Patient Specific Implant Supported Prosthetic Rehabilitation of a Post Mucormycosis Brown II Maxillectomy Defect: A Clinical Report
Patient Specific Implant Supported Prosthetic Rehabilitation of a Post Mucormycosis Brown II Maxillectomy Defect: A Clinical Report
Vinay Narender Wadhwa 1, Karan Padha *2
1.Graded Specialist (Prosthodontics), AFDC, New Delhi, India.
2.Graded Specialist (Oral & Maxillofacial Surgery), AFDC, New Delhi, India.
*Correspondence to: Karan Padha, Graded Specialist (Oral & Maxillofacial Surgery), AFDC,
New Delhi, India.
Copyright
© 2024 Karan Padha. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 March 2024
Published: 29 March 2024
Abstract
Background
Patients undergoing ablative tumor surgery of the mid face are faced with functional and esthetic challenges despite various reconstructive strategies available. The commonly used reconstruction modalities like implant-borne obturator prosthesis or microvascular tissue transfer have their own set of limitations. In the paper presented, PSIs with 3 integrated internal hex of implants were used and pedicled temporalis muscle flap was used for soft tissue coverage.
Results
The PSI was designed to gain anchorage from the zygomatic and the nasomaxillary buttress with soft tissue coverage being accomplished using pedicled temporalis flap tunnelled below the zygomatic arch. The implants were carefully planned to have abutments aligned with the teeth present in the mandible and to avoid any offset loading as a result of a cantilever. After 6 weeks, surgical exposure of the prosthetic components was done and impressions were made with polyvinyl siloxane impression material and the intermaxillary jaw relationship was recorded using aluminum-containing wax. The interim prosthesis followed by a Porcelain fused to Metal (PFM) permanent prosthesis was planned and cemented.
Conclusions
In this case report, we present a new prosthetic rehabilitation option in a post mucormycosis maxillectomy defect with patient specific implant reconstruction using a scientifically optimized protocol and stringent biomechanical and dimensional testing in the form of FEA and GOM analysis. It thus adds to the rehabilitation options available for the prosthodontist for reconstruction in the maxillofacial region thus paving for a new era in reconstruction.
Keywords: Patient Specific Implant, Maxillofacial Reconstruction, Mucormycosis.
Patient Specific Implant Supported Prosthetic Rehabilitation of a Post Mucormycosis Brown II Maxillectomy Defect: A Clinical Report
List of Abbreviations
PSI: Patient Specific Implant
CT: Computed Tomography
FEA: Finite Element Analysis
PFM: Porcelain fused to Metal
SLA: Stereolithography
CAD CAM: Computer assisted design Computer assisted manufacturing.
Background
Ablative tumor surgery of the midface often leads to esthetic and functional limitations that burden patients physically as well as psychologically. A wide variety of reconstructive procedures have been described ranging from intra-oral obturators to pedicled and free tissue transfer reconstruction modalities [1]. Recently, patient specific implants with advantages like reduced duration of surgery, prediction of failure due to FEA analysis and biomechanical accuracy have become the prime alternative and represent the next frontier in maxillofacial reconstruction. This case report presents the prosthetic rehabilitation of a post mucormycosis Brown II Maxillectomy defect using patient specific implant reconstruction.
Case Presentation
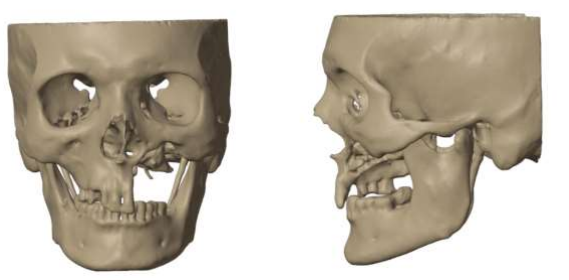
A 55-year-old man was referred to the Department of Prosthodontics with complaints of hypernasal speech, nasal regurgitation, and oroantral communication. He had undergone post Mucormycosis partial maxillectomy (Left Maxilla) and had not received any prosthetic rehabilitation (Figure 1). The patient presented with oroantral communication and difficulty in speech and mastication.
