Retrospective Observational Study on the Safety and Effectiveness of Ketamine as a Bronchodilator in Pediatric Asthma and Bronchiolitis
Retrospective Observational Study on the Safety and Effectiveness of Ketamine as a Bronchodilator in Pediatric Asthma and Bronchiolitis
Dr Sachin Padman 1*, Dr Tejaswini A 2, Venugopal Reddy I3
1. Director and Consultant Paediatrician Sunrise Hospital, Kanhangad, Kerala.
2. Junior consultant in Paediatricis, Sunrise Hospital Kanhangad , Kerala.
3. Medical Director and Consultant Pediatrician Ovum Hospital, Bangalore.
*Correspondence to: Dr Sachin Padman, Director and Consultant Paediatrician Sunrise Hospital, Kanhangad, Kerala
Copyright
© 2024: Dr Sachin Padman. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 March 2024
Published: 15 March 2024
Retrospective Observational Study on the Safety and Effectiveness of Ketamine as a Bronchodilator in Pediatric Asthma and Bronchiolitis
Introduction
Asthma is a chronic inflammatory disorder of the airways, characterized by increased airway hyper-responsiveness, recurrent episodes of wheezing, breathlessness, chest tightness, and coughing. In India, asthma rates are officially low, but recent evidence suggests a higher prevalence. The total estimated burden of asthma is 3%, with a median prevalence of 2.4% among adults over 15. Asthma exacerbations are a frequent cause of morbidity and mortality, and response to therapy is variable. Conventional therapies like nebulized albuterol, anti-cholinergics, theophylline, epinephrine, and corticosteroids are generally effective, but some patients require invasive ventilation due to worsening respiratory distress. Anesthetic agents like ketamine, isoflurane, sevoflurane, and halothane have bronchodilator properties, but no definite dosages and guidelines have been framed for severe refractory status asthmaticus. This review discusses the effects of ketamine on respiratory mechanics, its beneficial uses in refractory status asthmaticus, and potential adverse effects in context with available data.
Inclusion/Exclusion Criteria:
Inclusion: Children diagnosed with bronchial asthma or bronchiolitis, treated with ketamine between a specific timeframe (e.g., past 5 years).
Exclusion: Children with pre-existing neurological conditions, known history of ketamine misuse, or incomplete medical records.
Data Collection: Patient Demographics (age, sex, medical history) Diagnosis & Severity of Bronchial Asthma/Bronchiolitis Conventional Treatments Received Before Ketamine Ketamine Administration details (dosage, duration, route) Respiratory Parameters (e.g., oxygen saturation, wheezing scores) Clinical Outcomes (improvement in symptoms, need for mechanical ventilation, length of hospital stay) Adverse Events (hallucinations, sedation, changes in blood pressure)
Data Analysis: Descriptive statistics for patient demographics and outcomes. Univariate and/or multivariate analysis to identify associations between: Ketamine administration and clinical outcomes. Predictors of response to ketamine (e.g., age, diagnosis, severity). Occurrence of adverse events and associated factors.
Considerations: Ethical Approval: Ensure ethical approval from your institution, addressing data privacy and confidentiality.
Data Quality: Verify the accuracy and completeness of medical records. Selection Bias: Acknowledge potential limitations due to the retrospective nature (e.g., selection bias, confounding variables). Generalizability: Consider the specific patient population and setting.
