Detecting Progressive Disease: Genomic Alterations Associated with no Response to Immune Checkpoint Inhibitors
Detecting Progressive Disease: Genomic Alterations Associated with no Response to Immune Checkpoint Inhibitors
Lucia Ceniceros *1, Eduardo Castañon 2
1.Oncology department, Clinica Universidad de Navarra, Madrid, Spain;
2.Clinical Trials Unit, Clinica Universidad de Navarra, Madrid, Spain;
*Correspondence to: Lucia Ceniceros. Oncology department, Clinica Universidad de Navarra, Madrid, Spain;
Copyright.
© 2024 Lucia Ceniceros. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 February 2024
Published: 28 February 2024
DOI: https://doi.org/10.5281/zenodo.14185469
ABSTRACT
In the last decade, different immune checkpoint inhibitors (ICI) have been investigated to improve the survival of cancer patients. The novel development of oncolytic viruses, cancer vaccines, target therapies e.g. against TIGIT, anti-LAG3 and well-known anti-PD1/PDL-1 or antiCTLA-4 are creating a new era in oncology. However, these drugs only benefit a small group of patients. Since the beginning of the development of these agents, unconventional patterns of response have been observed. It is the case of pseudoprogression, hyperprogression or durable response. Additionally, various molecular characteristics may adversely affect the effectiveness of immune checkpoint inhibitors (ICI). At present, there is no validated biomarker that can accurately predict a patient's response to ICI. Therefore, there is a pressing need to identify individuals who are likely to respond or not respond to immunotherapy, in order to provide them with the most suitable treatment option. This review aims to summarize emerging markers that can be utilized to differentiate between responders and non-responders to immunotherapy.
Keywords: Immunotherapy, Immune Checkpoint Inhibitors, Mechanism, Resistance, Biomarkers
Detecting Progressive Disease: Genomic Alterations Associated with no Response to Immune Checkpoint Inhibitors
Introduction
Checkpoint blockade immunotherapy has become a mainstay of cancer therapy. Immune checkpoint inhibitors against the programmed cell death (PD-1) or its ligand programmed death-ligand (PDL-1) and against the cytotoxic T-Lymphocyte-associated antigen 4 (CTLA-4) are standard treatments in multiple tumours as non-small cell lung cancer, renal cell carcinoma (RCC), melanoma and other tumours [1-3]. Other indications of ICI have been approved based on molecular tumor characteristics. Such is the case of FDA approval pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastasic tumor mutational burden-high (TMB-H); considered TMB-High >= 10 mutations per megabase [4]. Nevertheless, only 20% treated with immunotherapy respond to immune checkpoint blockade and a significant proportion of patients develop resistance or refractories to treatment during therapy [5].
The human cells have a set of capabilities to make their way form normalcy to form malignant tumors. The complexity of cancer phenotypes and genotypes determine the steps of tumor pathogenesis and response of treatments [6]. The recent years have seen a substancial effort in the development of new technologies focused on the molecular analysis of tumors, enabling the detection of a wide range of alterations. These alteracions may have survival implications, know as prognosctic biomarkers, and therapeutic implications, referred to as predictive biomarkers. While our ability to predict therapeutic benefits has advanced through the development of tumor and patient cancer specific biomarkes, there remains an unmet clinical need to establish a standard biomarker [7].
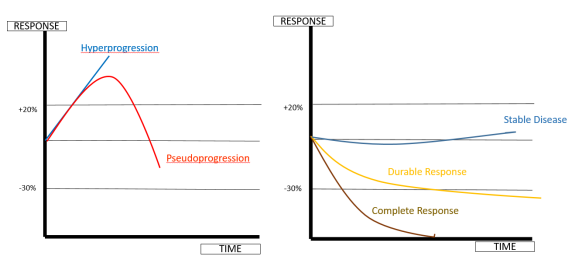
With the introduction of ICI, unconventional patterns of response have been observed, such as durable response, dissociated response, pseudoprogression and hyperprogression (Figure 1). Dissociated response is defined as the coexistence of responding and non-responding lesions within the same patient. Pseudoprogression (PD) is described as an objective response after an initial disease progression with the same treatment, while hyperprogression (HP) is the reported acceleration of tumor growth after initiation of immunotherapy [8]. The observation that certain patients achieve a plateau in their response following immunotherapy treatment suggests that, in some cases, the tumors may undergo long-term remission. In such instances, the disease´s progression and prognosis are more favourable than initially anticipated at the time of diagnosis. The longest information of this durable response was seen in melanoma patients with nivolumab and ipilimumab combination [9].

