Diagnostic Accuracy of Preoperative MDCT Staging of Colorectal Carcinoma in Comparison to Postoperative Histopathological Staging.
Diagnostic Accuracy of Preoperative MDCT Staging of Colorectal Carcinoma in Comparison to Postoperative Histopathological Staging.
Dr. Arsh Sukhija MBBS, MD *1, Dr. Mahajan Mangal S., DNB, Professor2, Dr. Joshi Priscilla C., MD, Professor & HOD 3, Dr. Prerna Malik, MD4
*Correspondence to: Dr. Arsh Sukhija, 1260/12, Sant Nagar, Rohtak, Haryana, India 124001.
Copyright.
© 2024 Dr. Arsh Sukhija. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 February 2024
Published: 28 February 2024
DOI: https://doi.org/10.5281/zenodo.14185485
Abstract
Background: Colon and rectal carcinoma is one of the most frequently diagnosed types of cancer globally and is more prevalent in developed countries. However, in past few decades, more and more cases have been encountered in developing countries like India. MRI is considered an excellent imaging procedure for staging the disease pre-operatively, especially rectal carcinoma because of better soft tissue delineation. However, it has low sensitivity for detecting colon cancers because of bowel motion artifacts. MDCT of abdomen and pelvis is the most widely available and used modality to demonstrate the extent of the tumor growth, lymph nodes involved, and distant metastases. Therefore, CT plays a crucial role in determining the clinical stage for CRC.
Materials and Methods: A total of 34 patients with proven colorectal carcinoma on histopathology were included in the study. All the patients underwent contrast enhanced MDCT with or without oral/rectal contrast.
Results: Of 34 cases studied, 8 (23.5%) had T1-T2 staging, 16 (47.1%) had T3 staging and 10 (29.4%) had T4 staging on MDCT. Of 34 cases studied, 8 (23.5%) had T1-T2 staging, 18 (52.9%) had T3 staging and 8 (23.5%) had T4 staging on post-operative histopathology. Of 34 cases, 18 (52.9%) had nodal involvement on histopathology and 16 (47.1%) did not have nodal involvement on Histopathology. Of 18 cases with nodal involvement on histopathology, 15 (83.3%) were true positives on MDCT. Of 34 cases studied, 27 patients (79.4%) did not have any intrabdominal metastasis on CT.
Conclusion: This study concludes that MDCT has good accuracy in determining the tumor invasion beyond the muscularis propria, but a limited role in differentiating the tumors extending beyond the bowel wall and locally advanced tumors. Therefore, the use of MRI should be recommended in determining the stage of tumor whenever the resources allow and the patient is willing.
Diagnostic Accuracy of Preoperative MDCT Staging of Colorectal Carcinoma in Comparison to Postoperative Histopathological Staging.
Introduction
Colon and rectal carcinoma (CRC) is one of the most frequently diagnosed types of cancer globally. It is ranked as the fourth most commonly diagnosed cancer (after lung, breast, and prostate) in either sex, with more than 1.4 million new cases reported every year.1,2CRC is more prevalent in developed countries. However, in the past few decades, more and more cases have been encountered in developing countries like India. The high incidence is attributed to dietary and lifestyle changes, with more and more people adopting a “Western” lifestyle3. Studies have reported a low age-standardized rate for colorectal carcinoma (CRC) in India (4.1 to 6.0 per 100,000 population in men and 3.6 to 4.9 in women)4,5. However, considering the billion-plus population load of India, the absolute number of patients affected by the disease is enormous. The most common age at the initial time of diagnosis ranges from 40 to 59 years. Men are slightly more at risk. There is a transition in these trends, and the burden of CRC in young adults is rising. 4,6 The disease is locally advanced on initial presentation in these patients, and metastasis is often seen. Consequently, a high index of suspicion in young adults is imperative in promptly diagnosing and managing these tumors and for ensuring a fast rehabilitation.
Colorectal cancer usually manifests as an asymmetrical, short segment (<5 cm length of involvement) colonic wall thickening that narrows the lumen with or without external wall deformity. The local spread ranges from subtle extension into the surrounding pericolic fat to a direct mass extension in locally advanced tumors.