Statistical Analysis
Statistical analysis of the data was performed using SPSS 23.0. The Categorical variables were presented as frequency and percentage. The continuous variables were presented as mean ± SD. Comparison between the groups was done using ANOVA followed by Bonferroni. A p value <0.05 was considered statistically significant
Table1: Age distribution
Table 2: Distribution based on gender
Table 3:mean and SD of weight
Table 4: Duration of presenting illness
Table 5: History
Table 6: Family history of asthma / atopy
Table 7: Past history
Table 8: Diagnosis
Table 9: Pram score
Table 10: PICU stay
Table 11: treatment before admission
Table 12: Ketamine initiated
Table13:Duration of Ketamine infusion
Table 14:Temperature
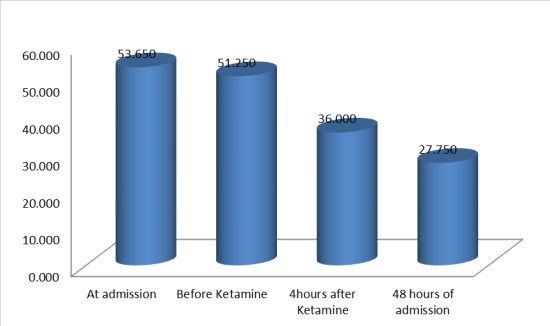
Table 15: RR
Table 16: Multiple comparison of RR
The p-values in the multiple comparison table indicate the statistical significance of the differences in respiratory rate (RR) between various time points. In each comparison, the p-value is less than 0.05, indicating that the observed differences are statistically significant.
Figure 1
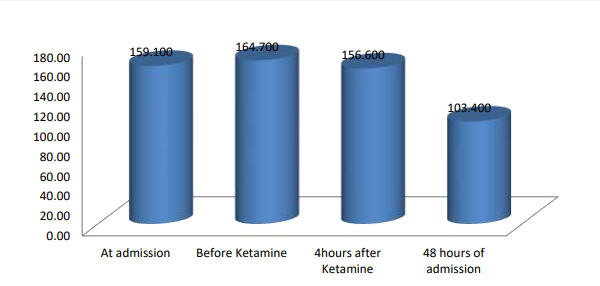
Table 17 : HR
At admission: 159.100 ± 9.619 beats per minute,Before Ketamine: 164.700 ± 9.342 beats per minute,4 hours after Ketamine: 156.600 ± 8.762 beats per minute,48 hours post-admission: 103.400 ± 5.688 beats per minute.These values indicate statistically significant changes in HR over time.
Table 18: Multiple comparison in HR
Figure 2
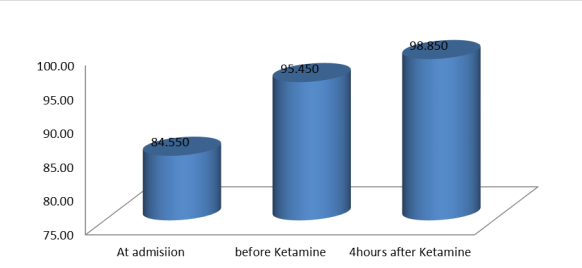
Table 19:SPO2
Figure 3
Table 20 : Multiple comparison in SPO2
Table 21: Adverse, Hallucination, HT, disorientation, trachebrochial secretators and Glycopyyrolate received
please click here to view all tables and figures
Discussion
The majority of the population surveyed was between 1 and 6 years old, with 75.0% of the total being males and 10.0% females. The weight data for the 20 individuals ranged from 6.00 to 26.00 units, with an average weight of 13.7300 units and a standard deviation of 4.83682 units. The duration of presenting illness was most common (60.0%), with most individuals reporting a duration of 1 day. The most common symptoms were fever, cough, and breathing difficulty, accounting for 30.0% of cases.
The majority of respondents (80.0%) reported no family history of asthma or atopy. A significant portion (50.0%) reported no specific past medical issues. WALRI was the most commonly mentioned condition, comprising 30.0% of cases. Other conditions such as allergic rhinitis, intermittent wheezing, and combinations thereof represented 5.0% of the total cases.
The majority (85.0%) were diagnosed with lower respiratory tract infections (WALRI), bronchiolitis, and acute severe asthma. PRAM scores were the most common, representing 35.0% of cases, followed by scores of 8.00 and 11.00, each at 15.0%. The length of Pediatric Intensive Care Unit (PICU) stays was the most common, with 60.0% having a stay of 4 days, 30.0% with a stay of 5 days, and a smaller proportion (10) having a stay of 3 days.