Figure 1. Patterns of response.
Different patterns of response can be achieved with immunotherapy as despicted in this figure. Hyperprogression: Accelerated tumor growht or worsening of the disease after tratment, beyond what is expected. Pseudoprogression: Initial apparent increase in tumor size that is later revealed to be treatment-related inflammation rather than actual disease progression. Stable Disease: The tumor size remains relatively constant over a period, indicating that the disease is neither progressing. Durable Response: Sustained positive response to treatment with long-lasting effectiveness. Complete Response: total disappearance of all signs of tumor disease.
Due to the worse outcome in patients who present HP, it is necessary to understand the underlying mechanism. However, it remains unclear. Some hypothesis assume that immune checkpoint inhibitors induce the expansion of PD1+ regulatory T-cells, exhaustion of cytotoxic T-cells, modulation of pro-tumorigenic immune cell subsets, activation of aberrant inflammation or activation of oncogenic signalling [9]. HP has been described in several studies [10-12]. This phenomenom is not rare, varying from 9% to 40% due to the lack of an accurate definition [13-14]. Some authors used a radiological criteria based on the variation of three-dimensional [10,15] or unidimensional [11] measurements of tumor burden over time to evaluate the tumor growth. Park et al categorized the definitions into four distinct groups: tumor growth rate ratio (TGR), tumor growth kinetics (TGK), early tumor burden increase, and combinations of these approaches [16]. It should be noted that TGR and TGK solely evaluate the variations in existing target lesions and do not incorporate the assessment of newly emerging lesion. Champiat et al considered hyperprogression disease (HPD) as at least 2-fold increase the TGR from baseline to during therapy [10].
Some authors have used the combination of clinical and radiological aspects in order to improve the definition. They have defined HP as the time interval between the initiation of ICI therapy and an unexplained discontinuation lasting no more than 2 months (TTF ≤ 2 months) [17]. Investigators suggest as a necessity an optimal definition to avoid underestimated or overestimated HPD (Table 1).
Table 1. Examples of definition to HPD.
We present a comprehensive review focusing on potential genetic predictive biomarkers of immunotherapy response across various tumor types.
Biomarker associated with progression.
A biomarker is a biological molecule found in blood, other fluids or tissues used as a sign of a normal or abnormal process, a condition or a disease. Biomarkers have many potential applications, including risk assessment, screening, prediction of response to treatment or monitoring. In the context of immunotherapy, biomarkers refer to measurable indicators that provide information about the state of a patients´s immune system or the presence specific characteristics in the tumor. Understanding which individual variations can justify the different patterns of response to ICI can improve selection of tumor types and patients. The massive development of immune checkpoint inhibitors makes it imperative to elaborate guidelines to assist clinicians in making decisions and selecting patients who can truly benefit from them or who may experience rapid disease progression.
This review summarizes the evidence regarding the relationship between mutations in tumor cells and their clinical relevance as biomarkers for response to immunotherapy (Table 2).
Table 2. Alteration of tumor cells as possible biomarkers.
Possible genomic alterations. The most common changes in these alterations are activating mutations, Loss-of-function (LOF) and Gain-of-function (GOF) changes in the development, progression and response of the treatment. Activating mutations can lead to abnormal signaling pathways, uncontrolled cell growth, and contribute to the development of various disease. GOF are the results in proteins with increased activity, promoting abnormal cell growth and survival. LOF normally affect tumor suppressor genes, wich normally inhibit cell proliferation and promote apoptosis.
MDM2: Murine double minute 2; EGFR: Epidermal growth factor receptor; PTEN: Phosphatase and tensin homolog; JAK: Janus kinase1/2; SKT11/LKB1: Serine/threonine kinase family NSCLC: non-small cell lung cancer; GBM: Glioblastoma multiforme
MDM2
Murine double minute 2 (MDM2) is a proto-oncogen. MDM2 possesses a RING finger domain porssesing E3 ligasa activity and bind to p53 inactivating it and therefore, regulating apoptosis and cell-cycle [20]. Amplification and/or overexpression of MDM2 has been identified in about 4% - 7% in several cancer types. It is most frequent in patients with liposarcoma (ranging from 40% to 60%), or metastasic breast cancer (13%) [21]. MDM2 amplification has been associated with HPD following immunotherapeutic agents and it is considerer as possible resistance biomarker. However, its validation is still pending. The mechanism by which MDM2 mediates HPD remains unclear. Nevertheless, there have been cases of occasional responses to immunotherapy in patients with liposarcoma and MDM2 amplification. This observation implies that the resistance mechanism coexists with other molecular alterations [22]. Diverse pathways, such as those related to tyrosine kinase, PI3K signaling, TP53 and MAPK signaling co-alterations were potentially targeteable alterations. The optimization of immunotherapy in combination with targeted therapy against MDM2 could contribute to enhancing resistance of ICI [20]. It is important to note that this specific pattern of disease progression does not uniformly impact all patients with MDM2 alteration [16].