MRI is considered an excellent imaging procedure for staging the disease pre-operatively, especially rectal carcinoma.7 MRI better delineates the rectal wall laminar structures, making the local spread of the tumor more easily detectable. Involvement of the mesorectal fascia, adjacent organs, and sphincter complex can also be detected due to its higher soft-tissue resolution. However, it has a low sensitivity for detecting colon cancers because of bowel motion artifacts. Contrast-enhanced CT of the abdominal and pelvis is the most widely used modality to demonstrate the extent of the tumor growth, lymph nodes involved, and distant metastases.8 The treatment approach wildly controvert on the grounds of the stage of the disease before surgery can be planned. The tumors confined to the colonic wall are typically resected, but the tumors that have grown beyond the bowel wall require adjuvant pre-operative chemotherapy and radiotherapy.9,10 Therefore, CT plays a crucial role in determining the clinical stage for CRC. Staging also helps in patient counseling regarding the risk of recurrence, survival rate, and possible future morbidity or mortality.
Baseline and follow-up postoperative CT scans aid in identifying the disease recurrence, evaluating the anatomical relationships, and assessing the treatment response. 9,10
Duke staging system has been replaced to a greater extent by the American Joint Committee on Cancer (AJCC) ‘’TNM’’ system. The AJCC system classifies the magnitude of the disease based on three tumor features: tumor infiltration into the various layers of the bowel wall (stage “T”), the extent of lymph node invasion (stage “N”), and and secondary distant or surrounding visceral involvement (stage “M”)11. Studies have shown that CT has excellent sensitivity for differentiating the T1/T2 versus T3/T4 tumors (invasion beyond the muscularis propria). However, differentiation of the tumor invasion of 5 mm or more (T1–T3 vs. T3–T4) remains a challenge for CT.12,13
In the present study, we compare the diagnostic accuracy of pre-operative CT in the staging of CRC with the postoperative histopathological findings (gold standard).
Materials and Methods
Patients of any age with suspected colorectal carcinoma based on clinical symptoms, ultrasonography findings or colonoscopy findings were studied. A total of 34 patients with proven colorectal carcinoma on pre or post operative histopathology were included in the study. The mean age was 57.82 ± 12.77 years and the range was 31 – 86 years. The male to female ratio was 2.4:1.
All the patients underwent contrast enhanced MDCT using a Philips 16 slice Brilliance CT scanner and Philips 128 slice Ingenuity CT scanner at a Tertiary care hospital (Bharati Hospital) Pune, Maharashtra. The CT images of these patients were reviewed by a radiologist with 14 years' of experience.The study was conducted over a period of 24 months.
A written valid informed consent was taken from the patient or guardian. In case of a minor (less than 18 years age), written and informed consent from their parents/guardian was taken. The patient’s clinical history and other investigation findings were recorded in a case record form. Oral and rectal negative contrast was administered to the patient to perform a plain and contrast enhanced CT scan of the abdomen and pelvis. The images were evaluated to look for the spread of tumor beyond the bowel wall, nodal involvement, and metastasis to intra-abdominal organs.
Categorical variables were represented with “n” (percentage of cases) and the continuous variables were put forward as Mean and Standard deviation (SD). The statistical comparison of distribution of categorical variables between CT staging and histopathological staging was done using Chi-Square test. Cohen-kappa coefficient (k value) was used to measure statistical agreement between the two diagnostic methods. 14 The diagnostic efficacy was evaluated by generating two by two contingency tables and calculating the sensitivities, specificities, positive predictive values (PPV), negative predictive values (NPV) and accuracy by keeping post-operative histopathology as the gold standard. All results were formulated in tabular as well as graphical format to represent the statistical difference more distinctly.
The p-value of less than 0.05 was considered as statistically significant. All the hypotheses were formulated using two tailed alternatives against each null hypothesis (hypothesis of no difference). The entire data was statistically analyzed using Statistical Package for Social Sciences (SPSS ver 24.0, IBM Corporation, USA) for MS Windows.
Observations and Results
This was a prospective, analytical, hospital-based study which was conducted over a period of 24 months. Pre operative CECT of abdomen and pelvis was conducted on 34 patients proved to have a colonic malignancy. Majority of the patients presented within the age of 51 to 70 years. The mean age ± SD was 57.82 ± 12.77 years and the range was 31 – 86 years. There was a significant male dominance in the study. Of 34 cases studied, 24 (70.6%) were males and 10 (29.4%) were females. The male to female sex ratio was 2.4 to 1. The majority of the patients presented with complaints of altered bowel habits (32.3%) and abdominal pain (29.4%). Less common symptoms included PR bleed, abdominal distension, and malena.
Of 34 cases studied, 6 cases (17.6%) showed features of proximal bowel obstruction on CT. Signs of obstruction were more commonly seen in apple core and concentric types of involvement.
