Iridocorneal Endothelial Syndrome with Secondary Angle Closure Glaucoma in a Male Patient
Iridocorneal Endothelial Syndrome with Secondary Angle Closure Glaucoma in a Male Patient
Ino Paul R. Villacastin, M.D 1, Ivo John S. Dualan, M.D 2, Maria Margarita Lat-Luna, M.D 3,
Perfecto Elpidio Octavio R. Cagampang III, M.D. *4
*Correspondence to: Ino Paul R. Villacastin, M.D.
Copyright
© 2024 Ino Paul R. Villacastin, M.D. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 October 2023
Published: 01 March 2024
Abstract
This case report presents a case of iridocorneal endothelial (ICE) syndrome with secondary angle closure in a male patient in a tertiary hospital in Manila. As ICE syndrome occurs more in females, this is an unusual case providing an opportunity to highlight the management of this rare disease.
Iridocorneal Endothelial Syndrome with Secondary Angle Closure Glaucoma in a Male Patient
Introduction
Iridocorneal endothelial (ICE) syndrome refers to a collection of conditions characterized by aberrant corneal endothelial cells which behave like epithelial cells in terms of proliferation, migration, and failure to demonstrate contact inhibition [1]. This syndrome usually affects one eye and is frequently seen in young females even without a family history [2]. The etiology of ICE remains unclear and can increase the risk of glaucoma.
The clinical manifestations of ICE are high intraocular pressures, reduced vision from corneal edema, unusual iris appearances, or subsequent angle closure glaucoma. Other findings include “battered bronze” appearance of the corneal endothelium and high peripheral anterior synechiae on gonioscopy. Three clinical subtypes have been identified: Chandler syndrome, essential iris atrophy, and Cogan-Reese syndrome. Among these, Chandler syndrome is the most common variant.
Case
A 37 -old-male came in for blurring of vision in the left eye at the outpatient general clinic of the Philippine General Hospital Sentro Oftalmologico Jose Rizal. The patient has a 4-month history of blurring of vision on his left eye which was described as “foggy.” He experienced rare episodes of mild eye redness but no floaters, flashes, photophobia, glares, eye pain, pruritus and secretions. He was managed at a local clinic as a case of Glaucoma with pilocarpine, Cosopt (Dorzolamide + Timolol) and Lumigan (Brimatoprost). Although medications provided temporary relief, persistence of symptoms led to consult at our clinic.
Patient’s visual acuity on lit ETDRS was SC 20/20 for the right eye and SC 20/58 improving to 20/46 on pinhole for the left eye. The left pupil was nonreactive to light and corectopic. The right eye showed Grade 3 reverse RAPD. Extraocular muscle testing was normal.
On gonioscopy, the ciliary body band of the right eye was seen in the superior and inferior quadrants and scleral spur on primary gaze opening to the cillary body band on the nasal and temporal quadrant. In the left eye, all quadrants were closed with note of peripheral anterior synechiae. On slit lamp examination, the right eye was unremarkable, while there were iris nodules superiorly and iris atrophy inferiorly for the left eye. On applanation tonometry, the right eye had an IOP of 11 mmHg. The IOP in the left eye was 41 mmHg and improved to 30 mmHg after 1 drop of brimonidine + timolol (Combigan) and a tablet of acetazolamide 250mg tablet. On indirect ophthalmoscopy, the right eye was unremarkable, while the left eye had a yellow orange disc and a cup to disc ratio of 0.9. Disc photos (Figure 1), optical coherence test (OCT) of the optic nerves (Figure 2), and automated visual field perimetry (Figure 3) showed structural and functional evidence for advanced glaucoma. The patient’s refraction was also noted to be plano for the right eye and -1.00D sph for the left eye. The patient was diagnosed with iridocorneal endothelium syndrome of the left eye, to consider Cogan-Reese syndrome, and was then referred to both the Glaucoma and External Disease services.
