Comparative Study of Using Elastic Stable Intramedullary Nail (Esin) Versus Rush Pin in Prophylactic Fixation of Femur & Tibia Fractures Among Children with Osteogenesis Imperfecta Cross-Sectional Study
Comparative Study of Using Elastic Stable Intramedullary Nail (Esin) Versus Rush Pin in Prophylactic Fixation of Femur & Tibia Fractures Among Children with Osteogenesis Imperfecta Cross-Sectional Study
Mohammed Abdelmohsin Khairelseed 1*, Mustafa Alsheikh Wad-Bador 2, Mohammed Khalid Alrasheed 3
1. Buraimi Hospital, Oman
2. Omduran Teaching Hospital, Sudan
3. Khartoum University, Faculty of Medicine, Sudan
*Correspondence to: Mohammed Abdelmohsin Khairelseed, Buraimi Hospital, Oman.
Copyright
© 2023 Mohammed Abdelmohsin Khairelseed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 October 2023
Published: 30 November 2023
Abstract
Introduction: Recurrent fractures is the most challenging problem in children with Osteogenesis imperfecta, a variety of surgical methods have been investigated to decrease the incidence of this problem.
Objectives: The aim is to compare between the use of Elastic Stable Intramedullary Nail (ESIN) and Rush Pins in order to decrease fracture frequency and asses the complications associated with each method.
Methods: A descriptive cross-sectional study was conducted in 40 children with Osteogenesis imperfecta, the age of the participants was between 3 - 16 years. 20 children with OI were operated using ESIN and 20 children with OI were operated using Rush pin.
Results: Both techniques are effective in guarding against fractures and correcting the deformities. The rate of nail proximal migration was relatively higher in the ESIN group. The re-fracture rate was lower in the Rush rod group. The rate of recurrence of angular deformities were slightly higher in the ESIN group. The reoperation rate was higher in the ESIN group.
Conclusion: Corrective osteotomy with use of (ESIN) or Rush rods works well in guarding against fractures, but the overall complications and reoperation rate is statistically lower when using Rush rods, however both techniques fail to follow bone growth and have a possible complication such as nail proximal migration, recurrence of deformities and also both techniques do need repeated surgeries.
Recommendations: We recommend further studies to assess the outcome between (ESIN, Rush pin) and Telescoping rods, to assess the longevity of these implants and the precise time for exchange and to correlate between surgical interventions with the concomitant use of Bisphosphonates.
Keywords: Osteogenesis imperfecta/ non-telescoping rods/ Fracture risk reduction/ Recurrent fractures.
Comparative Study of Using Elastic Stable Intramedullary Nail (Esin) Versus Rush Pin in Prophylactic Fixation of Femur & Tibia Fractures Among Children with Osteogenesis Imperfecta Cross-Sectional Study
Introduction
Osteogenesis Imperfecta is the most common inherited form of bone fragility disorder, characterized by quantitative or qualitative defect in Collagen Type I that present in bone, skin, sclera and dentin. [1] it is characterized by osseous and non-osseous manifestations in form of decreased bone density, tendency towards fractures, poor remodeling with various limb deformities, blue sclera and dentinogenetic Imperfecta. [1]
Four classic types of Osteogenesis Imperfecta was described by Sillence on 1979 based on clinical features and disease severity. Then it was expanded into eight types on 2004, with the new techniques of molecular genetic sequencing, many new genetic mutations were discovered including the PLS3 x-linked inheritance gene, thus it is a continuum disease with a varying degree of severity due to difference in genes involved and different clinical manifestations range from severe cases with perinatal lethality to asymptomatic individuals with mild predisposition to fractures, normal stature, and normal life. [2] The generalized osteoporosis in OI patients renders these children vulnerable to frequent fractures of long bones and progressive deformities, which may have a negative impact in patient’s quality of life. [3]
Most OI patients with long bones deformities may eventually develop fractures which can lead to further progression of deformities and affect children ability to walk and quality of life.