Each patient underwent a different operative procedure depending on the localization of the disease process. Rectum was the most commonly involved site followed by the sigmoid colon. Of 34 cases studied, 10 cases (29.4%) had rectal involvement and 8 (23.5%) had involvement of the sigmoid colon.
Focal involvement of the bowel wall was most commonly seen. 22 cases (64.7%) had focal (<5 cm) length of bowel wall involvement and 12 (35.3%) had segmental involvement (6-40 cm). The mean ± SD of length of involvement was 5.20 ± 1.92 cm and the minimum-maximum range was 2 – 10 cm.
Tumor morphology
We categorized tumor morphology into eccentric, polypoidal, circumferential and apple core types. Eccentric type was defined as involvement of less than 50% of the wall circumference without any external wall deformity. A total of 7 cases had this type of involvement on CT with 57% of them showing T1-2 disease, 28% showing T3 disease and 14 % showing T4 disease on histopathology. Two patients had polypoidal type of lesion on CT, both of them showed T1-2 disease on histopathology. Circumferential type was defined as involvement of more than 50% of the wall circumference with or without any external wall deformity. It was seen in 21 patients (61.8%) on CT and was highly associated with T3/T4 disease on histopathology (95%). Of the 21 patients with concentric type of involvement, 14 had T3 disease (66.6%), and 6 had T4 disease (28.5%) on histopathology. Apple core type was defined as circumferential wall involvement with external wall deformity causing severe luminal narrowing. 4 cases (11.8%) had apple core type of lesion on CT. 3 (75%) out of these 4 were associated with a T3/T4 disease on histopathology.
Of 4 cases with apple core type of involvement, 3 (75.0%) had features of proximal bowel obstruction on CT. Of the 21 cases with circumferential involvement, only 3 (14.3%) had features of bowel obstruction. None of the cases with eccentric or polypoidal involvement had features of obstruction.
Prevalence of obstruction was significantly associated with apple-core type of involvement in the study group (P-value<0.05) (Table 1).
Of 34 cases studied, 8 (23.5%) had T1-T2 staging, 16 (47.1%) had T3 staging and 10 (29.4%) had T4 staging on MDCT.
Of 34 cases studied, 8 (23.5%) had T1-T2 staging, 18 (52.9%) had T3 staging and 8 (23.5%) had T4 staging on post-operative histopathology (Table 2).
Of 34 cases, 18 (52.9%) had nodal involvement on histopathology and 16 (47.1%) did not have nodal involvement on Histopathology.
Primary tumor (“T” staging)
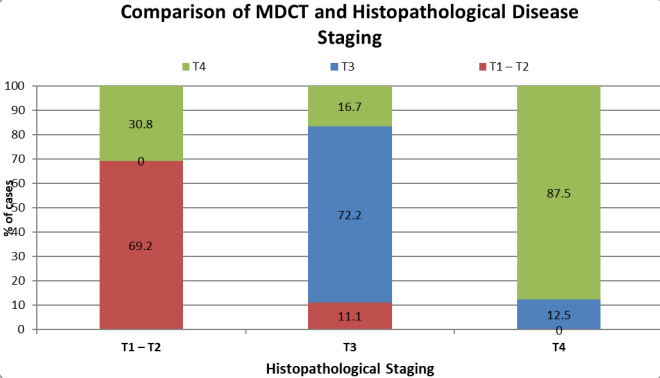
Of the 8 cases with T1-T2 staging on histopathology, 6 (75.0%) had T1-T2 staging on MDCT, 2 (25.0%) had T3 staging on MDCT. Of the 18 cases with T3 staging by histopathology, 2 (11.1%) had T1-T2 staging, 13 (72.2%) had T3 staging and 3 (16.7%) had T4 staging on MDCT. Of 8 cases with T4 staging by histopathology, MDCT correctly staged 7 cases (87.5%) and under staged in 1 case (12.5%) as T3 [Figure 1].
Distribution of staging by MDCT significantly corroborated with the staging by histopathology (P-value<0.05) with Cohen Kappa value of 0.624, which is in moderate to higher agreement limit. Therefore, it can be concluded that, there is a moderate to higher agreement between “T” staging by MDCT and histopathology in the study group (Table 3and 4).
Figure 1: Comparison of MDCT and Histopathological disease staging.
Table 3: Comparison of MDCT and Histopathological disease “T” staging.
Table 4 Diagnostic efficacy measures of MDCT against HPE for depiction of “T” staging in the study group.
