Early Result in Treatment of Osteoarthritis by Adipose Tissue-Derived Mesenchymal Stem Cells
Early Result in Treatment of Osteoarthritis by Adipose Tissue-Derived Mesenchymal Stem Cells
Mohammed Elfatih Elbadri *1, Ahmed Awadelbary 2, Tariq Mohammed 3, Alwya Elamien 4
1.Assistant Professor of Orthopaedics and Regenerative Medicine, National University-Sudan
2.Consultant of Orthopaedic Surgery and Regenerative Medicines, Abubakr Alrazi Hospital
3.Registrar of internal medicine, Sudan Medical Specialization Board.
4.Lecturer of radiological science and medical imaging, National University-Sudan.
*Correspondence to: Mohammed Elfatih Elbadri. Assistant Professor of Orthopaedics and Regenerative Medicine, National University-Sudan.
Copyright
© 2024 Mohammed Elfatih Elbadri. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 February 2024
Published: 01 March 2024
DOI: https://doi.org/10.5281/zenodo.10727384
Early Result in Treatment of Osteoarthritis by Adipose Tissue-Derived Mesenchymal Stem Cells
Introduction
Osteoarthritis is an irreversible, progressive degeneration of a synovial joint (Table 1) that greatly affects the affected individuals' daily performance and quality of life. Knee osteoarthritis (KOA) is by far the most common type of arthritis diagnosed, with a rising prevalence due to an increase in the average lifespan and the obesity rate in the general population. (1)
Management of KOA depends on the severity of the disease and aims to reduce pain and improve the physical functionality of the affected knees. Lifestyle modifications and conservative treatments like non-steroidal anti-inflammatory drugs (NSAIDs) and intra-articular injections using corticosteroid (CS) or hyaluronic acid (HA) are commonly used in managing mild KOA.
However, these oral medications and intra-articular injections provide temporary pain relief only and often require frequent administrations for symptomatic control. They are not beneficial in severe cases. Neither CS nor HA therapy can reverse the preexisting damage in the affected synovial joints. Their corresponding potential adverse effects include muscle atrophy, cartilage damage, and toxicity (2), which may cause more harm than benefit for the patient. Ultimately, patients may require invasive procedures such as total knee arthroplasty (TKA). Unfortunately, not all patients are eligible candidates for surgeries, like patients who cannot tolerate general anesthesia or prolonged surgical procedures or with certain underlying medical conditions.
The rise of regenerative medicine may provide promising treatment options for KOA patients. By far, the most promising alternatives are platelet-rich plasma (PRP) and mesenchymal stem cell (MSCs) injections in terms of pain alleviation, restoration of functional capacity (3), as well as potential tissue repairment (4). This literature review will evaluate the efficacy and safety of PRP and MSCs injections in KOA. We also aim to explore which population group will benefit from these treatment options.
This paper aims to present a case report of a patient who underwent stem cell therapy for treating knee Osteonecrosis.
Material and Methods
A prospective randomized controlled clinical trial was carried out on 60 knees of 30 patients (mean age 34 years, 18-71) who presented bilateral knee osteonecrosis about different severe medical conditions.
The rationale for using cytotherapy in osteonecrosis and techniques for implantation of osteogenic progenitor cells (autologous or allogenic), was evaluated and began in Sudan.
The operation was done in Alrazi Hospital, Khartoum, Sudan. We use adipose-derived MSCs (AMSCs). Adipose Tissue-Derived Mesenchymal Stem Cells were isolated and harvested from the tissue. Finally, the stem cells are injected into the injured area. The process can take up to an hour.