Correction of deformities is indicated in such cases to prevent further progression and decrease incidence of refractures which may have a negative impact on patient’s life. Elastic Intramedullary Nail, K-wires, Rush rods and Telescoping rods are all Useful Options in using operative treatment, although to use which choices remains a matter of controversy. Use of Telescoping rods such as FD rods shows a promising result, but not without complications, and been expensive and currently not available in our country. In our experience, Use of Elastic Stable Intramedullary Nail and Rush rods in deformity correction in OI patients carry a good outcome.
The aim of this study was to evaluate the results of using Elastic Stable Intramedullary Nail (ESIN) in comparison to using Rush Pin system in deformity prevention of recurrent fractures among patients with OI.
Material and Methods
Study design
Descriptive Cross-sectional study.
Study area
Study was conducted in four major hospitals in Khartoum state in Sudan since these are the providing facilities of treatment of O.I patients in all country states.
Study period
The study was conducted in 300 days the period from December 2020 to September 2021. patients were operated in period between 2013 and 2020.
Study population
The study involved pediatric patients diagnosed with OI treated by osteotomy using Elastic Stable Intramedullary Nail or Rush rod fixation. The patients aged between 3 – 16 years with long bone deformities was included. Patients managed with other techniques like Telescoping and non-telescoping nails, or have secondary causes of osteoporosis (Hypophosphatasia, calcium deficiency, and long-term treatment with glucocorticoids) were excluded.
Sampling size and Technique:
Through a probability total coverage for all available patients whom fulfill the inclusion criteria which was found to be 40 patients divided into two groups.
Methods
All the patients were diagnosed with O.I based on clinical features and radiological data, according to the criteria established by Sillence.
In Group (A): Elastic Stable Intramedullary Nail (ESIN):
Corrective osteotomy or multiple osteotomies depending of Center of Rotation and Angulation (CORA) axis, single osteotomy for single site of deformity and multiple sites for multiple CORA angles, with insertion of appropriate canal size ESIN antegrade. if both femur and tibia were involved both femur and tibia were operated simultaneously, blood were prepared for the expected bleeding, full cast were applied after for 6 weeks. Patients were followed up until healing, gradual mobilization and healing, gradual patients were followed up at regular intervals all sample patients have been evaluated after complete healing of fractures.
In Group (B): Rush pain
Patients were operated either by corrective osteotomy or multiple osteotomies depending of Center of Rotation and Angulation (CORA) axis, single osteotomy for single site of deformity and multiple sites for multiple CORA angles, with insertion of appropriate canal size Rush pin inserted antegrade. if both femora and tibiae were involved both femur or tibia were operated simultaneously or in different sessions, blood was prepared for the expected bleeding, cast were applied after for 6 weeks. Patients were followed up until healing, early mobilization initiated and healing, gradual patients were followed up at regular intervals by the treating surgeon, sample patients have been evaluated after complete healing of fractures in outpatient bases.
Data Collection
A standard structured data sheet filled by authors by direct interview with the patients and parents together with x-rays and patient records. The evaluation of the outcomes was established using El Sobk et al [11] scoring system, in which a grade of excellent was given to results above 15 points, good between 11 and 15 points, fair between 6 and 10 points while grading was poor if the score was 5 points or less.
Ethical considerations
An informed consent from parents/ legal guardian for participation was obtained after explaining the objectives of the study. the data was collected for the research purpose only and the confidentiality was maintained.
Results
Forty patients with OI were included in the study, twenty patients were operated using Titanium Elastic Nail (ESIN) fixation system in lower limb segments and rest of twenty patients were operated using Rush pin fixation in femora and tibiae.
Nail proximal migration is found in 18 patients operated for femoral & tibial segments using ESIN, 9 (50) % of patients developed nail proximal migration into proximal femur (Table 1). 9 (52%) out of 17 patients operated for tibia segments developed nail proximal migration (Table 2).
Nail proximal migration is found in 8 patients operated for femoral and tibial segments using Rush pin, 3 (25) % of patients out of 12 patient developed nail proximal migration into proximal femur (Table 3). 5 (52%) out of 13 patients operated for tibia segments developed nail proximal migration (Table 4).