Nodal involvement
Of 18 cases with nodal involvement on histopathology, 15 (83.3%) were true positives on MDCT. Of 16 cases with no nodal involvement on histopathology, 13 (81.2%) were true negatives on MDCT.
Distribution of nodal involvement on MDCT was significantly associated with nodal involvement on Histopathology (P-value<0.05) with Cohen Kappa value of 0.646, which is in moderate to higher agreement limit. Therefore, it can be concluded that there is a moderate to higher agreement between MDCT and histopathology for detecting nodal involvement (Table 5 and 6).
Table 5: Comparison of status of nodal involvement by MDCT and Histopathology in the study group.
Table 6: Diagnostic efficacy measures of MDCT against HPE for detection of nodal involvement in the study group
Please click here to view all tables and figures
Metastasis
Of 34 cases studied, 27 patients (79.4%) did not have any intrabdominal metastasis on CT. The liver was involved in all 7 patients (20.5%).
Discussion
CRC is the fourth most frequent type of cancer globally and the second most frequent cause of cancer-related fatalities. Earlier the disease was predominantly confined to developed countries. However, there is a recent rise in incidence in developing countries such as India. The major culprits are lifestyle and environmental changes, particularly the switch to a diet rich in red meats, refined grains, saturated fats, canned foods, poor intake of dietary fibers and cigarette smoking.3
Precise local staging of the tumor is critical in deciding the appropriate treatment strategies. Tumors confined to the muscularis mucosa (T1-2 tumors) without any nodal involvement are usually managed with local surgical excision. Tumors invading beyond the bowel wall (T3/T4 tumors) have shown reduced risk of recurrence when treated preoperatively with chemotherapy and / or radiation therapy. In cases of rectal cancers, tumors reaching within 1 mm of the mesorectal fascia (known as circumferential resection margin) are associated with significantly increased risk of recurrence. Including total mesorectal excision in the treatment plan is mandatory for these patients. Sphincteric complex invasion by T4 tumors may warrant abdominoperineal surgery with en bloc resection of the sphincter tissue.15
Imaging plays an important role in surveillance, establishing the diagnosis, pre-operative staging, treatment selection and post treatment follow up. MRI is the first-line imaging modality for assessing rectal carcinoma.15 It is capable of delineating the bowel wall laminar structure, therefore provides more information on the local spread of tumor, extramural extension, involvement of the mesorectal fascia or sphincter complex. 7,16. MRI, however, due to certain disadvantages such as high cost, less availability, longer acquisition times, patient discomfort and motion artifacts due to peristalsis and poor breath hold, it is less commonly performed modality, particularly in the low resource situations.
CT remains the most widely used modality for assessing colon and rectal tumors due to its easy availability and affordability. Acquiring ultrathin slices and use of multiplanar reconstruction techniques allow accurate anatomical assessment of the tumor due to exceptional spatial resolution. CT also provides critical information about the angiogenesis associated with tumor as well as the anatomical variations if present, which may otherwise lead to prolonged operative times and high risk of on table bleeding.17,18 Numerous studies have been performed to evaluate the role of CT in correctly staging the colorectal carcinoma. We conducted this study to represent the data from an Indian population.
T1-2 versus T3/T4 disease
T1 and T2 tumors (confined to submucosa and muscularis propria, respectively) are difficult to differentiate on CT because of its inability to delineate the bowel wall layers separately. Treatment wise they both are surgically resected. Surgery with adjunct chemotherapy and/or radiotherapy has shown better prognosis and reduced risk of recurrence when there is extension of tumor beyond the bowel wall. CT correctly staged T3/4 disease in 24 out of 26 cases where tumor extension beyond the bowel wall was present on post-operative pathological examination and achieved a sensitivity of 92.3% [Figure 2 and 3]. CT under staged in two patients who showed focal colonic involvement occupying < 50% of the wall circumference with absence of wall deformity, pericolic fat stranding, or nodal involvement [Figure 4]. The reason may be because of microscopic peri-colorectal fat infiltration which can be otherwise undetectable on CT. Six out of eight post-operatively proven T1-2 disease were correctly identified on CT, with a sensitivity of 75%[Figure 5]. CT over staged in two patients who showed focal circumferential involvement of the colonic wall and wall deformity with one of them showing nodal involvement [Figure 6 and 7]. The reason for this low sensitivity may be the inability of CT in differentiating the presence of benign local inflammatory or desmoplastic reaction versus extra colic tumor invasion. Therefore, caution must be taken before labelling mild pericolic fat stranding as a sign of extramural spread. Similarly, the presence or absence of nodal involvement may not be an accurate deciding factor in upstaging or downstaging a T2 or T3 tumor, respectively.
