Impact of COVID-19 Social Restrictions on Foreign Body Ingestion Rates in the Pediatric Population: A Decade in Review
Impact of COVID-19 Social Restrictions on Foreign Body Ingestion Rates in the Pediatric Population: A Decade in Review
Aniruddh Setya, MD *1, Priyanka Nair MD 2, Zalan Shah MD 3
1. Pediatric Gastroenterology, Saint Louis University School of Medicine and SSM Health Cardinal Glennon, MO, USA .
2. Pediatric Emergency Medicine, Washington University School of Medicine, Saint Louis, MO.
3. Saint Louis University School of Medicine, Saint Louis, MO.
*Correspondence to: Aniruddh Setya, MD, Pediatric Gastroenterology, Saint Louis University School of Medicine and SSM Health Cardinal Glennon, MO, USA.
Copyright
© 2024 Aniruddh Setya. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 February 2024
Published: 28 February 2024
Abstract
Introduction:
This retrospective study analyzes a decade of data (2012-2022) from a southern Florida tertiary care center to assess the impact of COVID-19-related social restrictions on pediatric foreign body ingestion (FBI) rates, with a focus on battery ingestions.
Methods:
Data, including annual esophagogastroduodenoscopy (EGD) rates and specific FBI cases, was collected from the Electronic Health Record system. Statistical analysis compared pre-COVID (2012-2019) and post-COVID (2019-2022) periods using a two-section T-test.
Results:
A significant increase in FBI rates and in battery ingestions occurred during the pandemic (2020-2021). While rates declined in 2022, they remained elevated compared to pre-pandemic levels. The post-COVID increase in FBIs, % FBI of EGD, battery ingestions, and % battery ingestions of EGD were statistically significant.
Discussion:
Pandemic-induced lifestyle changes increased indoor activities and reduced supervision which likely contributed to the elevated FBI rates. The persistence of elevated rates in 2022 suggests lasting behavioral changes post-lockdown.
Conclusion:
This study reveals a significant increase in pediatric FBI, particularly in battery ingestions, during and after the COVID-19 pandemic. The lasting impact of pandemic-induced lifestyle changes underscores the need for continued public health education and regulatory measures to protect children from foreign body ingestions.
Impact of COVID-19 Social Restrictions on Foreign Body Ingestion Rates in the Pediatric Population: A Decade in Review
Introduction
Foreign body ingestion (FBI) is an accidental ingestion of an object into the respiratory tract. General guidelines for FBI entail using radiography to confirm the presence of the foreign body, and endoscopic removal of the object is recommended if it is in the esophagus or is symptomatic, large, and/or sharp located prior to the duodenal sweep [1].
More prevalent in children, FBIs can cause significant harm and potentially be fatal, representing the leading cause of death among infants and the fourth for preschool-aged children [2]. Absent or inadequate supervision is a factor associated with increased risk of FBIs, approximately 40% of FBIs are unwitnessed [1, 3].
In March 2020, lockdowns and social distancing were widely implemented to mitigate the spread of COVID-19 [4]. This resulted in significant lifestyle changes for children including decreased physical activity, increased feelings of boredom, more time spent indoors, and decreased supervision; children of essential workers were especially vulnerable to these consequences [4]. These conditions could have increased FBIs in the pandemic years of 2020 and 2021.
Of the various items that children can ingest, button batteries are of particular concern, given the prevalence of batteries in households with children has been increasing [5]. Button batteries are small single-celled batteries with positive and negative terminals at their ends, and their ingestion can cause severe esophageal damage and mortality [5]. Increased mortality of button battery ingestion cases has been observed in the two decades before 2010 with many surviving patients suffering injuries post removal of ingested batteries such as esophageal-tracheal fistula, esophageal perforation, and esophageal stenosis [2, 6].