Recurrent fractures occurred in 45 % of patients operated using ESIN in femur (Table 5) and 42% of patient operated using ESIN in tibia (Table 6), While same complication occurred in 34% of patients operated using Rush pin in femur (Table7) and 16% of patient operated using Rush pin in tibia (Table 8)
The rate of reoperation was about 80% of patients operated using ESIN in femur (Figure 1) and 65% of patient operated using ESIN in tibia (Figure 2), While the rate of reoperation was 41% of patients operated using Rush pin in femur (Figure 3) and 23% of patient operated using Rush pin in tibia (Figure 4)
Recurrence of bowing and angular deformities occurred in 27% of patients operated using ESIN in femur (Table 9) and 35% of patient operated using ESIN in tibia (Table 10), While same complication occurred in 16% of patients operated using Rush pin in femur (Table11) and 5% of patient operated using Rush pin in tibia (Table 12).
Table No:1: Frequency of Nail proximal migration in femur in Elastic Stable Intramedullary Nail (ESIN) patients.
Table No: 2 Frequency of Nail proximal migration in tibia in Elastic Stable Intramedullary Nail (ESIN) patients
Table No:3: Frequency of Nail proximal migration in femur in Rush pin patients
Table No:4: Frequency of Nail proximal migration in tibia in Rush pin patients
Table No: 5 Frequency of recurrent-fractures in femur in Elastic Stable Intramedullary Nail (ESIN) patients.
Table No:6 : Frequency of recurrent-fractures in tibia in Elastic Stable Intramedullary Nail (ESIN) patients.
Table No: 7: Frequency of recurrent-fractures in femur in Rush pin patients.
Table No:8: Frequency of recurrent-fractures in tibia in Rush pin patients.
Figure 1: Reoperation rate in femur segments of patients operated using Elastic Stable Intramedullary Nail (ESIN).
Figure 2: Reoperation rate in tibia segments of patients operated using Elastic Stable Intramedullary
Nail (ESIN).
Figure 3: Reoperation rate in femur segments of patients operated using Rush pin.
Figure 4: Reoperation rate in tibia segments of patients operated using Rush pin.
Table No:9: Frequency of recurrence of angular deformity in femur Elastic Stable Intramedullary Nail (ESIN) patients.
Table No:10: Frequency of recurrence of angular deformity in tibia Elastic Stable Intramedullary Nail (ESIN) patients.
Table No:11: Frequency of recurrence of angular deformity in femur in patients operated using Rush pin.
Table No:12: Frequency of recurrence of angular deformity in tibia Elastic Stable Intramedullary Nail (ESIN) patients:
Discussion
A total of 40 patients were included in this study. Twenty children with OI were operated using ESIN, 50 % of them were males and 50% were females, thirteen patients of age above 7 years and seven were below 7 years. Of the 20 patients 36 femoral segments were operated and 32 tibia segments operated. The other Twenty children with OI were operated using Rush rod ,50 % of them were males and 50% were females, thirteen patients of age above 7 years and seven were below 7 years. Of the 20 patients 19 femoral segments were operated and 20 tibia segments operated. in our study revealed that the male to female ratio was 1: 1, which is identical to the ratio in the Daly et al [12] Al sobky et al [11].
Eight (45%) patients operated using ESIN in femoral segments patients showed occurrence of new fractures, and 10 (55%) patients showed no fractures after the interventions. Seven (42) % patients operated ESIN in tibia segments patients showed occurrence of new fractures and 10 (58%) patients shows no new fractures after the interventions. The current study showed slightly lower rate of re-fracture in compare to Persani et al study done in 2019[8].
There rate of re-fractures was moderately higher in age group above 7 years for femur and tibia patients with P value 0.5 and 0.6 respectively, when compared to previous author study they reported the rate of complications were higher to age group above 5 years.
