pneumonia patients requiring respiratory support were higher among patients with history of asbestos exposure or asbestosis, compared to unexposed-asbestos patients (p = 0.015) [7]. During and after hospitalization, the association between main studied variables and occupational asbestos exposure demonstrated significantly higher percentage of requiring respiratory-support patients [7]. Except for a lower FEV1/FVC in asbestos-exposed patients, no different spirometry parameters were detected [7]. Asbestos-exposed patients with COVID-19 comorbidity presented more intense dyspnea, compared to unexposed patients [7]. In the univariate analysis, asbestos exposure was related to severe COVID-19 [7]. Nevertheless, in the logistic multivariate regression analysis, this hypothesis could not be confirmed [7]. In asbestos-exposed patients, other more frequent variables were cigarette smoking, male predominance, older age, respiratory and cardiological pathologies, and history of diabetes [7]. Currently, the study of association between exogenous-agent-inhalation exposure and the COVID-19 severity has been concentrated on environmental contamination [9]. Approximately, 92 % of the US Lincoln county population with asbestos exposure and chronic pulmonary diseases had been protected from COVID-19 infection or comorbidity by proactive and cooperative participation of their residents with unknown asbestosis situation and severity in the period of COVID-19 pandemic [8].
Conclusion
The detection of an independent relation in small sample of subjects may be precluded by confounding covariables, such as smokers, having more comorbidity, more frequently male, and older age. In occupational asbestos exposure, respiratory support was required higher, compared to unexposed-asbestos patients. Proactive and cooperative participation can protect people with asbestos exposure from COVID-19 comorbidity.
Authors Contributions
Dr. Attapon Cheepsattayakorn conducted the study framework and wrote the manuscript. Associate Professor Dr. Ruangrong Cheepsattayakorn and Professor Dr. Porntep Siriwanarangsun contributed to scientific content and assistance in manuscript writing. All authors read and approved the final version of the manuscript.
Competing Interests: The authors declare that they have no actual or potential competing financial interests.
Funding Sources: The authors disclose no funding sources.
References
1.American Thoracic Society (ATS). Diagnosis and initial management of nonmalignant diseases related to asbestos. The official statement of the American Thoracic Society, adopted by the ATS Board of Directors on December 12, 2003.
2.Azadeh N, Limper AH, Carmona EM, Ryu JH. The role of infection in interstitial lung diseases : a review. Chest 2017; 152 : 842-852. DOI : 10.1016/j.chest.2017.03.033
3.Drake TM, Docherty AB, Harrison EM, Quint JK, Adamali H, Agnew S, et al. Outcome of hospitalization for COVID-19 in patients with interstitial lung disease : an international multicenter study. Am J Respir Crit Care Med 2020; 202 : 1656-1665. DOI : 10.1164/rccm.202007-2794OC
4.Ouyang L, Gong J, Yu M. Pre-existing interstitial lung disease in patients with coronavirus disease 219 : a meta-analysis. Int Immunopharmacol 2021; 100 : 108145. DOI : 10.1016/j.intimp.2021.108145
5.Roggli VL, Gibbs AR, Attanoos R, Churg A, Popper H, Cagle P, et al. Pathology of asbestosis-an update of the diagnostic criteria. Arch Pathol Lab Med 2010; 134 (3):462-480. DOI: 10.5858/134.3.462.
6.Fazzo L, Grande E, Zona A, Minelli G, Crialesi R, Lavarone I, et al. Mortality rates from asbestos-related diseases in Italy during the first year of the COVID-19 pandemic. Frontiers in Public Health 2024. Published on January 16, 2024. DOI : 10.3389/fpubh.2023.1243261
7.Granados G, Sa?ez-Lo?pez M, Aljama C, Sampol J, Cruz M-J, Ferrer J, et al. Asbestos exposure and severity of COVID-19. International Journal of Environmental Research and Public Health 2022; 19 : 16305.DOI : https://doi.org/10.3390/ijerph192316305
8.McNew T, Morrissette KL, Black B. Controlling COVID-19 in an asbestos-exposed population. Chest 2021 annual meeting. October 17-20, 2021. 1927A.
9.Wu X, Nethery RC, Sabath MB, Braun D, Dominici F. Air pollution and COVID-19 mortality in the United States : strengths and limitations of an ecological regression analysis. Si Adv 2020; 6 : eabd4049.