The extraoral and intraoral examination revealed the absence of the maxilla, hard palate, and nasal floor of the left side. The nasolabial fold was obliterated, with drooping of the corners of his mouth, and insufficient upper lip support. The patient was classified as having Brown II maxillectomy defect with the aim of the reconstruction being to obturate the defect and restore the facial profile and function. The main goal was to deliver a patient specific implant supported prosthesis in which the intaglio surface of the prosthesis would share the support and stabilization functions and the retention would be dependent on the implants.
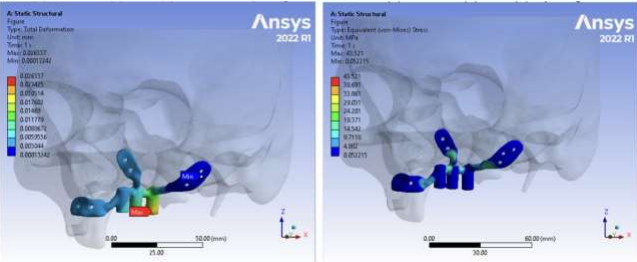
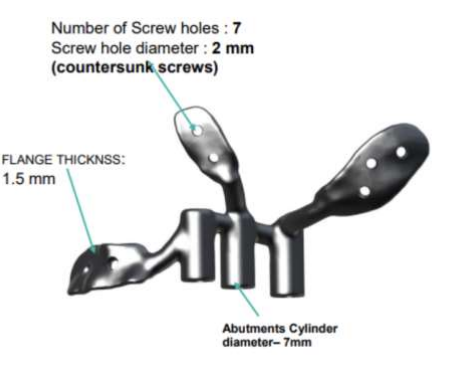
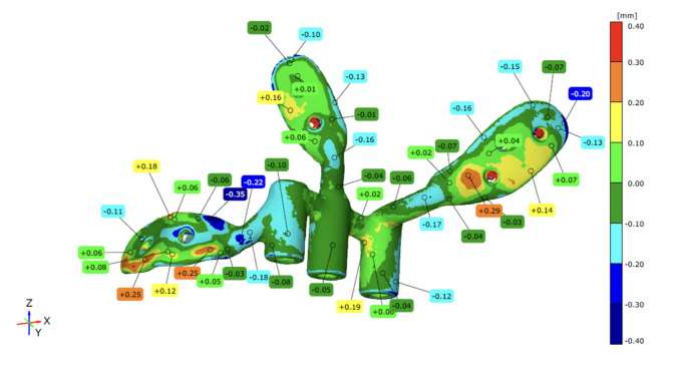
The patient underwent CT scan and subsequently the DICOM data was sent to the engineering team. The virtual planning was done using MIMIC software for segmentation and BLENDER software for final designing (Figure 2). The models were sent for FEA analysis to pass a set of standardised protocols in which nodal points were used to solve equation for stress with different colors representing load distribution for visualization purposes with blue signifying minimum stress and red signifying maximum stress. The implanted maxilla was subjected to biting and chewing simulations with a compressive force of 300 N and the von Misses stress on the implant was measured to be 43.521 MPa, which was much lesser than the allowable limit of 830 MPa thus indicating the PSI design to be biomechanically and functionally stable (Figure 3). An SLA printer was used to print a polymer resin prototype for final consultation with the operating surgeon before metal printing (Figure 4). The powder size was kept 30 microns with a layer thickness of 20-80 micrometer. Scanning speed was kept 4.5 meter/second with the laser power being 100 W. The transitional fillet radius of the implant was 1.5mm with the bending stress calculated being 107.14 MPa. “I style” fixation plate was adopted over the “L style” as it is the only configuration possible in the maxilla and staggered countersink holes with an angulation of 45 degrees were used. The implants were printed using Ti6Al4V titanium alloy and tested for accuracy using GOM software which is used for generating report for surface analysis and deviation with a 3D scanner being used to scan the finished 3D printed model to compare the surface deviations. Maximum deviation of 0.29 mm was observed for the maxillary PSI which was lesser than the acceptable limit of +/- 0.4 mm as per quality standards (Figure 5).
