Awareness of Breast Cancer Screening among the Educational Fraternities: A Requisite Students, College Lecturer and School Teachers
Awareness of Breast Cancer Screening among the Educational Fraternities: A Requisite Students, College Lecturer and School Teachers
Aravind-Kumar Radhakrishnan1,2,3 ,Shashikala Narayanaswamy3 ,Ramya Kodandapani3 , Hemamalathi Aravindkumar 3,4 , Kasthuri Natarajan6 , Jayaraman Tharmalingam7 , Shalini Priya3 , Elisha Sundararajan 3,5
1. Charité University Medicine, Charité Campus Virchow, Berlin, Germany
2. Jerarsi Clinic, Tbilisi, Georgia
3. Lets Focus Health, India
4. Vivantas Hospital GmbH
5. Panchayat Union Middle School Pernambut,
6. SRM Medical College Hospital and Research Centre
7. Biomedical engineering department, University of Houston, Houston, Texas, USA
*Correspondence to: Aravind-Kumar Radhakrishnan, Jerarsi Clinic, Tbilisi, Georgia, Department of Internal Medicine and Cardiology, Charité University Medicine, Campus.
Copyright
© 2024 Aravind-Kumar Radhakrishnan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2024
Published: 29 March 2024
Abstract
Background: Breast cancer is the most common cancer in among women. India is placed in second place in the world which recorded 1,62,468 incidences and 87,090 deaths reported in the year 2018. In this situation, it is incredibly essential to create awareness among the younger population about the breast cancer symptoms. Self-screening is the most effective way to prevent the fatal breast cancer. Early detection of breast cancer reduced the mortality rate and proved that early prevention is an effective fight against breast cancer. In India, culture influence and social stigma prevent the self- awareness among population irrespective of education status. Though early detection through screening can be treatable, there is a high mortality rate due to late stage diagnosis in our country. Hence, it is important that every woman must have a knowledge on breast self-examination.
Methods: A cross-sectional survey among students, college lecturers and teachers were conducted through a self-run questionnaire to evaluate the participant’s awareness and knowledge on breast self- examination. A total of 606 participants which include students, college lecturers and teachers from the awareness webinar programs successfully completed the survey after the webinar on breast cancer awareness.
Results: It was observed that most of the participants were not aware about the importance of monthly breast self-examination and early signs and changes in shape and color of the nipple. Based on the questionnaires, it was noted that many of the participants irrespective of the professional qualifications did not have any knowledge about the self-screening method which is the easiest way to identify early signs of breast cancer. The webinar provided an opportunity to the participants to self-screen themselves after the session. Among the study participants 39% were of less than 30 years and 61% were above 30 years of age. We observed maximum percentage of individuals in students 38%, faculty with higher degree 28% and faculty with doctorate 34% never undergone self-examination of breast before this awareness session. Others failed to do subsequent breast self- examination. Nearly 5 members with age above 30 years have reported unusual changes and abnormalities in the breast.
We found the incidence of 1% among 505 individuals have abnormalities and may develop breast cancer through our survey analysis. This indicates that 1000 in 1,00,000 population may have chance of developing breast cancer providing an eye opener in our society.
Conclusion: This report was an initiative to involve many volunteers to spread the message on early symptoms of breast cancer to reach everywoman of our community. The survey after the session has emphasized on the importance of promoting awareness on breast cancer early screening methods among women. Also, the information obtained marks the requisite for Health and Education department to organize several awareness programs which is the need of the hour.
Keywords: Breast cancer, awareness, self-examination
Awareness of Breast Cancer Screening among the Educational Fraternities: A Requisite Students, College Lecturer and School Teachers
Background
Breast cancer is the most common cancer in women and accounts for 15% of cancer deaths worldwide. Nearly 627,000 deaths of women with breast cancer have been reported in 2018 (www.who.in). India is found to be the second highest wherein 1,62,468 women were detected with breast cancer and 87,090 deaths reported in the year 2018 (www.breastcancerindia.net). However these facts and figures are likely to increase with the globalising scenario, and the present life style exposures beats an alarming situation. In this situation, it is incredibly essential to create awareness among the younger population about the breast cancer symptoms. As early detection through screening can be treatable, it is important that every women must have a knowledge on how a normal breast looks, and, when to recognise the changes that can arise due to breast cancer. This can have a great impact on the health care of individuals being affected and can benefit with early detection, diagnosis as well as reduction in the death rate pertaining to breast cancer. Having based on the above said facts, an informative session by medical experts on breast cancer awareness, self-examination, screening and treatment options were discussed. It was observed that many of the participants; faculties and students from various organisations were not aware of the breast cancer early symptoms. This session created an immediate response with them for a regular need based self-check on breast cancer early symptoms.