The purpose of this study was to evaluate the impact of the social restrictions of the COVID-19 lockdown on FBI rates by comparing data before and after the start of the pandemic as well as to assess trends related to FBI in the pediatric population over ten years (2012-2022), with a specific focus on battery ingestion. This study is unique in that no prior studies have assessed data about FBIs over ten years, including data after pandemic restrictions were lifted.
Materials and Methods
Study Population: This retrospective study evaluated cases within a singular tertiary care center in southern Florida within ten years between 2012 and 2022. Individuals below the age of 21 were included in this study.
Data Collection: The data was collected using the Electronic Health Record system. The variables of interest included the total number of esophagogastroduodenoscopies (EGDs) performed annually by the pediatric gastroenterologist, total cases of FBI and battery ingestions, and the percentage of FBI and battery ingestions relative to the total number of annual EGDs (% FBI of EGD and % battery ingestion of EGD))
Statistical Analysis: The study categorized data into pre-COVID (2012-2019) and post-COVID (2019-2022) periods. A two-section T-test was used to determine the significance between the two groups within the variables of interest. The significance level was set at p = 0.05.
Results and Discussion
Table 1. Data collected from electronic health record on performed esophagogastroduodenoscopies (Annual EGD), including total foreign body ingestion cases (Total FBI), percentage of FBI of all performed EGDs (%FBI of EGD), total battery ingestion cases (Total Battery Ingestions), and percentage of battery ingestions of all performed EGDs (% Battery Ingestions of EGD).
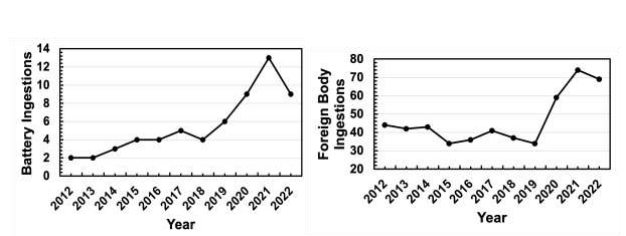
Between 2012 and 2019, the annual rates of FBI fluctuated between 4-6% of total EGDs. A notable rise in FBI occurred in the pandemic years of 2020 (11%) and 2021 (12%), followed by a decrease in 2022 (9%) which still exceeded the pre-pandemic rates. Among the FBI cases, the number of battery ingestion cases ranged from 2 to 6 annually up until 2019. A distinct surge was observed in 2020 (9 cases) and 2021 (13 cases), before showing a decline in 2022 (9 cases). ?
Figure 1. Total cases of foreign body ingestions (FBI) and battery ingestions from 2012 to 2022.
Overall, the trend present in the data showed a consistent rate of FBI and battery ingestions before the pandemic years, a significant spike during the pandemic, followed by a return to the pre-pandemic values following the pandemic (Figure 1).
Table 2. Averages and p-values of total foreign body ingestion cases (Total FBI), percentage of FBI of all performed EGDs (%FBI of EGD), total battery ingestion cases (Total Battery Ingestions), and percentage of battery ingestions of all performed EGDs (% Battery Ingestions of EGD) are displayed, comparing pre-covid years (2012-2019) and post-covid years (2020-2022).
Relative to the pre-COVID period, there was a significant increase in cases of FBIs (p < 0.001), % FBI of EGD (p < 0.001), cases of battery ingestions (p < 0.001), and % FBI of EGD (p < 0.001) post-COVID (Table 2). This data agrees with multiple prior studies that have also found that foreign body ingestions and button battery ingestions increased significantly after the start of the pandemic in 2020 [7, 8, 9 and 10]. These increases could have been a result of the increased time indoor activities and decreased adult supervision caused by the pandemic lockdown that took place from 2020-2021[4].
The spike in button battery ingestion cases could have also been facilitated by the long-term trend of increased prevalence, size, and voltage of button batteries in children’s toys and household electronics [5]. These existing trends would have been further exacerbated by pandemic conditions where children spent more time at home and unsupervised with these battery devices [4].