All individuals initiated ketamine through a 5 mic/kg/min IV infusion, representing 100.0% of the cases. The mean heart rate (HR) data indicated significant fluctuations over different time points, with the mean dropping to 36.000 ± 4.779 breaths per minute after 4 hours and further decreasing to 27.750 ± 2.221 breaths per minute 48 hours post-admission.
At admission, the mean SpO2 (blood oxygen saturation level) was 84.550%, significantly improved to 95.450% before ketamine administration. Following ketamine infusion, there was a further increase in SpO2 levels, reaching 98.850% 4 hours afterward.
Among adverse events, tracheo bronchial secretion was the most commonly reported, accounting for 30.0% of cases. The majority of individuals (65.0%) did not experience any adverse events. Regarding specific medical conditions, all surveyed individuals reported no occurrences of hallucination, hypertension, or disorientation. However, tracheobronchial secretions were noted in 35.0% of cases, while 7 individuals (35.0%) received glycopyrrolate.
Conclusion
Ketamine is a versatile and inexpensive drug used as a bronchodilator in severe status asthmaticus refractory to routine medications. It has been found to eliminate the need for mechanical ventilation in various studies due to its limited side effects. However, its use in asthma is debated due to a lack of randomized studies and information on its optimum dose. Physicians typically administer bolus doses ranging from 0.1-2 mg/kg and continuous infusions from 0.15 to 2.5 mg/kg/hr. Most studies have small sample sizes and lack control groups, and the dosage and duration of conventional medication are not mentioned. Reporting bias is likely, and ketamine is considered a potent bronchodilator for refractory status asthmaticus. Further well-designed studies are needed to identify its role in acute asthma.
References
1. Ebert B, Mikkelsen S, Thorkildsen C, Borgbjerg FM. Norketamine, the main metabolite of ketamine, is a non-competitive NMDA receptor antagonist in the rat cortex and spinal cord. Eur J Pharmacol. 1997;333:99–104. [PubMed] [Google Scholar]
2. Grant IS, Nimmo WS, McNicol LR, Clements JS. Ketamine disposition in children and adults. Br J Anaesth. 1983;55:1107–11. [PubMed] [Google Scholar]
3. Qureshi FA, Mellis PT, McFadden MA. Efficacy of oral ketamine for providing sedation and analgesia to children requiring laceration repair. Pediatr Emerg Care. 1995;11:93–7. [PubMed] [Google Scholar]
4. Roelofse JA, Joubert JJ, Swart LC, Stander I, Roelofse PG. An evaluation of the effect of oral ketamine and standard oral premedication in the sedation of paediatric dental patients. J Dent Assoc S Afr. 1996;51:197–201. [PubMed] [Google Scholar]
5. Bourke DL, MAlit LA, Smith TC. Respiratory interactions of ketamine and morphine. Anesthesiology. 1987;66:153–6. [PubMed] [Google Scholar]
6. Hamza J, Ecoffey C, Gross JB. Ventilatory response to CO2 following intravenous ketamine in children. Anesthesiology. 1989;70:422–25. [PubMed] [Google Scholar]
7. Mankikian B, Cantineau JP, Sartene R, Clergue F, Viars P. Ventilatory pattern of chest wall mechanics during ketamine anesthesia in humans. Anesthesiology. 1986;65:492–99. [PubMed] [Google Scholar]
8. Shulman D, Beardsmore CS, Aronson HB, Godfrey S. The effect of ketamine on the functional residual capacity in young children. Anesthesiology. 1985;62:551–56. [PubMed] [Google Scholar]