Literature Review:
Mesenchymal stem cells (MSCs) one frequently used subsets. They are widely distributed in various tissues, such as bone marrow, peripheral blood, fat, umbilical cord, etc. Therefore, depending on the source of the tissue, MSCs are named bone marrow-derived MSCs (BMSCs), adipose-derived MSCs (AMSCs), peripheral blood-derived MSCs (PBMSCs), and umbilical cord-derived mesenchymal stem cells (UCMSCs). (5)
In recent years, IA injection of adipose-derived MSCs in knee OA showed clinical, radiological, arthroscopic, and histological evidence at a 6-month follow-up. (6)
Among other studies, the IA injection of these stem cells (isolated from abdominal subcutaneous fat tissue) in severe knee OA reported that the low- and medium-dose groups' clinical outcomes (pain, function knee, return to sport) tended to deteriorate after one year. In comparison, those of the high-dose group tended to plateau after one year, until two years. (7)
Spasovski et al. (2018) have demonstrated that adipose-derived MSCs from subcutaneous fat in knee OA improves clinical symptoms and reduces pain at three months, obtaining the best results at six months. (8)
Clinical presentation:
60 knees of 30 patients (mean age 34 years, 18-71), pre-operative outcomes, morbidity, complications, and safety of the two procedures were compared to postoperative clinical outcomes.
At the most recent follow-up (average of 6 months), clinical outcomes of the patient (Knee Society score) were obtained along with radiological imaging outcomes (MRIs for knees with subchondral bone marrow injection).
Pre-operative assessment:
Pain on both the left and right knee was experienced by all patients, with a mean of 4.46 years of pain. The pain on the severity scale was moderate to severe (the mean for all patients is 7 for both knees).
30% of patients suffered from front knee pain on both, 30% suffered from outer side knee pain, while others suffered from inner side pain on both knees. Some patients felt achy-like pain on both knees (30%), 25% felt stabbing-like pain, while others felt a baseline dullness and achiness with episodes of sharp pain. Most patients stated that their pain radiated from knee to hip or down the back of the leg to knee with mild swelling (50%) and moderate swelling (50%).
Most patients stated that their pain was aggravated by ascending stairs, descending stairs, walking, in/out of a car, bending the knee, going from sitting to standing and sitting for long periods in both knees.
Most patients tried weight loss and NSAIDs to improve their knee pain.
Most of the patients experienced moderate pain at rest for both knees.
Three months Postoperative assessment:
The symptoms improved after the operation.
The pain on the severity scale was mild (60% of patients, 0 to 3 on the pain scale) and no pain (40% of patients, 0 on the pain scale).
Most patients stated that their pain, radiation, andswelling had disappeared.
Most of the patients stopped using NSAIDs to improve their knee pain.
Most patients experienced mild pain at rest in both knees.
Six months postoperative assessment:
The symptoms improved after the operation.
The pain on the severity scale was mild (60% of patients, 0 to 3 on the pain scale) and no pain (40% of patients, 0 on the pain scale).
Most patients stated that their pain, radiation, and swelling disappeared.
Most of the patients stopped using NSAIDs to improve their knee pain.
Most patients experienced mild pain at rest in both knees. Most patients stated that their pain didn't aggravate by ascending stairs, descending stairs, walking, in/out of a car, bending the knee, going from sitting to standing and sitting for long periods in both knees.
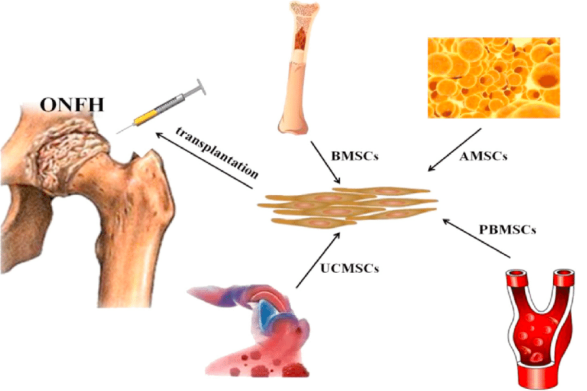
Figure 1: The main source of stem cells for transplantation. ONFH: osteonecrosis of the femoral head. BMSCs: bone marrow-derived mesenchymal stem cells; AMSCs: adipose-derived mesenchymal stem cells; PBMSCs: peripheral blood-derived mesenchymal stem cells; UCMSCs: umbilical cord-derived mesenchymal stem cells.