Figure 2: True positive for T3 and N positive disease.
A 65 years old female presented with PR bleed. Ultrasound done showed dilated small and large bowel loops.
Figures 2A (axial), 2B (coronal) and 2C (Sagittal) CT images in venous phase show telescoping of sigmoid colon into the rectum suggestive of intussusception (arrows). The pericolic fat appears normal, however an enhancing mass can be seen at the of the intussusception. Multiple sub centimetric lymph nodes are seen (arrowheads).
Figure 2D (magnified axial CT image in venous phase) shows cluster of nodes with perinodal stranding. One of the nodes shows heterogeneous enhancement (arrowhead).
T3, N positive disease was confirmed on post-operative histopathology.
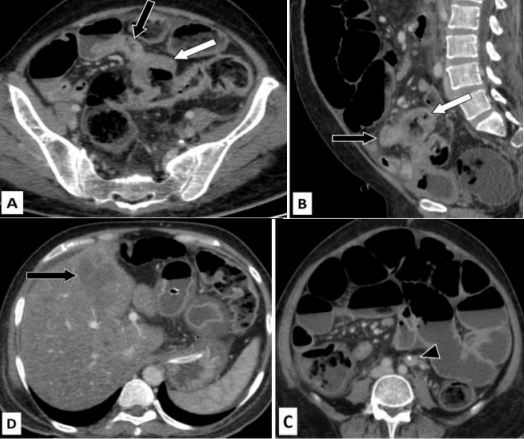
Figure 3: True positive for T4 disease and false positive for nodal involvement.
Case of 45 years old male who presented to the emergency room with pain in abdomen and distension.
Figure 3A (axial) and 3B (sagittal) CT images in venous phase show a relatively well-defined cavitating mass (white arrow) arising from the sigmoid colon. Fistulous communication with anterior ileal loops can be seen (black arrow).
Figure 3C (axial CT image in venous phase) shows multiple dilated small bowel loops with air fluid levels suggestive of obstruction. Arrowhead points to an enlarged para-aortic lymph node with calcification. Figure 3D (axial CT image in venous phase) shows diffuse fatty liver with multiple small sub centimetric hypo enhancing nodules suggestive of micrometastasis. A larger hypo enhancing lesion was seen in the left lobe(arrow). Palliative surgery was performed and the post-operative histopathology revealed T4 disease of the primary tumor. The para-aortic node was negative for malignancy.
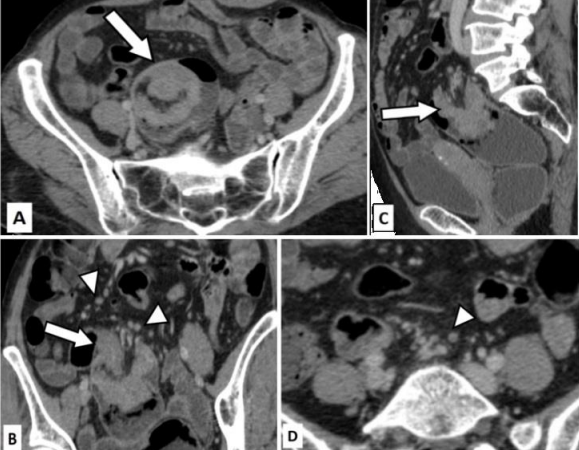
Figure 4: False negative for T4 disease and true positive for nodal negative disease (N0).
Case of 70 years old female with abdominal pain and loss of appetite. She underwent an ultrasoud which showed rectal wall thickening. Colonoscopy was done subsequently which revealed ulcerative growth in the recto-sigmoid junction. Biopsy was taken during colonoscopy which came out to be positive for malignancy (adenocarcinoma).
Figure 4A (Sagittal CT image in venous phase) shows severe apple-core type of wall thickening involving the rectum (white arrow). There is only minimal pericolic fat edema. Extramural vascular invasion is seen (black arrow). The fat planes with urinary bladder and seminal vesicles are maintained (black arrowheads)
Figure 4B (axial CT image in venous phase) shows severe apple-core type of wall thickening (arrow). Figure 4C (Coronal CT image in venous phase) shows the thickening with only minimal pericolic fat stranding (arrow). Figure 4D (Axial CT image in venous phase) shows multiple dilated small bowel loops with air-fluid levels suggestive of bowel obstruction. Minimal ascites is present (arrow).