Four (34%) patients operated using Rush pin in femoral segments patients showed occurrence of new fractures, and 8 (66%) patients showed no fractures after the interventions. Two (16) % patients operated using Rush pin in tibia segments showed occurrence of new fractures and 11 (84%) patients shows no new fractures after the intervention. In comparison to study published by Deepak in 2019 our study the re-fracture rate was similar in femur group and high in patients operated in tibia segments. [13]
There was no significant relationship between the age and reduction in fracture frequency post intervention in both ESIN and Rush pin groups in both femur and tibia segments, P value. 5&0.6 for ESIN and .6&0.7 for Rush pin.
Of 18 patients operated for femoral segments using ESIN , 9 (50)% of patients developed nail proximal migration into proximal femur ,9 (52%) out of 17 patients operated for tibia segments developed nail proximal migration, there were a statistical significance reduction of nail proximal migration in Femur segments with age group below 7 years compared to patients who were above 7 years of age P value .02 ..in comparison to our study , the rate of this complication is higher than had been reported by Popvok 2019 [10] in literature.
Of 12 patients operated for femoral segments using Rush Pin , 3 (40%) of patients developed nail proximal migration into proximal femur ,5 (38%) out of 13 patients operated for tibia segments developed nail proximal migration, there were a statistical significance reduction of nail proximal migration in femur segments with age group below 7 years compared to patients who were above 7 years of age P value .02 .We found that the rate of this complication reported in our study was higher than had been reported in literature by Gamal El-Adl et al 2009 [14], Joseph 2005 [15].
Of 20 children with OI operated using ESIN 5(25%) patients were recumbent,4 (20%) of patients were mobilizing with use of frames or crutches ,3 (15%) Walking without aid and 3patients (40%) Wheelchair bond. In study published by Popvoc 2019 he operated 9 patients using transphyseal flexible intramedullary nailing in pediatric osteogenesis imperfecta patients. Six from nine patients started to walk independently with a walker and/or orthotic devices at home. But two patients did not advance their walking capacity.
Of 20 children with OI operated using Rush pin ,3(15%) patients were recumbent,8 (40%) of patients were mobilizing with use of frames or crutches ,2 (10%) Walking without aid and 7patients (35%) Wheelchair bound. Deepak in 2019, they reviewed 21 children with OI, Rush rods were used in 20 femurs, for the tibiae15 children received rush rods the Seven children (33%) became household physiologic walkers, three achieved independent ambulation with orthosis, and one child with mild OI could walk unaided . The result was comparable in independent walkers. Aboulsoud 1989 used a rush pin, steinmann pin or K - wire in 10 children with 16 lower limb segments, six of the patients became totally independent of aids to ambulation.
Our study showed that total number of reoperations for ESIN group were 37 for femoral segments 102% and 25 for tibial segments 78%. In femoral segments there was no revision in 6 (33%) of cases ,4 (22%) of cases are due to deformity recurrence+ bone overgrowing Nail,4 (22%) of cases are due to bone overgrowing nail,2 (11%) of the cases due to recurrent fractures,1 (5.5%) due to recurrent fractures plus bone over growing nail and 1 (5.5%) was due to Bone overgrowing nail plus distal fracture .In tibiae segments there were no revision in 6 (35%) of the cases, 5 (29%) of reoperation were due to bone overgrowing the nail and the rest were due to several reasons including angular deformities and in one of the cases was due to infection.
Popvok 2019, studied 17 sliding flexible intramedullary nailing procedures (34 segments) in 9 children with OI he found the reoperation rate was 100% with all patients require reoperations either to bone overgrowth or various complications. our results were comparable to study done by Popvok in 2019[10].
The reoperation rate for Rush pin group were 9 (47%) for femoral segments and 6 (30%) for tibial segments a median of 38% mostly due to recurrent fracture and bony overgrowth and recurrence of deformities. we believe that our result is comparable to Al Adl et al study [66].
In our study the recurrence of deformity rate for ESIN group of patients was 4 patients 27% in femur segments and in 6 patients 35% in tibia segments, and in total 28%. In compare to our study the rate was equivalent to Pobvok study published at 2019 [10].