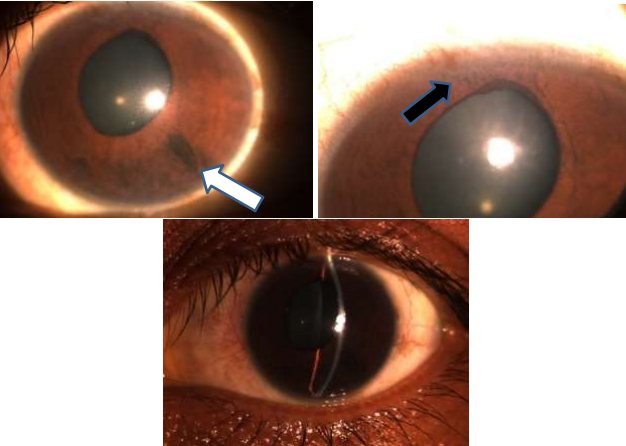
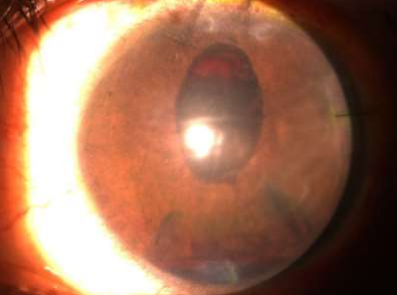
Figure 1. Slit lamp photos of the patient’s left eye. The slit lamp photos highlight the correctopic pupil of the left eye and the noted iris nodules superiorly (black arrow) and iris atrophy inferiorly (white arrow).
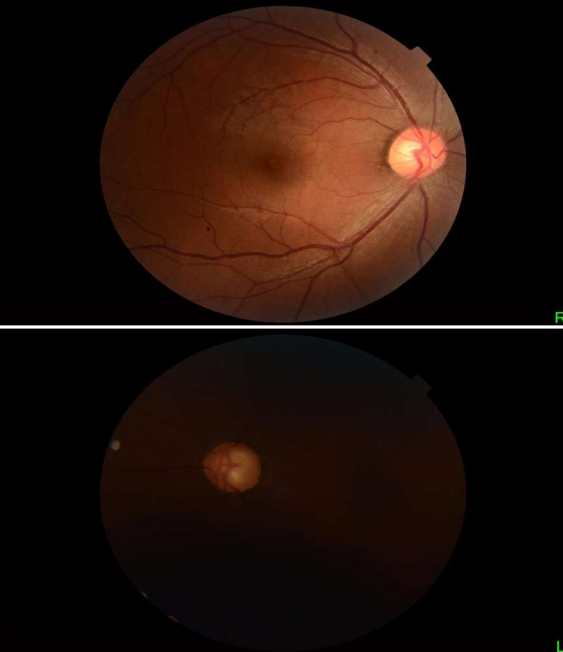
Figure 2. Disc photos of both eyes. Above: Disc photo of the right eye shows clear media, an average-sized pink orange disc with distinct disc borders, vertical CDR 0.4 and horizontal CDR 0.3, difficult to assess for PPA and RNFL reflex, follows the ISNT rule, good RNFL reflex, no disc hemorrhages. Below: Disc photo of the left eye shows hazy media, an average-sized slightly pale disc with distinct disc borders, vertical CDR 0.9 and horizontal CDR 0.9, difficult to assess for PPA and RNFL reflex, I=S=N=T or generalized rim thinning, Difficult to assess RNFL reflex, No disc hemorrhages
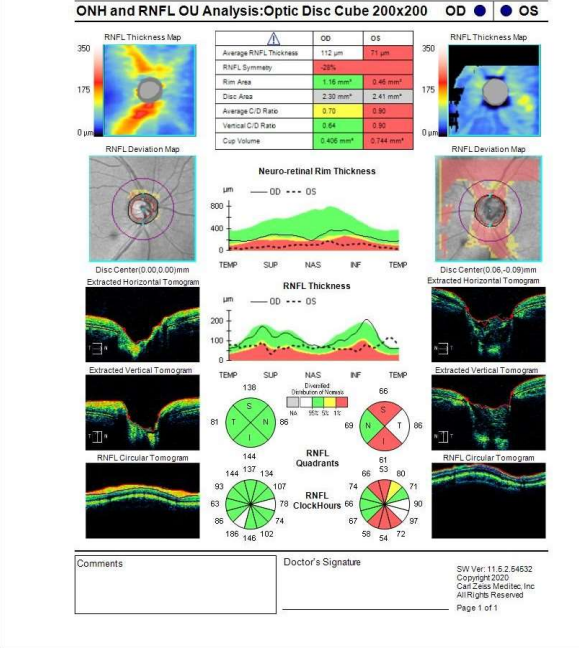
Figure 3. Optical coherence test (OCT) of the optic nerve. The patient’s OCT (done using Zeiss Cirrus 3000) showed severe thinning of the superior and inferior retinal nerve fiber layer of the left eye.