Worldwide, breast cancer is the most common invasive cancer in women. India is placed in second place in the world which recorded 1,62,468 incidences and 87,090 deaths reported in the year 2018.In India Breast cancer accounts for 25 to32% of female cancers in women, more than 1/4th of all female cancers. It is reported that with every 4min an Indian woman is diagnosed with breast cancer. Breast cancer is on the rise, both rural (1 in 22)and urban(1 in 60) India. One in twenty eight women is likely to develop breast cancer during her lifetime. Cancer survival becomes difficult in higher stages of its growth, more than 50% of Indian women suffer from stage 3 or stage 4 of breast cancer. Post cancer survival for women with breast cancer was reported 60% in women as compared to 80%in the US. The reason for low survival rate accounts from its lack of awareness, poor early screening and diagnosis. As per latest reports, highest cancer rate is listed in state of Kerala, other states include Mizoram, Haryana, Delhi and karnataka. New figures of rise in breast cancer spell a startling future – its time we took preventive measures. There is no escaping the fine print –BC is the most common form of cancer in the country, having overtaken cervical cancer. Its also more common in younger age group. Almost 50%in the age group 25 to 50 yrs. More than 70% present in advanced stage with poor survival and high mortality. As per Indian council for medical research report new cases are likely to increase upto 17.3lakhs in 2020, when compared to 14.5lakh new cases in 2014.The only way to change these numbers is by increasing awareness. The simplest way for prevention of breast cancer is by being able to do self- breast Examination.
Methods
Briefly explain about the highlights of the awareness program. Then mention about total participants, inclusion and exclusion criteria…
Total Participant(606)
Included in the study 505, Excluded 101 due to incomplete data
Flow chart
Sampling and data collection:
A cross-sectional survey among students, college lecturers and teachers were conducted through a self-run questionnaire to evaluate the participant’s awareness and knowledge on breast self- examination. A total of 606 participants which include students, college lecturers and teachers from the awareness webinar programs successfully completed the survey after the webinar on breast cancer awareness, in which 101 were excluded due to incomplete data, eligible for our analyses were only 505.
Data were screened, sorted and analysed for the observation of awareness on breast self- examination among the individuals participated in the awareness program. Raw Data obtained from the awareness questionnaire master chart were categorized based on age, educational status and period of breast self-examination.
The percentage of knowledge and awareness was calculated among 505 women. The frequency of breast self-examination was assessed based on age group (less than 30 and greater than 30), educational status (students, faculties with higher degree and faculties with doctorate) and period of breast self-examination (never, more than a year, less than a year, within a month and within a week). The association was analysed using chi square and fisher exact statistic by SPSS software.
Discussion and Results
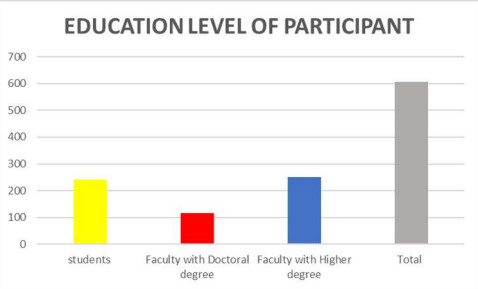
Questionnaires were presented to 606 women participants, all agreed to fill the questionnaire, among them 240 were students, 250 were faculties with higher degree and 116 were faculties with doctorate (Figure 1). Due to incomplete data, only 505 women were included in this study. We discussed about the importance of monthly breast self-examination and early signs and changes in shape and color of the nipple and their education background of all participants.
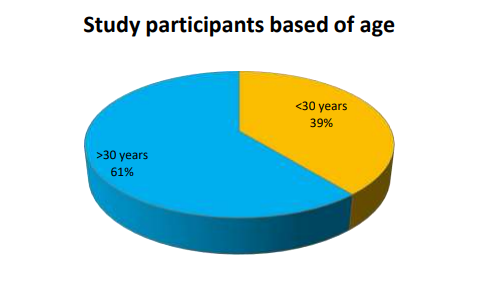
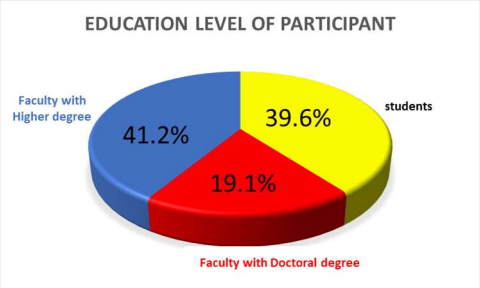
Among 505 study participants 39% were between 18 – 30 years and 61% were within 31 to 50 years of age (Figure 2). Proportion of women based on educational status, 39.6% students, 41.2% faculties with higher degree and 19.1% faculties with doctorate were participated and included in this study (Figure 3).