In 2022, when pandemic lockdown restrictions were no longer in place, the values for FBI and battery ingestion remained elevated relative to the pre-covid baseline values. This could be indicative of lasting behavior and lifestyle changes after the conclusion of lockdowns and social distancing, and further emphasizes the urgency to address this significant safety concern for children. Public health measures to increase education about the dangers of button batteries to caregivers and regulate the use of batteries in children's products are needed.
The results of this study were limited due to its retrospective, single-center design. A literature review evaluating multiple studies on FBI elevation post-COVID is needed to make conclusions about FBI trends more confidently.
Conclusion
Comparing pre-COVID to post-COVID periods, there was a significant increase in cases of FBIs (p < 0.001), % FBI of EGD (p > 0.001), cases of battery ingestions (p < 0.001), and % Battery Ingestions of EGD (p < 0.001). This could be an indication that the lifestyle changes children undertook in the COVID-19 pandemic enabled these incidents.
While the cases for FBI and battery ingestion fell in 2022, they remained elevated relative to pre-pandemic levels which indicates that the effects of pandemic-induced lifestyle changes on child safety may be lasting. The findings underscore the ongoing need for preventive public health measures, including improved caregiver education, and stronger safety regulations for children's products.
Reference
1. Uyemura MC. Foreign body ingestion in children. Am Fam Physician. Jul 15 2005;72(2):287-91.
2. Salih AM, Alfaki M, Alam-Elhuda DM. Airway foreign bodies: A critical review for a common pediatric emergency. World J Emerg Med. 2016;7(1):5-12. doi:10.5847/wjem.j.1920-8642.2016.01.001
3. Montana A, Salerno M, Feola A, et al. Risk Management and Recommendations for the Prevention of Fatal Foreign Body Aspiration: Four Cases Aged 1.5 to 3 Years and Mini-Review of the Literature. Int J Environ Res Public Health. Jun 30 2020;17(13)doi:10.3390/ijerph17134700
4. Pfefferbaum B. Challenges for Child Mental Health Raised by School Closure and Home Confinement During the COVID-19 Pandemic. Curr Psychiatry Rep. Aug 16 2021;23(10):65. doi:10.1007/s11920-021-01279-z
5. Bolton SM, Saker M, Bass LM. Button battery and magnet ingestions in the pediatric patient. Current Opinion in Pediatrics. 2018;30(5):653-659. doi:10.1097/mop.0000000000000665
6. Litovitz T, Whitaker N, Clark L, White NC, Marsolek M. Emerging battery-ingestion hazard: clinical implications. Pediatrics. Jun 2010;125(6):1168-77. doi:10.1542/peds.2009-3037
7. Klein LJ, Black K, Dole M, Orsagh-Yentis DK. Epidemiology of Pediatric Foreign Body Ingestions Amidst the Coronavirus 2019 Pandemic at a Tertiary Care Children's Hospital. JPGN Rep. Feb 2022;3(1):e168. doi:10.1097/pg9.0000000000000168 - only FBI
8. Pizzol A, Rigazio C, Calvo PL, et al. Foreign-body Ingestions in Children During COVID-19 Pandemic in a Pediatric Referral Center. JPGN Rep. Nov 2020;1(2):e018. doi:10.1097/pg9.0000000000000018 - both battery and FBI
9. Festa NT, Thakkar H, Hewitt R, et al. Foreign body ingestion during the COVID-19 pandemic: a retrospective single centre review. BMJ Paediatr Open. 2021;5(1):e001042. doi:10.1136/bmjpo-2021-001042

10. Neal JT, Monuteaux MC, Porter JJ, Hudgins JD. The Effect of COVID-19 Stay-At-Home Orders on the Rate of Pediatric Foreign Body Ingestions. J Emerg Med. Dec 2022;63(6):729-737. doi:10.1016/j.jemermed.2022.09.019.