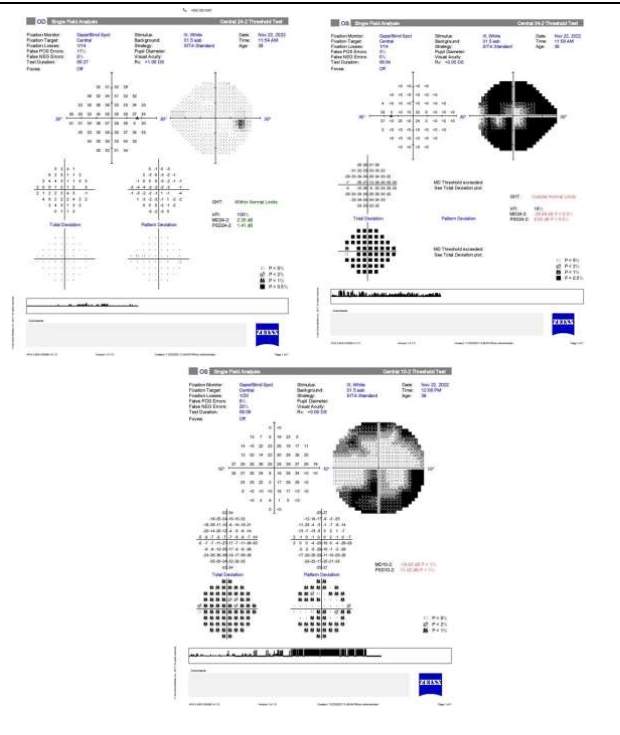
Figure 4. Automated visual field perimetry (Zeiss Humphrey machine). The patient’s AVF of the left eye showed severe generalized defects with clustered points of depression in all quadrants, while sparing the central field. Fixation was also affected and this could be caution for surgical procedures to be done due to the wipe-out phenomenon.
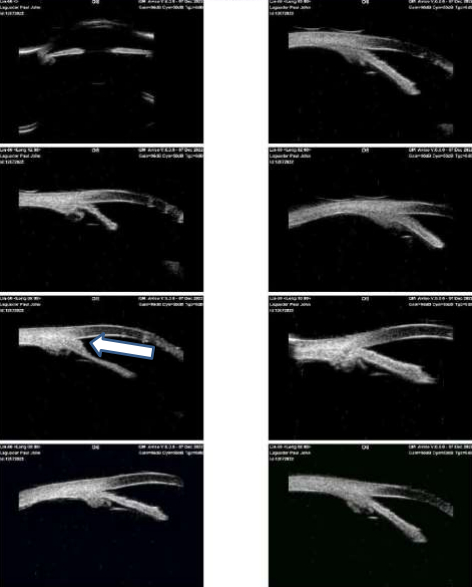
Figure 5. Pre-operative UBM of the left eye. The UBM shows a slightly shallow axial anterior chamber, flat iris configuration, several areas where the ciliary body has cysts, with some having iridotrabecular contact. Several areas with iridotrabecular contact due to peripheral anterior synechiae (white arrow). The superotemporal iridocorneal angle was deemed a suitable area for GDD implantation.
On the first day post-operation, the patient’s visual acuity was only hand movement with good light projection. There was hyphema inferiorly and blood clots over the tube as seen in Figure 6. The cornea was hazy and Descemet membrane folds were noted. The intraocular pressure was 7 mmHg. Atropine and sodium chloride were added to the post-operative medications and the patient was discharged.
Figure 6. Slit lamp photo 1st day status post CLE with IOL + GDD. This slit lamp photo highlights the hyphema inferiorly and the blood clots surrounding the tube.
