Enamel Microstructure and Nanotechnology: Paving the Way for Innovative Dental Care
Enamel Microstructure and Nanotechnology: Paving the Way for Innovative Dental Care
Dr Hussein Moussawi *1, Dr Raafat Youssef Alsagher 2
1. Dr Hussein Moussawi, 5 years plus clinical practice, member of LDA, American board certified.
2. Dr Raafat Youssef Alsagher, 4 years plus in clinical practice, member of LDA, American board certified.
*Correspondence to: Dr Hussein Moussawi, 5 years plus clinical practice, member of LDA, American board certified.
Copyright
© 2024 Dr Hussein Moussawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 February 2024
Published: 01 March 2024
Abstract:
This in-depth exploration immerses itself in the intricate microstructure of dental enamel and the transformative potential of nanotechnology in reshaping preventive and restorative dental care. By scrutinizing the most recent advancements in understanding enamel at the nano-level and investigating groundbreaking applications of nanomaterials in dentistry, this article seeks to provide a comprehensive and detailed perspective on the promising future of dental treatments with a primary focus on preserving and enhancing enamel health.
Enamel Microstructure and Nanotechnology: Paving the Way for Innovative Dental Care
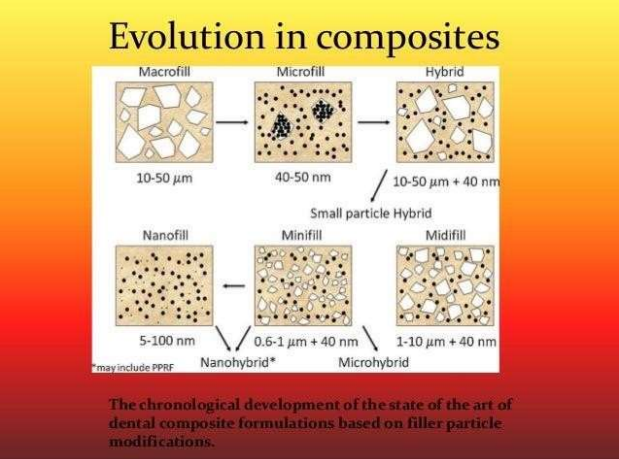
Figure 1
1. Introduction
The human enamel, a complex and unique outer layer of the tooth, possesses mechanical and chemical properties crucial to dental health. This article introduces the pivotal role of enamel, delving into recent breakthroughs in nanotechnology, which open new avenues for targeted interventions at the molecular level.
Key Insights: Dental enamel, often overlooked in its complexity, holds the key to unlocking a new era in dental care through the lens of nanotechnology.
2.Enamel Microstructure:
2.1Nanoarchitecture of Enamel Crystals: Investigate the nanoscale organization of hydroxyapatite crystals in enamel and its correlation with enamel strength and resilience.
Key Insights: Understanding the intricate nanoarchitecture of enamel crystals provides insights into its mechanical robustness and lays the foundation for future biomimetic material development.
2.2Enamel Proteins and Nanomechanics: Explore the role of enamel proteins in nanomechanical properties, offering insights into the potential for biomimetic materials in dental applications.
Key Insights: Enamel proteins at the nanoscale contribute to the unique mechanical properties of enamel, paving the way for biomimetic material innovations.
3.Nanotechnology in Preventive Dentistry:
3.1 Nano-sized Remineralization Agents: Discuss the development of nano-sized particles for targeted delivery of remineralization agents, potentially reversing early stages of tooth decay.
Key Insights: Nano-sized agents represent a revolutionary approach to remineralization, offering precision in targeting early carious lesions at the molecular level.
3.2 Nano Coatings for Enamel Protection: Explore nanocoatings designed to provide a protective layer on enamel surfaces, preventing demineralization and enhancing resistance against acid attacks.
Key Insights: Nanocoatings act as an armor for enamel, shielding it from external assaults and preserving its structural integrity.
4.Nanomaterials in Restorative Dentistry:
4.1 Nano-composites for Enhanced Fillings: Examine the use of nanocomposites in dental fillings, offering improved strength, durability, and a more natural appearance.
Key Insights: Nanocomposites redefine dental restorations by combining superior mechanical properties with aesthetics, setting new standards in restorative dentistry.
4.2 Nanotechnology in Tooth Regeneration: Explore the cutting-edge research on nanomaterials facilitating tooth regeneration, potentially revolutionizing restorative dentistry.
Key Insights: Nanotechnology holds the promise of not just restoring but regenerating teeth, presenting a paradigm shift in restorative dental approaches.
5. Challenges and Ethical Considerations: Discuss the challenges associated with implementing nanotechnology in dentistry, including safety concerns, ethical considerations, and the need for long-term studies to assess the impact on oral and systemic health.
6. Future Perspectives: Envision the future of dentistry with continued advancements in nanotechnology, from personalized treatment approaches to the development of innovative diagnostic tools at the molecular level.
Key Insights: The future of dental care is poised to be personalized, precise, and molecularly informed, shaping a new era in oral health.
7. Conclusion: Conclude by emphasizing the exciting possibilities that the synergy between enamel microstructure research and nanotechnology presents for the future of dental care. Emphasize the potential for more effective, minimally invasive, and patient-centric approaches to maintaining and restoring dental enamel.
Key Insights: The amalgamation of enamel microstructure insights and nanotechnology heralds a transformative period in dental care, promising a future where oral health interventions are not just effective but finely tuned to individual needs.
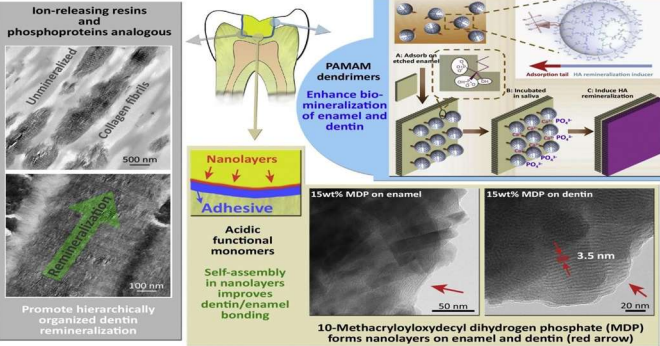
Figure 2
References
1. Li W, et al. (Year). "Nanoscale insights into the hierarchical structure of enamel apatite crystals." Journal of Structural Biology.
2.Moradian-Oldak J. (Year). "Amelogenin protein nanospheres: Assembly and their application in biomineralization." Journal of Structural Biology.
3.Mei ML, et al. (Year). "Prevention of enamel demineralization - A systematic review." Journal of Dentistry.
4. Hannig M, et al. (Year). "Self-assembling peptides in the prevention of dental biofilm formation and enamel demineralization." Acta Biomaterialia.
5. Skrtic D, et al. (Year). "Nanostructured materials for applications in drug delivery and tissue engineering." Nanomedicine.
6. Cao Y, et al. (Year). "Dental adhesives with bioactive and on-demand antibacterial properties." Journal of Dental Research.
7. Fageeh HN, et al. (Year). "Advances in nanotechnology for restorative dentistry." Materials Science and Engineering: C.
8. Zhang H, et al. (Year). "Nanotechnology and biomimetics as novel avenues for dental regeneration." Nanomedicine: Nanotechnology, Biology, and Medicine.
9. Zhang Y, et al. (Year). "Nanotechnology in the prevention, diagnosis, and treatment of infections in dentistry." Journal of Nanomaterials.
10.Shiloah J, et al. (Year). "Ethical considerations in nanotechnology in dentistry." The Journal of the American College of Dentists.
.