Discussion
Our results improved clinical outcomes, which, in parallel to other studies in this field. One study concluded that PRP treatment is more effective in pain reduction at six months and 12 months than HA use (p=0.02) (9). One study showed that using a large volume (8 mL) of pure PRP compared to a small volume (3-5.5 mL) in one single injection generated a significant clinical improvement with a response rate of 80% up to six months post-injection (10). A study indicated that triple administrations of PRP at monthly intervals yielded a more satisfactory effect in pain control based on visual analog scale (VAS) and WOMAC pain scores than a single application (p=0.0007) (11).
Conclusion
Positive outcomes include reduced pain, improved function and motion, delayed progression, reduced inflammation, and repair of damaged tissue, and may even help prevent knee replacement surgery.
Reference
1. Aho OM, Finnilä M, Thevenot J, Saarakkala S, Lehenkari P: Subchondral bone histology and grading in osteoarthritis. PLoS One. 2017, 12:0173726. 10.1371/journal.pone.0173726
2. Wernecke C, Braun HJ, Dragoo JL: The effect of intra-articular corticosteroids on articular cartilage: a systematic review. Orthop J Sports Med. 2015, 3:2325967115581163. 10.1177/2325967115581163
3. Guillibert C, Charpin C, Raffray M, et al.: Single injection of the high volume of autologous pure PRP significantly improves knee osteoarthritis: a prospective routine care study. Int J Mol Sci. 2019, 20:1327. 10.3390/ijms20061327
4. Lu L, Dai C, Zhang Z, et al.: Treatment of knee osteoarthritis with intra-articular injection of autologous adipose-derived mesenchymal progenitor cells: a prospective, randomized, double-blind, active-controlled, phase IIb clinical trial. Stem Cell Res Ther. 2019, 10:143. 10.1186/s13287-019-1248-3
5. Afizah H, Hui JH. Mesenchymal stem cell therapy for osteoarthritis. J Clin Orthop Trauma 2016;7:177e82.
6. Jo, C.H.; Lee, Y.G.; Shin, W.H.; Kim, H.; Chai, J.W.; Jeong, E.C.; Kim, J.E.; Shim, H.; Shin, J.S.; Shin, I.S.; et al. Intra-articular injection of mesenchymal stem cells for treating osteoarthritis of the knee: A proof-of-concept clinical trial. Stem Cells 2014, 32, 1254–1266.
7. Jo, C.H.; Chai, J.W.; Jeong, E.C.; Oh, S.; Shin, J.S.; Shim, H.; Yoon, K.S. Intra-articular Injection of Mesenchymal Stem Cells for the Treatment of Osteoarthritis of the Knee: A 2-Year Follow-up Study. Am. J. Sports Med. 2017, 45, 2774–2783.
8. Spasovski, D.; Spasovski, V.; Bascarevic, Z.; Stojiljkovic, M.; Vreca, M.; Andelkovic, M.; Pavlovic, S. Intra-articular injection of autologous adipose-derived mesenchymal stem cells in the treatment of knee osteoarthritis. J. Gene Med. 2018, 20, e3002.
9. Emérito Carlos Rodríguez-Merchán, Intra-Articular Platelet-Rich Plasma Injections in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Degree of Efficacy, Int J Mol Sci. 2022 Feb; 23(3): 1301.
10. Caroline Guillibert, Caroline Charpin, Marie Raffray, Annie Benmenni, Francois-Xavier Dehaut, Georges El Ghobeira, Roch Giorgi,4 Jeremy Magalon, and Denis Arniaud, Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study, Int J Mol Sci. 2019 Mar; 20(6): 1327.
11. Ip HL, Nath DK, Sawleh SH, Kabir MH, Jahan N. Regenerative Medicine for Knee Osteoarthritis - The Efficacy and Safety of Intra-Articular Platelet-Rich Plasma and Mesenchymal Stem Cells Injections: A Literature Review. Cureus. 2020;12(9):e10575. Published 2020 Sep 21. doi:10.7759/cureus.10575.