On follow-up at the glaucoma and cornea clinics one week after, patient noted sudden onset of left eye pain. Visual acuity was still hand movement with good light projection, but the IOP was elevated to 62 mmHg that was brought down to 37 mmHg after one tablet of acetazolamide. There was also noted bedewing of the left eye and blood clots around the area of the tube with +2 cells +2 flare. The patient was then restarted on Combigan and acetazolamide.
The patient then underwent anterior chamber wash out the next day. Intra- operatively, there was a membrane connected to the iris covering the tube. Tube priming was done but no further manipulation of the tube was done to prevent further bleeding and pain. Iridectomy was done over the area of the tube.
The next day, the tube was now more visible and placed in the sulcus. Visual acuity was still hand movement with good light projection with the IOP at 26 mmHg, probably from post-op inflammation. Combigan was continued for one week until it was discontinued when IOP was controlled to 10.
Figure 7. Slit lamp photo day after anterior chamber washout, membranectomy, and iridectomy. The tube is now visible and seen to be placed in the sulcus.
On subsequent follow-ups, the patient’s visual acuity improved, reaching a best corrected visual acuity of 20/21 on ETDRS. IOP was controlled for the most part without anti-glaucoma medications, at a range of 6-10 mmHg. However, at around 7 weeks post operation, when the patient was last seen by both the Glaucoma and External Diseases and Cornea services, the IOP was elevated to 14 mmHg and was treated with timolol.
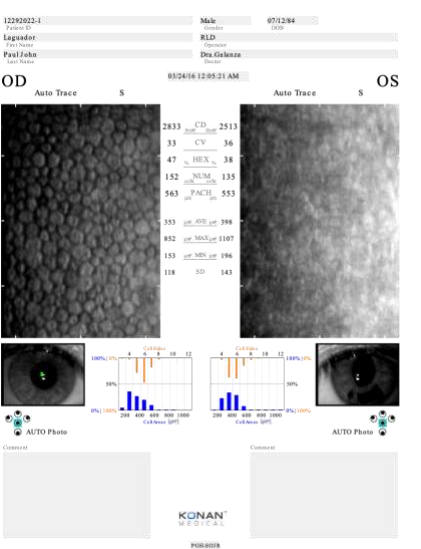
Figure 8. Specular microscopy. The left eye shows “ICE cells”.
The patient was scheduled for glaucoma drainage device (GDD) implantation on the left eye following a pre-operative ultrasound biomicroscopy (UBM). The UBM (Figure 5) showed that the GDD tube could be inserted at the superotemporal iridocorneal angle. Additional baseline specular microscopy was ordered. During the operation, clear lens extraction was performed while the cornea is still clear and an Aurolab Aqueous Drainage Implant (AADI) implanted valve implanted with the tube being placed further posteriorly at the sulcus.
Discussion
ICE syndrome can be classified into three clinical subtypes. The most prevalent variety is Chandler syndrome, which manifests with minor iris atrophy, corectopia, and a predominance of corneal and angle abnormalities. The symptoms of essential iris atrophy include heterochromia, corectopia, ectropion uveae, iris stromal and pigment epithelial atrophy, as well as hole formation. On the anterior iris surface, Cogan-Reese syndrome is characterized by tan pedunculated nodules or diffuse pigmented lesions.
In the case presented in this report, the patient had a corectopic pupil, iris atrophy and pedunculated iris nodules in the left eye. These findings were consistent Cogan- Reese syndrome.
Other diseases, like posterior polymorphous corneal dystrophy, could present as ICE syndrome. To differentiate one from the other, a specular microscopy could be ordered1. So-called “ICE cells” are described as dark cells with a light central spot and a light peripheral zone. ICE cells are usually bigger than normal endothelial cells. These are also seen in the areas of the cornea with the beaten bronze or hammered silver appearance. The endothelium is described as “epithelioid-like” with hyperreflective nuclei and irregularity of cell shape and size. All of these characteristics can be seen in the patient’s baseline specular microscopy. It also highlights the importance of a baseline specular microscopy in a patient with iris and pupillary abnormalities, even if the cornea is still clear, can help clinch the diagnosis of ICE syndrome. If there is corneal edema present that might obscure the view of the angles, an anterior segment optical coherence topography or UBM can be done to see if there are any PAS present [3].