MDM2 amplification could potentially be associated with accelerated disease progression in patient receiving PD-1 and PDL-1 inhibitors [17,23]. Watson et al reported a case of hyperprogression after administering anti-PDL-1 (pembrolizumab) treatment in a patient with Epstein-Barr virus-associated gastric adenocarcinoma. The Epstein-Barr virus-related subtype typically shows a favourable response to immune checkpoint inhibitors (ICI). However, the lack of response observed in this case suggests a potential resistance to immunotherapy, possibly mediated by the presence of ERBB2 amplification and in a lesser extent, MDM2 amplification. This unusual tumor profile may have contributed to the lack of response to pembrolizumab [24]. Rayburn et al studied the expression of this oncogen and concluded that patients who presented MDM2 amplification tended to develop distant metastasis and were less prone to responding to treatment [25].
The role of MDM2 in resistance to ICI requires investigation. Currently, the presence of this alteration should not be a reason to avoid immunotherapy [19]. However, in patients with MDM2 amplification, it may be advisable to consider early radiological monitoring to rule out hyperprogressive disease.
EGFR mutation
Epidermal growth factor receptor (EGFR) is a tyrosine kinase transmembrane receptor that activates RAS/RAF/MEK and PI3K/AKT/mTOR pathways, increasing cell proliferation and growth. EGFR activating mutations, amplifications and overexpression are found in different tumors [26-28].
Akbay et al proved that the activation of the EGFR pathway promotes overexpression of PDL-1 on the surface of cancer cells, production of cytokines and others immunosuppressive cells, such as macrophages and T regulatory cells (Tregs) to avoid the antitumor response. This immunosuppresive enviroment may explain the resistance to ICI therapy [29]. This promote the clinical investigation of targeting EGFR pathway and immune checkpoints. Chubachi et al published a case with a drastic progression after Nivolumab in EGFR mutant non-small cell lung cancer (NSCLC), previously responding to anti EGFR–TKI [30]. Based in this results, combination therapy is a field of study in this population. A comparation of the efficacy of four immunotherapy-based therapies in NSCLC patients after EGFR-TKIs failure concluded that immunotherapy in combination with chemotherapy and anti-angiogenesis are improve ORR and DCR [31]. Similar benefit was observed in the phase 1 NCT02013219 with erlotinib plus atezolizumab resulted a higher ORR [32]. Alterations in EGFR, MDM2/MDM4 and several genes located on 11q13 (CCND1, FGF3, FGF4, FGF19) are reported as possible predictive biomarkers for HPD [33]. Rapid progression in a patient with EGFR mutation and MYC amplification has been described by Huang et al [34] and ICI monotherapy in this subgroup of patients must be performed with caution. The relationship between EGFR exon 20 insertion and ICI-induced HPD is unknown. Some studies hipothesy and EGFR mutated tumor growth throught interaction with M2-like macrophages [35] and MYC amplification can contribute to tumor growth. EGFR, MDM2/4 and DNMT3a alterations remained independent predictors of poor clinical outcome [22]. The mechanism of resistance is unclear and the researchers proposed upregulation of PD-1 and PDL-1 through EGFR activation. It is important to take into account that the coexistence with other alterations can also play a role in resistance to immunotherapy in this population and the combination therapy may be an option for improvement response. The role of EGFR requires further investigation.
PTEN loss
Phosphatase and tensin homolog (PTEN) is a tumor suppressor gene with roles in the cell cycle, growth, survival, DNA repair and regulation of the Akt/mTOR pathway. Somatic alterations result in loss-of-function (LOF) in many types of tumors [36-37]. Loss of expression of PTEN increase the activation of PI3K pathway regulating several critical cellular processes [38]. PI3K/AKT/PTEN/mTOR pathway plays a role in multiple mechanism of chemo and radio resistance, that suggest targeting this pathway could be a promising strategy to restore drug sensitivity [39].