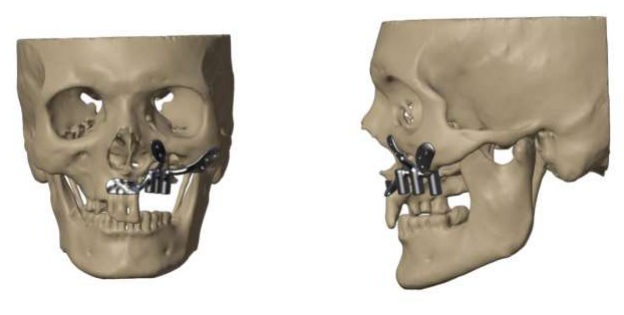
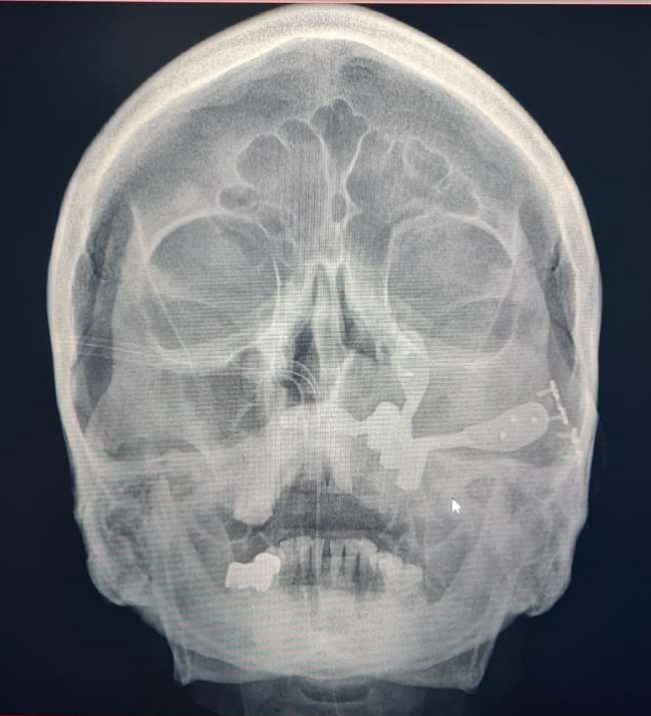
The PSI was designed to gain anchorage from the zygomatic and the nasomaxillary buttress with soft tissue coverage being accomplished using pedicled temporalis flap tunnelled below the zygomatic arch (Figure 6,7).
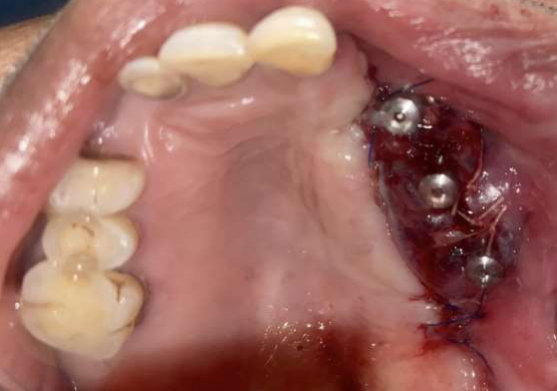
The implants were carefully planned to have abutments aligned with the teeth present in the mandible and to avoid any offset loading as a result of a cantilever. According to literature and also according to the authors experience, the PSI should be kept submerged for at least 6-8 weeks before second stage surgery thus allowing adequate time for healing and stabilisation of the soft tissue component (Figure 8). After waiting for 6 weeks, surgical exposure of the prosthetic components was done, impressions were made with polyvinyl siloxane impression material and the intermaxillary jaw relationship was recorded using aluminum-containing wax (Aluwax; Aluwax Dental Products) (Figure 9,10). The interim prosthesis was delivered and a Porcelain fused to Metal (PFM) permanent prosthesis was planned. A metal try in was done followed by cementation of the final prosthesis (Figure 11). Utilizing high quality porcelain-fused-to-metal, the prosthesis achieved both durability and aesthetic appeal (Figure 12). Gingival porcelain was added to compensate for the lost soft tissue. Occlusal adjustments were made, and speech quality was evaluated. This prosthetic concept achieved patient satisfaction, restored masticatory function, markedly improved speech and improved the lost facial profile contour and lip support.