In our study the recurrence of deformity rate for Rush pin group of patients was 2 patients 16% in femur segments and in 1 patient in tibia segments. In compare to our study the rate was lower than what has been described by Abulsaad in 2009 [16].
Conclusion
The aim of orthopedic treatment in of children with Osteogenesis Imperfecta is to prevent deformities and fractures and correct established deformities and attempt to enhance overall patients functioning, we believe that corrective osteotomy with use of Elastic Stable intramedullary Nails (ESIN) or Rush rods works well in achieving the previous goals. The overall mobility of ESIN group shown that, 25% patients were recumbent, 20% of patients were mobilizing with use of frames or crutches ,5% Walking without aid and patients 40%Wheelchair bond. The overall mobility of Rush pin group shown that 15%patients were recumbent, 40% of patients were mobilizing with use of frames or crutches, 10%Walking without aid and 35% of patients were Wheelchair bound, the integration of surgical and rehabilitation programs is of fundamental importance. Both devices fail to follow the bone growth leaving the distal growing segment liable for deformity recurrence and future fractures. Incidence of nail proximal migration was 50% and 52% in femur &tibia respectively in ESIN group, 40% and 38% in femur &tibia respectively in Rush pin group (more common with age more than 7 years in both groups P value 0.02). Bone growth and proximal nail migration are the major factors for need of repeated surgeries. The reoperation rate was higher in ESIN group, for ESIN group was 102% and 78% for femur and tibia segments respectively, while the reoperation rate for Rush pin group was 47% and 30% for femur and tibia segments respectively.
The re-fracture rate was lower in Rush pin group in femur and tibia, for ESIN group was 45% and 42% for femur and tibia segments respectively, while the re-fracture rate for Rush pin group was 34% and 16% for femur and tibia segments respectively. The rate of recurrence of angular deformities in ESIN group were slightly higher than for Rush pin group 26% &18% respectively.
Reference
1. Tournis, S., & Dede, A. D. (2018). Osteogenesis imperfecta–a clinical update. Metabolism:80: p. 27-37.
2. Van Dijk, F. S., Pals, G., Van Rijn, R. R., Nikkels, P. G. J., & Cobben, J. M. (2010). Classification of osteogenesis imperfecta revisited. European journal of medical genetics, 53(1): p. 1-5.
3. Lutomia, M. L., & Lakati, K. C. (2011). Titanium Elastic Nails Successfully Splint Subsequent Femoral Fractures in a Child with Osteogenesis Imperfecta. Annals of African Surgery, 8.
4. Monti, E., Mottes, M., Fraschini, P., Brunelli, P., Forlino, A., Venturi, G., ... & Antoniazzi, F. (2010). Current and emerging treatments for the management of osteogenesis imperfecta. Therapeutics and clinical risk management, 6: p. 367..
5. Hsiao, C. M. S., Mormino, M. A., Esposito, P. W., & Burke, B. A. (2013). Distal humerus atrophic nonunion in a child with osteogenesis imperfecta. Journal of Pediatric Orthopaedics, 33(7): p. 725-729..
7. Cho, T. J., Lee, K., Oh, C. W., Park, M. S., Yoo, W. J., & Choi, I. H. (2015). Locking plate placement with unicortical screw fixation adjunctive to intramedullary rodding in long bones of patients with osteogenesis imperfecta. JBJS, 97(9): p. 733-737..
8. Persiani, P., Martini, L., Ranaldi, F. M., Zambrano, A., Celli, M., Celli, L., ... & Villani, C. (2019). Elastic intramedullary nailing of the femur fracture in patients affected by osteogenesis imperfecta type 3: indications, limits and pitfalls. Injury, 50: p. S52-S56.
9. Scollan, J. P., Jauregui, J. J., Jacobsen, C. M., & Abzug, J. M. (2017). The outcomes of nonelongating intramedullary fixation of the lower extremity for pediatric osteogenesis imperfecta patients: a meta-analysis. Journal of Pediatric Orthopaedics, 37(5): p. e313-e316.