PTEN loss has been related to a poorer response to immunotherapy in patients with melanoma, as it is associated with the upregulation of vascular endothelial growth factor (VEGF) and other immunosupressive cytokines [38]. In prostate cancer PTEN loss has been described in 20% to 30% patients. This cell-specific genomic change modified the immunosuppressive microenvironment as a consequence of upregulated FoxP3+ T regulatory cells and lower CD8+ T cells [40]. It has been identified as an acquired mechanism of resistance to immunotherapy in metastatic uterine leiomyosarcoma [41]. The publication by Trujillo et al discussed acquired resistance through PTEN LOF in melanoma patients. The analysis of new brain metastases in a BRAF V600E mutant melanoma patient revealed PTEN loss, whereas no detectable PTEN alterations were observed in the pre-treatment biopsy. Additionally, a tumor biopsy conducted at the time of treatment progression demonstrated a near complete absence of CD8+ cells. These findings support the notion that PTEN loss contributes to ineffective CD8+ T-cell response and resistance to ICI [42].
These data suggest that PTEN status contributes to a dysregulated antitumor response and may help guide the selection of patients for future immunotherapy treatment in diverse tumor types.
JAK 1/2 loss
Janus kinase (JAK) is a non-receptor protein tyrosine kinase. Interferon receptors activate intracellular signaling pathways involving JAK1 and JAK2 Kinases. These kinases are implicated in the phosphorylation and activation of STAT transcription factors, triggering IFN mediated response. In the context or immunotherapy, activation of IFN signaling pathways through JAK1/2 is crucial for the anti-tumor immune response. The mutations observed in the interferon pathway may contribute to immune evasion by tumor populations in response to ICI. As it often the case with LOF mutations in JAK1/2 have been associated with resistance to therapies targeting PD-1/PDL-1 pathway in cancer treatment [43].
Zaretsky et al described an acquired resistance in two melanoma patients who initially responded to anti-PD1. The sequencing of paired biopsy (biopsy at diagnosis and at progression) showed a total loss of JAK2 protein, resulting a lack of response to interferon gamma (IFN-gamma), without change in sensitivity to interferon alfa or beta. The acquisition of mutations in JAK was an early event before clonal selection after treatment [44]. A recent publication suggest that patients with JAK1/JAK2 mutation did not respond to downstream signalling to IFN-gamma and not upregulate PDL-1 [45]. Other study reported an uncommon defects in IFN-gamma pathway (JAK2, IRF1, IFIT1/2/3, MTAP and miR31) detected in melanoma samples from patients who progressed to anti-CTLA-4 treatment [46]. A proof of concept publication suggested that the presence of a T-cell inflamed phenotype contained IFN-gamma genes related to antigen presentation, chemokine expression, cytotoxic activity and adaptive immune resistance. These features are crucial for clinical response to ICI. Nevertheless, there are non-responders to anti-PD1 therapy patients in this publication. The reason for lack of response is unknown, it might be a result of a coexist immunosuppressive pathways [47].
Some controversial data exist in microsatellite Instability- High (MSI-High) colorectal cancer with Beta-2 microglobulin (B2M) and JAK1/2 loss-of-function. JAK1/2 LOF patients did not show worse response to anti-PD1 therapy. B2M and JAK1/2 mutations had a lower mutational tumor burden score and occurred frequently in high microsatellite Instability patients (MSI-H). MSI-H is a phenotype characterized by a high number of genetic mutations due to defects in the DNA mismatch repair system. These mutations can affect various genes, including B2M and JAK1/2, and contribute to the development of tumors with higher microsatellite instability. In conclusion, colorectal MSI-H patients with B2M and JAK1/2 alterations should not be excluded from ICI [47]. These results are contrary to lung and melanoma tumors were JAK1/JAK2 LOF are associated with resistance to ICI. It may indicate a different molecular mechanism that needs to be further clarified.