Other glaucoma work-up like OCT of the optic nerve head and auto-visual field perimetry are also helpful in diagnosing and monitoring glaucoma in ICE syndrome. The patient’s baseline work-up can be seen in Figure 8.
In the case, the involved eye also developed glaucoma, but did not have corneal edema. ICE syndrome increases the risk of glaucoma, with over 70% of eyes with ICE syndrome developing glaucoma and half of the eyes developing corneal edema [5]. Medical management to control the intraocular pressure should be started immediately.
However, more than 50% of cases will require surgical management [5]. Trabeculectomy was commonly performed before, but as noted by Walkden et. al (2018) 1, 12.5 to 53.8%, patients would eventually require a glaucoma drainage device implantation. As noted by Doe et. al (2001) 6, GDD implantation had better survivability in the long term, which is why for our patient above, this was the procedure chosen [3].
Placement of the tube is also important to avoid it touching the cornea [7]. Doe’s study suggested to place the tube along the route of the sclera and lengthen the tube, as this would minimize the possibility of occlusion by the iris or an endothelial membrane. Additionally, it also allows for repositioning if needed. It is also important to avoid iris touch as this could accelerate synechia formation. Another option is if there is an iris defect or an iridectomy, the tube could be placed there as it will be far from the cornea and above the iris, to further decrease the chance of occlusion. If there is diffuse synechiae formation, the tube should be in placed in the sulcus or pars plana. This would necessitate lens extraction as it would create more operating space [6]. As with our patient, clear lens extraction was done while the cornea was also still clear, since corneal edema occurs in more than half of the cases of ICE. It also makes it easier for a graft to be done in the future if needed. If corneal decompensation occurs in the future, a PKP or DALK will be done.
Conclusion
ICE syndrome is a rare unilateral syndrome that typically affects females and can cause glaucoma. We report a case of Cogan-Reese Syndrome variant of ICE syndrome in a male patient. Early diagnosis, timely management, and close follow-up are paramount in preventing complications for this disease.
References
1. TANNA, A. N. G. E. L. O. P. (2022). 2022-2023 Basic and clinical science course, Section 10: Glaucoma Print. AMER ACADEMY OF OPHTHALMOLOGY.
2. Walkden, A., & Au, L. (2018). Iridocorneal endothelial syndrome: clinical perspectives. Clinical ophthalmology (Auckland, N.Z.), 12, 657–664. https://doi.org/ 10.2147/OPTH.S143132
3. Sacchetti, M., Mantelli, F., Marenco, M., Macchi, I., Ambrosio, O., & Rama, P. (2015). Diagnosis and Management of Iridocorneal Endothelial Syndrome. BioMed research international, 2015, 763093. https://doi.org/10.1155/2015/763093
4. Cogan-Reese Syndrome: A rare case of unilateral glaucoma. (n.d.). Retrieved February 26, 2023, from https://webeye.ophth.uiowa.edu/eyeforum/cases/275- cogan-reese-syndrome.htm
5. Chandran, P., Rao, H. L., Mandal, A. K., Choudhari, N. S., Garudadri, C. S., & Senthil, S. (2017). Glaucoma associated with IRIDOCORNEAL endothelial syndrome in 203 Indian subjects. PLOS ONE, 12(3). https://doi.org/10.1371/journal.pone.0171884
6. Doe, E. A., Budenz, D. L., Gedde, S. J., & Imami, N. R. (2001). Long-term surgical outcomes of patients with glaucoma secondary to the iridocorneal endothelial syndrome. Ophthalmology, 108(10), 1789–1795. https://doi.org/10.1016/s0161-6420(01)00725-4
7. Mittal, V., Mittal, R., & Maheshwari, R. (2014). Combined endothelial keratoplasty and clear lens extraction for corneal decompensation in irido-corneal endothelial syndrome. Indian journal of ophthalmology, 62(5), 651–653. https://doi.org/10.4103/0301-4738.118435
8. Paul A. Sidoti, M. D. (2016, February 5). Managing glaucoma with ice syndrome. Review of Ophthalmology. Retrieved March 5, 2023, from https:// www.reviewofophthalmology.com/article/managing-glaucoma-with-ice-syndrome.