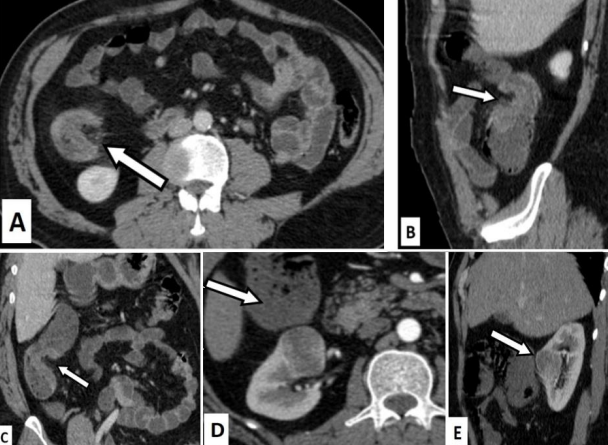
Figure 5: Example of true positive for T2 and N0 stage of the tumor.
48 years old male presented with complaints of altered bowel habits. He underwent colonoscopy which showed ulcero-proliferative caecal growth and subsequently mucosal biopsy was obtained. Histopathology showed moderately differentiated mucinous adenocarcinoma. CT was don pre operatively for staging.
Figures 5A (axial CT image), 5B(sagittal CT image) and 5C (coronal CT image) show asymmetric eccentric enhancing wall thickening involving the caecum and ascending colon (arrows) without any significant pericolic stranding. No significant nodal involvement can be seen. Figures 5D (axial arterial phase image) and E (sagittal venous phase image) show a well-defined hyper enhancing lesion in the mid pole of right kidney.
The patient underwent right hemicolectomy with partial right nephrectomy. Postoperative histopathology confirmed the presence of T2 N0 disease. The renal lesion was diagnosed as a renal oncocytoma.
Figure 6:False positive for tumor invasion beyond the bowel wall (T3/4) and true positive for nodal involvement.
Figure 6A (axial CT image in venous phase) shows severe apple-core type of wall thickening involving the recto-sigmoid junction causing severe luminal narrowing. Figure 6B (axial CT image in venous phase) show multiple subcentimetric lymph nodes with surrounding fat edema (white arrowheads) and extramural vascular congestion likely due to invasion (black arrowhead).
Figure 6C (sagittal CT image in venous phase) shows the wall thickening with pericolic stranding (white arrow) and extramural vascular invasion (black arrowhead). Post-operative histopthology showed tumor confined to the bowel wall (T2) and nodal involvement.
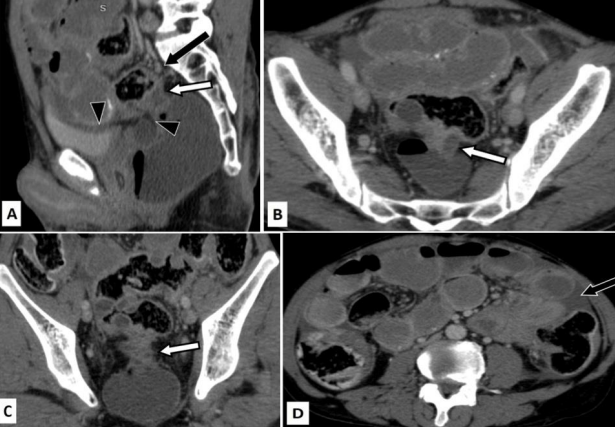
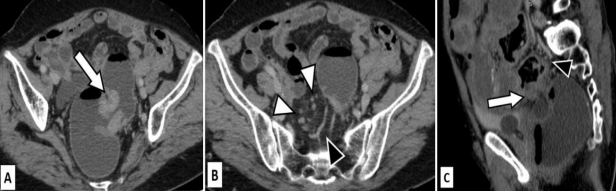
Figure 7: False positive for T4 disease and true positive for nodal involvement.
Years old male presented with abdominal pain. Ultrasound was suggestive of focal large bowel wall thickening. Colonoscopy revealed malignant growth in recto-sigmoid junction.