Wnt/Beta-catenin
Beta-catenin gene (CTNNB1) is a member of the Wnt (wingless) signalling pathway. It plays an important role in tumorigenesis, cancer progression (by regulating the tumor-immune cycle), migration and division [48]. The Wnt signal is transduced through cell membrane-associated receptors from the frizzled family. This signaling pathway stabilizes beta-catenin, allowing its entry into the cell nucleus. Inside the nucleus, beta-catenin forms a complex with members of the Tcf/Lef-1 family of transciption factors. This activation initiates the transcription of various genes, among them proto-oncogenes such as CCND1 [48]. A probable mechanism of resistance to ICI is a down-regulation of Batf3-lineage dendritic cell recruitment and consequently low recruitment CD8+ T-cells. In melanoma patients an up-regulation of Wnt signalling may supress immune infiltration producing a lack of response to immunotherapy [49]. An exome sequencing and pathway analysis revealed that non-T cell inflamed melanoma tumors showed an activation of Wnt/beta-catenin pathway. Spranger et al revealed a correlation between the activation of the Wnt/beta-catenin signalling pathway and absence of a T-cell gene expression signature. For instance, novel therapeutic interventions to restore T-cell entry could remodel immunotherapy responsiveness [49]. Some proposals with target therapy against Wnt/beta-catenin signalling are expected to overcome the resistance to immunotherapy [50].
In the canonical Wnt/beta-catenin pathway, the nuclear transcription co activator protein beta-catenin is constantly degradation in the cytoplasm by a destruction complex comprised of the scaffolding protein axin (AXIN1) along casein kinase 1 (CK1), glycogen synthase Kinase 3 (GSK3) and the adenomatous polyposis coli (APC) gene product [51]. Adenomatous polyposis coli (APC) mutations are found in more than 80% of colorectal tumors and it associated in its pathogenesis. Alterations in APC generate a dysregulation of multiple cellular process leading to activation of the Wnt signalling pathway. This alteration has been associated with a more aggressive colon cancer biology with a down regulation of T-cell infiltration and not benefit from immunotherapies. Microsatellite stable (MSS) colon cancer patients typically harbouring a dysregulation of Wnt pathway with lower T-cell and they not benefit from ICI treatment [52].
Trying to categorize tumors based on the presence or absence of a T-cell–inflamed tumor microenviroment, Luke et al performed an integrative analysis of The Cancer Genome Atlas (TCGA). They identified strong associations in non-T cell inflamed microenvironment and Beta-catenin pathway activation. Most of the tumors showed a lower immune gene expression compared with normal tissue. They suspected that this biologic process was an early event in the carcinogenesis [53]. Pinyol et al observed that approximately 30% of hepatocarcinoma (HCC) patients showed a “cold” tumor enrichment in CTNNB1 mutations with an innate resistance to anti-PD1/PDL-1 treatment [54].
Wnt/beta-catenin signaling plays a crucial role in maintaining the stem cell pool and facilitating tissue and organ regeneration. Preclinical trials are currently underway to develop new targeted therapies aimed at modulating the Wnt signaling pathway. However, no drugs have been approved for clinical use in this regard. The potential toxicity of manipulating Wnt signaling in normal intestinal epithelium and its association with bone disorders have contributed to the lack of approved drugs.
Further studies are necessary to gain a deeper understanding of the specific role of Wnt signaling and its potential as a target for therapy. These studies will help determine the feasibility and safety of targeting the Wnt pathway in different disease contexts. It is essential to carefully evaluate the effects of manipulating Wnt signaling to minimize any potential adverse effects and ensure the development of effective and safe therapies.
Beta 2-microglobulin mutation
Beta 2-microglobulin (B2M) is a low-molecular-weight protein that is synthesized by various cells, including lymphocytes. B2M is closely associated with Human Leukocyte Antigen class I (HLA-I) molecules, as it is encoded by the B2M gene.
Loss of Beta 2-microglobulin can have significant implications for antigen recognition by CD8+ T-cells involved in antitumor immune responses. When B2M is lost the assembly of HLA-I complexes are compromised and are unable to properly present antigens on the surface of tumor cells. This loss of antigen presentation can lead to a reduced ability of CD8+ T-cells to recognize and target tumor cells effectively. However, there are multiple strategies or mechanism employed by cells to evade detection and destruction by CD8 T-cells. One of the most common interconnected because B2M loss is the downregulation or loss of expression of major histocompatobility complex class-I (MHC-I) molecules on their surface.
The loss of Beta 2-microglobulin has been documented in various types of cancer and is considered a potential mechanism for tumor cells to evade immune recognition. By downregulating or eliminating B2M expression, tumor cells can escape immune surveillance and avoid detection and destruction by CD8+ T-cells [55-56].
Understanding the molecular mechanism of acquired resistance to ICI, Ribas et al analysed of paired tumor samples from four patients with metastatic melanoma who had relapsed while receiving PD-1 inhibition. Patient 1 and patient 2 presented LOF mutations in the gene encoding JAK1 and JAK2. The third patient showed a frameshift deletion in exon 1 of the B2M and patient fourth not presented genetic alterations with clear potential in acquired resistance. Focus in the third patient, some of the possibilities of the lack of tumor recognition, activation or a loss of sensitivity to their effector molecules by the cancers cells are the loss of antigen-presenting machinery components. The loss of B2M results in reduced recognition for cancer cells by immune cells, leading to acquired resistance [44].