9. Betts EK, Parkin CE. Use of ketamine in an asthmatic child. Anesth Analg. 1971;50:420–1. [PubMed] [Google Scholar]
10. Corssen G, Gutierrez J, Reves JG, Huber FC., Jr Ketamine in the anesthetic management of asthmatic patients. Anesth Analg Curr Res. 1972;51:588–96. [PubMed] [Google Scholar]
11. Youssef-Ahmed MZ, Silver P, Nimkoff L, Sagy M. Continuous infusion of ketamine in mechanically ventilated children with refractory bronchospasm. Intensive Care Med. 1996;22:972–6. [PubMed] [Google Scholar]
12. Hemmingsen C, Nielsen PK, Odorico J. Ketamine in the treatment of bronchospasm during mechanical ventilation. Am J Emerg Med. 1994;12:417–20. [PubMed] [Google Scholar]
13. Shlamovitz GZ, Hawthorne T. Intravenous ketamine in a dissociating Dose as a temporizing measure to avoid mechanical ventilation in adult patient with severe asthma exacerbation. J Emerg Med. 2008;41:492–4. [PubMed] [Google Scholar]
14. Strube PJ, Hallam PL. Ketamine by continuous infusion in status asthmaticus. Anaesthesia. 1986;41:1017–9. [PubMed] [Google Scholar]
15. Jahangir SM, Islam F, Chowdhury SN, Aziz L, Ghani MA. Ketamine infusion for postoperative analgesia: A prospective cohort study in asthmatics. Bangladesh Med Res Counc Bull. 1993;19:21–7. [PubMed] [Google Scholar]
16. Achar MN, Achar KN. Efficacy of ketamine infusion in refractory asthma complicated by acute myocardial infarction. Anaesth Intensive Care. 1993;21:115–7. [PubMed] [Google Scholar]
17. Park GR, Manara AR, Mendel L, Bateman PE. Ketamine infusion. Its use as a sedative, inotrope and bronchodilator in a critically ill patient. Anaesthesia. 1987;42:980–3. [PubMed] [Google Scholar]
18. Huber FC, Jr, Reves JG, Gutierrez J, Corssen G. Ketamine: Its effect on airway resistance in man. South Med J. 1972;65:1176–80. [PubMed] [Google Scholar]
19. Petrillo TM, Fortenberry JD, Linzer JF, Simon HK. Emergency department use of ketamine in pediatric status asthmaticus. J Asthma. 2001;38:657–64. [PubMed] [Google Scholar]
20. Heshmati F, Zeinali MB, Noroozinia H, Abbacivash R, Mahoori A. Use of ketamine in severe status asthmaticus in intensive care unit. Iran J Allergy Asthma Immunol. 2003;2:175–80. [PubMed] [Google Scholar]
21. Howton JC, Rose J, Duffy S, Zoltanski T, Levitt MA. Randomized, double-blind, placebo-controlled trial of intravenous ketamine in acute asthma. Ann Emerg Med. 1996;27:170–5. [PubMed] [Google Scholar]
22. Allen JY, Macias CG. The efficacy of ketamine in pediatric emergency department patients who present with acute severe asthma. Ann Emerg Med. 2005;4:43–50. [PubMed] [Google Scholar]
23. Rock MJ, Reyes de la Rocha S, L’Hommedieu CS, Truemper E. Use of ketamine in asthmatic children to treat respiratory failure refractory to conventional therapy. Crit Care Med. 1986;14:514–16. [PubMed] [Google Scholar]
24. Fisher MM. Ketamine hydrochloride in severe bronchospasm. Anesthesia. 1977;32:771–2. [PubMed] [Google Scholar]
25. Turnpenny PD, Nash SF. Ketamine in severe acute asthma. Arch Emerg Med. 1991;8:291–2. [PMC free article] [PubMed] [Google Scholar]
26. Hemming A, MacKenzie I, Finfer S. Response to ketamine in status asthmaticus resistant to maximal medical treatment. Thorax. 1994;49:90–1. [PMC free article] [PubMed] [Google Scholar]
27. Galbis-Reig D, Rasansky MA. A case presentation and literature review of successful ketamine administration in a patient with refractory status asthmaticus. Internet J Intern Med. 2004;5:31. [Google Scholar].