Figures 7A (axial CT image in venous phase) and 7B (sagittal CT image in venous phase) show concentric asymmetric wall thickening involving the sigmoid colon (white arrow) and pericolic fat stranding and extramural venous engorgement (white arrowheads). Figures 7C (sagittal CT image in venous phase) and 7D (coronal CT image in venous phase) show involvement of the pericolic fat inferior to the sigmoid colon reaching up to the superior wall of urinary bladder probably breaching the peritoneal reflection (black arrowheads). Two enlarged lymph nodes with perinodal stranding are seen in left para-aortic region (black arrows). Surgical excision of the involved segment was done. Post-operative histopathology revealed T3 tumor with nodal involvement.
T3 versus T4 disease:
Correctly identifying a T3 or T4 disease is clinically important as it may alter the treatment plan both surgically and pharmacologically. The imaging features suggestive of T4 disease included outer wall deformity, irregular spiculated or lobulated margins of the involved colonic segment, extramural vascular prominence, frank extension of similar density mass into the visceral peritoneum or adherence to the surrounding bowel loops or organs. In the study CT was able to correctly detect seven out of eight T4 disease cases with a sensitivity of 87.5% and specificity of 88.5%. Dighe et al. in 2012 used a criteria of >5 mm pericolorectal fat infiltration and extramural vascular invasion to differentiate between advanced T3/T4 disease from early T3/T2 disease19. In this study we used the combination of all previously mentioned features to stage the T4 disease.
Nodal involvement:
The ability of CT to predict nodal status is variable as compared to the previous studies. The criteria we used to assign nodes as pathological were, long axis diameter of >10 mm, irregular borders/contour with or without perinodal fat stranding, cluster of nodes, heterogeneous enhancement, necrosis and calcifications. The results showed sensitivity, specificity, PPV and NP of 83.3%, 81.2%, 84.3% and 81.2% respectively. The fluctuating sensitivity and specificity were probably due to misinterpretation of reactionary nodes as pathological.
Metastasis:
Distant organ metastasis was observed in 20.5% (7 out of 34) of the patients. The primary tumor in all of these patients was located in the rectum or sigmoid colon and liver was the site of metastasis. Two out of these seven patients presented with signs of bowel obstruction. One of these patients had fistula formation between the loop of sigmoid colon involved by the primary tumor and adjacent ileum. Surgical resection of the primary tumor was performed for these patients along with additional resection of adjacent ileal loops and mesenteric node dissection in the latter patient. CT was reported as T4 tumor without nodal involvement which was conformed on postoperative histopathology.
Two of the remaining five patients had surgically resectable liver metastasis, confined to only one lobe and three had multiple liver metastasis. The primary tumor showed no signs invasion to the surrounding organs or bowel loops in any of these patients. Therefore, neoadjuvant chemotherapy to downstage the liver lesions with surgical resection of the primary tumor were chosen as the treatment plans for these patients. There were a few limitations of the study. Firstly, the sample size of 34 patients was very small and cannot represent the data from whole of the country. Secondly, the study participants included the patients referred to a tertiary care medical Centre. Therefore, the data could be extended to the general population. Intra-observer disparities were not acknowledged in the study. Lastly, MDCT can only delineate the colonic wall layers distinctly. Therefore, T1 and T2 diseases were not evaluated separately.
Conclusion
Since past few decades, the incidence of colon and rectal carcinoma has been rising in India. The patients are presenting at a younger age and usually have locally advanced or metastatic tumor at the time of initial presentation. Therefore, timely diagnosis and accurate staging of the tumor are imperative in deciding the appropriate treatment plan for each patient to ensure speedy recovery and rehabilitation. CT is the most widely used modality in India due to its easier availability at a relatively less expense.
This study concludes that MDCT has a good accuracy in determining the tumor invasion beyond the muscularis propria, which is the major determinant of adding neoadjuvant chemotherapy to the treatment regimen. CT still has a limited role in differentiating the tumors extending beyond the bowel wall and locally advanced tumors. Additionally, CT shows variable sensitivity and specificity in detecting malignant nodes primarily due to misinterpretation of the reactionary nodes. Therefore, the use of MRI should be recommended in determining the stage of tumor whenever the resources allow and the patient is willing.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [Internet]. 2018 Nov [cited 2021 Dec 22];68(6):394–424. Available from: https://pubmed.ncbi.nlm.nih.gov/30207593/
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin [Internet]. 2021 May 1 [cited 2021 Dec 23];71(3):209–49. Available from: https://onlinelibrary.wiley.com/doi/full/10.3322/caac.21660
3. Bishehsari F, Mahdavinia M, Vacca M, Malekzadeh R, Mariani-Costantini R. Epidemiological transition of colorectal cancer in developing countries: Environmental factors, molecular pathways, and opportunities for prevention. World J Gastroenterol. 2014;20(20):6055–72.