A longitudinal analysis of somatic genetic alterations in a cohort of melanoma patients during their ICI therapy detected 29.4% of B2M aberrations of patients with progressive disease. Alterations including frameshift mutations, loss of heterozygosity (LOH) overlapping B2M and abscense of tumor-specific B2M protein expression. Non-responders patients are enriched of B2M LOH, and it is associated with poorer survival [57].
In a comparison of the molecular profiles between the time of treatment initiation and disease progression in lung cancer patients, a study found that the loss of B2M was observed specifically in patients who did not respond to ICI therapy. This analysis utilized a sequential circulating tumor DNA whole-exome sequencing method. The study also identified several other aberrations related to inflammation and neoantigen recognition by immune cells at the time of disease progression in the entire patient cohort. These aberrations suggest a potential connection between the development of resistance to ICI therapy and alterations in pathways involved in immune recognition and response [58]. A recent study investigated the mechanisms of acquired resistance during treatment in lung cancer patients. The researchers reported heterozygous loss of B2M during chemotherapy and homozygous loss during ICI treatment. This defect in antigen processing resulted in acquired resistance among lung cancer patients [59].
Overall, this research highlights the importance of molecular profiling in understanding the mechanisms underlying treatment response and resistance in lung cancer patients undergoing ICI therapy. The detection of B2M loss and other aberrations related to immune recognition provides insights into potential biomarkers and therapeutic targets that could aid in optimizing treatment strategies and improving patient outcomes.
SKT11/LKB1 and KRAS mutated
Serine/threonine kinase family (SKT) is a tumor suppressor gene that regulates cell metabolism, growth and polarity. It plays an important role in invasion and metastasis by activating adenine monophosphate-activated protein kinase (AMPK). Loss of STK11 function can disrupt cellular homeostasis and contribute to tumor development and progression. The presence of concurrent KRAS and STK11 mutations has been associated with poor prognosis and resistance to certain targeted therapies. Kirsten rat sarcoma virus (Kras) is an oncogene that encodes a small GTPase transductor protein called Kras. Mutations in Kras result in the constitutive activation of KRAS, leading to uncontrolled cell differentiation, tumor growth chemotaxis and apoptosis [60].
The presence of SKT11/LKB1 have been identified in certain types of cancer and are associated with resistance to immune checkpoint blockade [61-62]. It is present in 33% of patients with non-small cell lung cancer [63] with an increased prevalence seen in smokers and patient harbouring Kras mutations. To elucidate the biology of SKT11 mutations leading to poor clinical outcomes, a translational assessment was conducted in lung tumors. The investigation revealed that the unfavorable prognosis might be attributed to a compromised peripheral and intratumoral immune phenotype enriched with immunosuppressive cells. Similar findings were reported by Koyama et al demonstrating that genetic ablation of SKT11/LKB1 resulted in the accumulation of neutrophils with T-cell suppressive effects and a decrease in tumor-infiltrating lymphocytes (TILs). This population exhibited reduced survival, likely due to the ineffectiveness of targeting antibodies [64].
This negative biomarker is determinant of primary resistance in lung cancer patients despite the presence of high or intermediated tumor mutational burden (TMB) [62]. In approximately 30% of non-small lung tumors with an aggressive phenotype, LOF mutations in STK11 and gain-of-function (GOF) Kras mutations are observed. A retrospective real-world cohort of advanced NSCLC who received first line with ICI, chemotherapy or targeted therapies explain that SKT11 alteration confers a poor prognosis, regardless of the treatment received. Therefore, STK11 mutations represent a prognostic biomarker [65]. However, there is not clear if STK11 alterations are also a potential predictive biomarker of ICI [62]. Combination strategies of immunotherapy with chemotherapy showed a benefit impact in survival in NSCLC Kras mutated patients. Is the case of Sotorasib (Kras G12C inhibitor) in combination with atezolizumab or Pembrolizumab in Kras p.G12C-mutated NSCLC. The results demostrate a better ORR in the combination of sotorasib with Pembrolizumab but a higher incidence of grade 3-4 TRAEs in the combinations arms [66]. Nevertheless, a recent meta-analysis concluded that there was not a significant association between the efficacy if ICI and Kras status [67]. And preclinical studies have indicated that Kras-mutant lung tumors bearing Tp53 or SKT11/LKB1 comutations differ in their response to docetaxel with or without selumetinib, suggesting that comutations may also affect treatment responsiveness [68]. In summary, there is a need for improved combination therapies in patients with KRAS mutations to achieve enhanced clinical benefits.