10. Popkov, D., Popkov, A., & Mingazov, E. (2019). Use of sliding transphyseal flexible intramedullary nailing in pediatric osteogenesis imperfecta patients. Acta Orthop. Belg, 85(1): p. 1-11.
11. El Sobky, M. A., Hanna, A. A. Z., Basha, N. E., Tarraf, Y. N., & Said, M. H. (2006). Surgery versus surgery plus pamidronate in the management of osteogenesis imperfecta patients: a comparative study. Journal of Pediatric Orthopaedics B, 15(3): p. 222-228.
12. Daly, K. A. R. E. N., Wisbeach, A. L. I. S. O. N., Sanpera Jr, I. G. N. A. T. I. U. S., & Fixsen, J. A. (1996). The prognosis for walking in osteogenesis imperfecta. The Journal of Bone and Joint Surgery. British volume, 78(3): p. 477-480.
13. Bhaskar, A. R., & Khurana, D. (2019). Results of rodding and impact on ambulation and refracture in osteogenesis imperfecta: study of 21 children. Indian Journal of Orthopaedics, 53(4): p. 554-559.
14. El-Adl, G., Khalil, M. A., Enan, A., Mostafa, M. F., & El-Lakkany, M. R. (2009). Telescoping versus non-telescoping rods in the treatment of osteogenesis imperfecta. Acta Orthopædica Belgica, 75(2): p. 200.
15. Joseph, B., Rebello, G., & Kant, B. C. (2005). The choice of intramedullary devices for the femur and the tibia in osteogenesis imperfecta. Journal of Pediatric Orthopaedics B, 14(5):p. 311-319.
16. Abulsaad, M., & Abdelrahman, A. (2009). Modified Sofield-Millar operation: less invasive surgery of lower limbs in osteogenesis imperfecta. International orthopaedics, 33(2): p. 527-32.
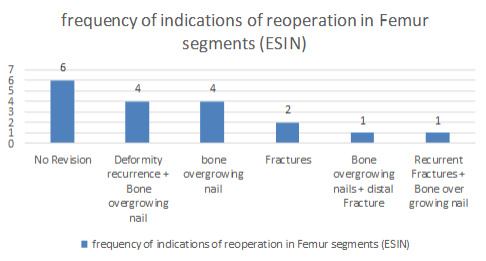
Figure 1
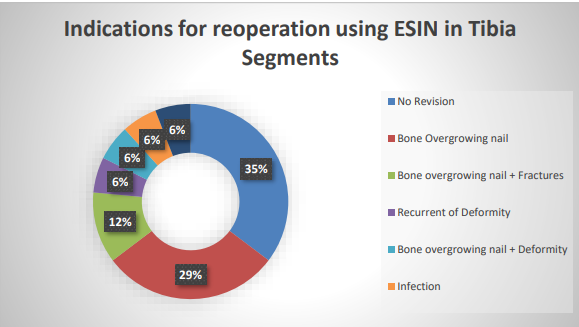
Figure 2
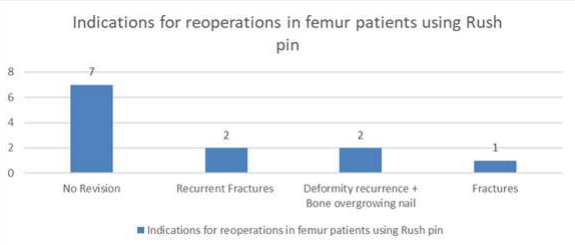
Figure 3
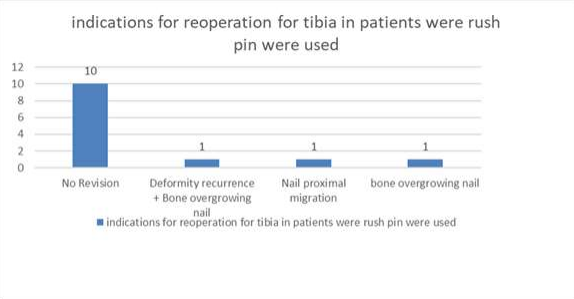
Figure 4