Figure 1: Survey analysis study population
Figure 2: Age group of study participants
Figure 3: Educational status of study participants
Frequency of Breast Self-Examination (BSE) based on educational status:
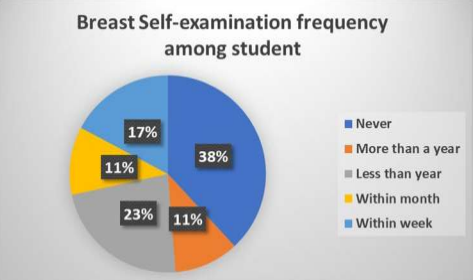
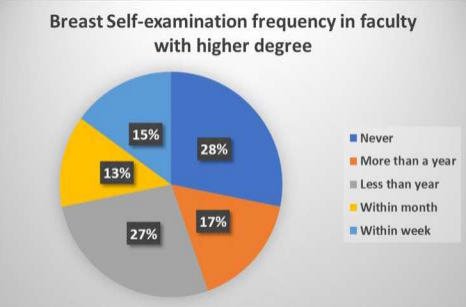
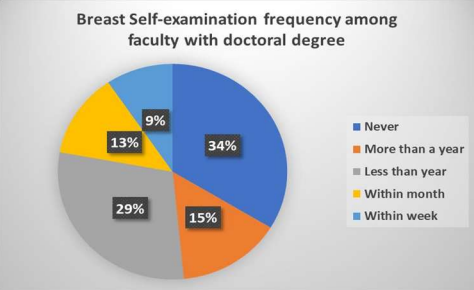
Percentage of breast self-examination frequency among students has shown that 38% never done, 11% more than a year and 28% less than a year (Figure 4). The percentage frequency of breast self-examination among faculty with higher degree indicates 28% never, 17% more than a year and 27% less than a year (Figure 5). Even faculties with doctorate had shown the breast self- examination frequency percentage as 34% never, 15% more than a year and 29% less than a year in our survey report analysis (Figure 6). These results suggest that the lack of awareness about the sequential breast self-examination among the women in our study population.
Figure 4: Percentage of BSE frequency among Students
Figure 5: Percentage of BSE frequency among faculty with higher degree
Figure 6: Percentage of BSE frequency among faculty with doctoral degree
Association analysis among participants with abnormal findings:
We are grateful to report that from the survey analysis there is no significant abnormal finding in breast self-examination among the educated women participated in our study. We observed the breast abnormality during the self-examination after the awareness program in 5 women of 505 participants. All the 5 were more than 30years of age with higher professionals. Even though we found less number of individual with abnormal findings in breast suggest around 1% of study participant may develop breast cancer. The risk will be 1 in 100 participants. Risk assessment based on the age group we observed risk value of 0.02 and odds value of 0.02 in the population with age > 30 years. We did not observe any risk in age group < 30 years as well known. The relative risk will be greater in population above 30 years of age. Our study report the incidence 1000 in 100000 population may have a chance to develop breast cancer and wakeup call of consecutive breast self-examination for women in our society. (Table 1 – 2)
Table 1: Statistic analysis among survey responders based on educational status and abnormal findings
|
Breast cancer |
Chi square statistic (P Value) |
Chi square yates (P value) |
Fisher exact statistic |
|
Responders * Findings |
0 (1) |
0.303 (0.582) |
1 |
|
Students * Findings |
1.2864 (0.257) |
0.509 (0.476) |
0.1619 |
|
Faculties * Findings |
2.9621 (0.852) |
1.6028 (0.206) |
0.1674 |
|
Doctorates * Findings |
0.0047 (0.976) |
0.2567 (0.612) |
1 |
Table 2: Statistic analysis among survey responders based on age group and abnormal findings
|
Breast cancer |
Chi square statistic (P value) |
Chi square yate(P value) |
Fisher exact statistic |
|
Age * Findings |
1.2864 (0.257) |
0.509 (0.476) |
0.1619 |
Conclusion
This study raises important issues for future public health initiatives in our society. Self- examination remains a key method of Breast Cancer early detection
This report was an initiative to involve many volunteers to spread the message on early symptoms of breast cancer to reach everywoman of our community. The survey after the session has emphasized on the importance of promoting awareness on breast cancer early screening methods among women. Also, the information obtained marks the requisite for Health and Education department to organize several awareness programs which is the need of the hour.