CDKN2A
Cyclin dependent Kinase inhibitor 2A (CDKN2A) gene codifies for several proteins. These proteins act as a tumor supressor and are involved in regulating cell cycle and stopping cell division in older cells (senescence).
There is a controversy in the role of CDKN2A to response to immunotherapy treatment. Adib et al studied the association between CDKN2A LOF alterations and response to treatment. They evaluated six tumor types: esophagogastric cancer, head and neck cancer, melanoma, non-small-cell lung cancer, renal cell carcinoma and urothelial carcinoma. In their experience, the presence of CDKN2A in urothelial carcinoma was related to a shorter progression-free survival and a shorter overall survival when compared with wild type tumors. Discordant association was detected in the others cohorts of tumors [70]. A study analysed 139 non-small lung cancer samples with Next Generation Sequence (NGS) before started ICI. They evaluated the association of CDKN2A LOF with different clinical outcomes. The reported a negatively impact in survival when CDK2NA LOF was present [70]. In melanoma patients, the deletion of CDKN2A is associated with a higher occurrence of alterations such as TTN, MgUC16, LRP1B, and NF1. Studies have reported a beneficial effect of immune checkpoint inhibitors in the melanoma population with these alterations. These patterns suggests that CDKN2A alterations may serve as a positive prognostic biomarker for the response to ICI therapy in melanoma. This pattern was also seen in non-small cell lung cancer but not in glioblastoma multiforme [71]. Nevertheless, CDKN2A deletion is negatively correlated with the expression of T-cell markers and could inhibit expression of certain chemokines [72].
Further investigation is needed to discern the biology of CDKN2A alterations and their interaction with immunotherapy.
Others immune-related biomarkers.
Indeed, besides tumor cell biomarkers, there has been a growing interest in studying other emerging predictive biomarkers. These biomarkers aim to provide additional information to guide treatment decision and predict response to therapies.
Tumor microenvironment (TME) is a complex ecosystem composed of various types of cells and extracellular matrix. Changes in TME after checkpoint inhibitors could be another potential mechanism to resistance. Cancer associated fibroblasts (CAFs) play a role in tumor growth, progression and metastasis. TCGA database has been used to evaluate the prognosis utility of signature genes for CAF-subtypes and its implications in immunotherapy resistance [73]. Myeloid-derived suppressor cells (MSDCs) are other group of immunosuppressive cells. They have been implicated in tumor angiogenesis, metastasis and prognosis. A high frequency of this heterogeneous group are associated with poor outcomes in prostate and melanoma patients [74-75].
T cells play a direct role in the cancer-immunity cycle and are essential for an effective immune response against cancer. The T-cell receptor (TCR) repertoire refers to the diverse range of T-cell receptor genetic rearrangements within the adaptive immune system. A low TCR repertoire footprint, indicating a limited diversity of T-cell receptors, can be associated with a less favorable response to ICI therapies [76]. This suggests that a more diverse TCR repertoire is beneficial for recognizing a wide range of tumor antigens and mounting an effective immune response.
An increased density and localization of TILs are correlated with therapeutic response. Forty-six samples from patients with metastasic melanoma during anti-PD-1 treatment showed higher levels of CD8+ T-cells within the responders [70]. The presence of high levels of TILs are associated with a higher PDL-1 expression (PDL1 expression is currently approved as a biomarker for treatment with ICI in NSCLC, gastric or oesophageal cancer or bladder cancer among others) [77]. Regulatory T (Treg) cells contribute to immune suppression by inhibiting response against cancer cells. In the tumor microenvironment, Tregs can infiltrate and accumulate, creating an immunosuppressive environment that dampens the anti-tumor immune response. In contrast, reducing the suppressive activity of Tregs or depleting Tregs can enhance anti-tumor immune responses and improve the efficacy of immunotherapies [78]. A recent publication suggests that changes in circulating Treg cells could predict clinical benefit to ICI. They detect that a proliferation of Treg has been associated with hyperprogression [79].
Gut microbiota has been shown to influence on anticancer immune responses. Some unfavourable changes in the microbiota have been described to cancer immunotherapy resistance. Some efforts to maintain or reprogramme intestinal bacteria are ongoing [80]. Beneficial gut bacteria play a role to maintaining intestinal barrier and homeostasis to avoid system inflammation during immunotherapy.