4. Patil PS, Saklani A, Gambhire P, Mehta S, Engineer R, De’Souza A, et al. Colorectal Cancer in India: An Audit from a Tertiary Center in a Low Prevalence Area. Indian J Surg Oncol [Internet]. 2017 Dec 1 [cited 2021 Dec 22];8(4):484. Available from: /pmc/articles/PMC5705504/
5. Pathy S, Lambert R, Sauvaget C, Sankaranarayanan R. The incidence and survival rates of colorectal cancer in India remain low compared with rising rates in East Asia. Dis Colon Rectum [Internet]. 2012 [cited 2021 Dec 22];55(8):900–6. Available from: https://pubmed.ncbi.nlm.nih.gov/22810477/
6. Mathew A, Baby B, Wang K, Sirohi B, Lei F, Chen Q, et al. Colorectal cancer incidence in younger adults in India. Gut. 2020;69(10):1899–900.
7. Rastogi R, GL M, Gupta Y, Sinha P, Kumar Das P, Chaudhary M, et al. CT or MRI Which is better for Rectal Cancer Imaging? Color Cancer Open Access. 2016;2(3):2–4.
8. Horton KM, Abrams RA, Fishman EK. Spiral CT of colon cancer: imaging features and role in management. Radiographics [Internet]. 2000 [cited 2021 Dec 22];20(2):419–30. Available from: https://pubmed.ncbi.nlm.nih.gov/10715340/
9. Hong N, Park SH. CT colonography in the diagnosis and management of colorectal cancer: Emphasis on pre- and post-surgical evaluation. World J Gastroenterol [Internet]. 2014 Feb 28 [cited 2021 Dec 22];20(8):2014. Available from: /pmc/articles/PMC3934471/
10. Tan CH, Iyer R. Use of computed tomography in the management of colorectal cancer. World J Radiol [Internet]. 2010 [cited 2021 Dec 22];2(5):151. Available from: /pmc/articles/PMC2999018/
11. Weiser MR. AJCC 8th Edition: Colorectal Cancer. Ann Surg Oncol [Internet]. 2018 Jun 1 [cited 2021 Dec 22];25(6):1454–5. Available from: https://pubmed.ncbi.nlm.nih.gov/29616422/
12. AH C, RA N, HF S, W C, M K, A A, et al. Accuracy of computed tomography in nodal staging of colon cancer patients. World J Gastrointest Surg [Internet]. 2015 [cited 2021 Dec 22];7(7):116. Available from: https://pubmed.ncbi.nlm.nih.gov/26225194/
13. Nerad E, Lahaye MJ, Maas M, Nelemans P, Bakers FCH, Beets GL, et al. Diagnostic Accuracy of CT for Local Staging of Colon Cancer: A Systematic Review and Meta-Analysis. AJR Am J Roentgenol [Internet]. 2016 Nov 1 [cited 2021 Dec 22];207(5):984–95. Available from: https://pubmed.ncbi.nlm.nih.gov/27490941/
14. Sundar PSS, Richard RJ. INTRODUCTION TO BIOSTATISTICS RESEARCH AND METHODS Fifth Edition. 2012;
15. Rao SX, Zeng MS, Xu JM, Qin XY, Chen CZ, Li RC, et al. Assessment of T staging and mesorectal fascia status using high-resolution MRI in rectal cancer with rectal distention. World J Gastroenterol [Internet]. 2007 Aug 14 [cited 2021 Dec 21];13(30):4141. Available from: /pmc/articles/PMC4205321/
16. Samee A, Selvasekar CR. Current trends in staging rectal cancer. World J Gastroenterol. 2011;17(7):828–34.
17. DelGaudio JM, Swain RE, Kingdom TT, Muller S, Hudgins PA. Computed tomographic findings in patients with invasive fungal sinusitis. Arch Otolaryngol - Head Neck Surg. 2003;129(2):236–40.
18. Kijima S, Sasaki T, Nagata K, Utano K, Lefor AT, Sugimot H. Preoperative evaluation of colorectal cancer using CT colonography, MRI, and PET/CT. World J Gastroenterol. 2014;20(45):16964–75.
19. Dighe S, Swift I, Magill L, Handley K, Gray R, Quirke P, et al. Accuracy of radiological staging in identifying high-risk colon cancer patients suitable for neoadjuvant chemotherapy: A multicentre experience. Color Dis. 2012;14(4):438–44.