Reference
1. Muhammad Akram , Mehwish Iqbal , Muhammad Daniyal , Asmat Ullah Khan Awareness and current knowledge of breast cancer Biol Res . 2017 Oct 2;50(1):33. doi: 10.1186/s40659-017-0140-9.
2. Máirín O'Mahony, Harry Comber, Tony Fitzgerald, Mark A Corrigan Interventions for raising breast cancer awareness in women Cochrane Database Syst Rev 2017 Feb 10;2(2):CD011396.
3. Shatabdi Paul , Prem Prakash Solanki, Uday Pratap Shahi , Saripella Srikrishna Epidemiological Study on Breast Cancer Associated Risk Factors and Screening Practices among Women in the Holy City of Varanasi, Uttar Pradesh, India Asian Pac J Cancer Prev, 16 (18), 8163-8171
4. Rajendra A Badwe , Rajesh Dikshit, M Laversanne, Fredie Bray Cancer incidence trends in India Jpn J Clin Oncol. 2014 May;44(5):401-7. doi: 10.1093/jjco/hyu040. Epub
5. Mara Y. Roth, M.D., Joann G. Elmore, M.D., M.P.H.,Joyce P. Yi-Frazier, Ph.D., Lisa M. Reisch, Ph.D.,Natalia V. Oster, M.P.H.,and Diana L. Miglioretti, Ph.D. Self- Detection Remains a Key Method of Breast Cancer Detection for U.S. Women, J Womens Health (Larchmt). 2011 Aug; 20(8): 1135–1139
6. Rahman SA, Al-Marzouki A, Otim M, Khalil Khayat NEH, Yousuf R, Rahman P. Awareness about Breast Cancer and Breast Self-Examination among Female Students at the University of Sharjah: A Cross-Sectional Study. Asian Pac J Cancer Prev. 2019 Jun 1;20(6):1901-1908. doi: 10.31557/APJCP.2019.20.6.1901. PMID: 31244316; PMCID: PMC7021607.
7. Ahmed BA. Awareness and practice of breast cancer and breast self-examination among university students in Yemen. Asian Pac J Cancer Prev. 2010;11:101–5. [PubMed] [Google Scholar]
8. Al-Sharbatti SS, Shaikh RB, Mathew E, Al-Biate MA. Assessment of breast cancer awareness among female university students in Ajman, United Arab Emirates. Sultan Qaboos Univ Med J. 2014;14:e522. [PMC free article] [PubMed] [Google Scholar]
9. American Cancer Society. Breast cancer facts and figures. 2008. [Accessed April 18, 2019.sed April 15, 2019]. http://www.cancer.org/downloads/STT/CAFF2005BrFacspdf2005.pdf.
10. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. [PubMed] [Google Scholar]
11. Boulos DN, Ghali RR. Awareness of breast cancer among female students at Ain Shams University, Egypt. Glob J Health Sci. 2014;6:154. [PMC free article] [PubMed] [Google Scholar]
12. Chaudhary SB. Cancer cases to double by 2030 in Middle East. Gulf NewsHealth. 2018;13:28. [Google Scholar]
13. Emirates 24/7 News (2014, November 13). 39 women died of breast cancer in UAE in 2013. [Accessed March 2, 2017]. http://www.emirates247.com/news/emirates/39- women-died-of-breast-cancer-in-uae-in-2013-2014-11-13-1.569816.
14. Emirates 24/7 News (2016, January 10) Cancer the third leading cause of death in UAE. [Accessed May 12, 2017]. http://www.emirates247.com/news/emirates/cancer-the- third-leading-cause-of-death-in-uae-2010-09-20-1.293190.
15. Erbil , Bolukbas N. Health beliefs and breast self-examination among female university nursing students in Turkey. Asian Pac J Cancer Prev. 2014;15:6525–9. [PubMed] [Google Scholar]
16. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:359–86. [PubMed] [Google Scholar]
17. Forbes L, Atkins L, Ramirez A, Haste F, Layburn J. Awareness of breast cancer among women living in inner North East London. King’s College, London; 2010. [Google Scholar]..