Ongoing and future investigations in predictive biomarkers hold great promise for improving treatment outcomes and enabling more personalized approaches to cancer therapy. By identifying biomarkers that can accurately predict treatment response, clinicians can make more informed decisions, optimize treatment selection, and ultimately improve patient outcomes.
In the present day, there are many advances aimed at detecting potential predictive biomarkers for response to immunotherapy. However, we still lack a validated biomarker. The type of mutation also seems to influence how the immune system responds to tumors. This is the reason why the same alteration sometimes has a different effect. While many of the biomarkers presented here can contributed to therapeutic decision-making, none of them are perfect, but there are useful. In light of this complexity, researchers are exploring ways to combine multiple biomarkers.
Conclusion
Cancer immunotherapy is now a pillar of cancer treatment and have brought an important improvement in patient survival. Understanding the mechanism how the immune system detects and kills cancer cells would improve the clinical application of immunotherapies through improved patient selection strategies. However, not all patients respond to these novel therapies and approximately 9% to 20% progressed during the therapy. The mechanism underlying HP or PD and other patterns of response are poorly understood. The lack of a standarized definition difficult the early detection of these patients and it is urgent multidimensional studies to better characterise unconventional responses to immunotherapy.
No definitive biomarkers have been identified to differentiate between the various response patterns to immunotherapy. The complex interplay of the tumor microenvironment, tumor cells, immune system and clinical characteristics must be integrated to select patients appropriately and avoid the risk of administering potentially harmful therapies. It is imperative to incorporate oncogenic sequencing panels into our daily practice to prioritize research on the other molecular pathways across a wide range of tumor types.
Author Contributions: LC drafted the manuscript and EC supervised the article. All authors have read and agreed to the published version of the manuscript
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable
Informed Consent Statement: Not applicable.
Data Availability Statement: Data is contained within the article.
Conflicts of Interest: The authors declare no conflict of interest.
References
1.Borghaei H, Paz-Ares L. Nivolumab versus docetaxel in advanced nonsquamous non–small-cell lung cancer. N Engl J Med. 2015;373(17):1627-1639
2.Larkin J, Chiarion-Sileni V. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373(1):23-34.
3.Motzer RJ, Escudier B. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803-1813.
4.Marcus L, Fashoyin-Aje LA. FDA approval summary: pembrolizumab for the treatment of tumor mutational burden–high solid tumors. Clin Cancer Res. 2021;27(17):4685-4689
5.Sharma P, Hu-Lieskovan S. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. 2017;168(4):707-723.
6.Hanahan D. Hallmarks of cancer: new dimensions. Cancer Discov. 2022;12(1):31-46.
7.Halima A, Vuong W, Chan TA. Next-generation sequencing: unraveling genetic mechanisms that shape cancer immunotherapy efficacy. J Clin Invest. 2020;132(12).
8.Champiat S, Dercle L. Hyperprogressive Disease Is a New Pattern of Progression in Cancer Patients Treated by Anti-PD-1/PD-L1 Therapy. Clin Cancer Res. 2017;23(8):1920-1928.
9.Wolchok JD, Chiarion-Sileni V. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. 2022;40(2):127-137
10.Champiat S, Ferrara R. Hyperprogressive disease: recognizing a novel pattern to improve patient management. Nat Rev Clin Oncol. 2018;15(12):748-762.
11.Saâda-Bouzid E, Defaucheux C. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann Oncol. 2017;28(7):1605-1611.
12.Kas B, Talbot H. Clarification of definitions of Hyperprogressive disease during immunotherapy for non–small cell lung cancer. JAMA Oncol. 2020;6(7):1039-1046.
13.Kim Y, Kim CH. Comprehensive clinical and genetic characterization of hyperprogression based on volumetry in advanced non–small cell lung cancer treated with immune checkpoint inhibitor. J Thorac Oncol. 2019;14(9):1608-1618.
14.Kim CG, Kim KH. Hyperprogressive disease during PD-1/PD-L1 blockade in patients with non-small-cell lung cancer. Ann Oncol. 2019;30(7):1104-1113.
15.Ferrara R, Mezquita L. Hyperprogressive disease in patients with advanced non–small cell lung cancer treated with PD-1/PD-L1 inhibitors or with single-agent chemotherapy. JAMA Oncol. 2018;4(11):1543-1552.
Please view attached pdf to view complete references