Figure 1: Maxillary defect post Mucormycosis
Figure 2: 3D virtual planning of PSI in Mucormycosis case
Figure 3: FEA analysis
Figure 4: PSI design
Figure 5: GOM analysis
Figure 6: PSI fixation
Figure 7: Post op PA view
Figure 8: Pedicled temporalis muscle for soft tissue coverage
Figure 9: Exposure of the prosthetic components
Figure 10: Attachment of the abutments
Figure 11: Metal try in
Figure 12: The final prosthesis in place
Please click here to view all figures
Discussion
Autologous bone grafting and prosthodontic restoration using obturators represent the most commonly used techniques for post-ablative maxillary reconstruction. Both treatment options have their individual disadvantages, with autologous bone grafts having issues of donor-site morbidity and risk of graft loss whereas obturators can have nasal leakage, instability as well as limited mouth opening makes insertion of an obturator prosthesis difficult [2,3].
In the paper presented, PSIs with 3 integrated internal hex of implants were used and pedicled temporalis muscle flap was used for soft tissue coverage. The powder size was kept 30 microns with a layer thickness of 20-80 micrometer. Scanning speed was kept 4.5 meter/second with the laser power being 100 W. The transitional fillet radius of the implant was 1.5mm with “I style” fixation plate used. The implants were printed using Ti6Al4V titanium alloy and FEA analysis was used to calculate von Misses stress on the implant making sure that the maximum stress on the implant being less than the
allowable limit. GOM analysis was used for surface analysis and deviation making sure the maximum deviation being within the acceptable limit. The treatment algorithm presented here provides a predictable reconstruction, even after extended maxillary ablation, without time-consuming bone augmentation. 3D CAD-CAM technology has made it possible to plan virtual surgery together with implant designing enabling digital simulation and precise planning of surgery. Overall, it shortens operation time, speeds up the recovery and improves patient outcome [4,5].
At the time of surgery, cover screws were attached to prevent soft tissue ingrowth. After 6 weeks of surgery, the cover screws were replaced with gingival formers and subsequently with abutments. Impressions were made with polyvinyl siloxane impression material and a Porcelain fused to Metal (PFM) permanent prosthesis was planned achieving durability and aesthetic appeal. Occlusal adjustments were made, and speech quality was evaluated achieving patient satisfaction. This prosthetic concept restored masticatory function, markedly improved speech and improved the lost facial profile contour and lip support. Patient specific implants form the next frontier in maxillofacial reconstruction with numerous advantages like biomechanical prediction and prevention of failure through FEA analysis, reduced duration of surgery, improved quality of life and integrated dental rehabilitation [6,7]. However, the lack of standardisation and the complexity of the designing process has led to PSI’s not being accepted as a widespread prosthetic rehabilitation option in Maxillectomy defects [8].
Conclusion
Through this paper, we have addressed the lack of a standardised designing process of patient specific implants in the challenging reconstruction of a post mucormycosis maxillectomy defect. The reconstruction was done using a scientifically optimized protocol and stringent biomechanical and dimensional testing in the form of FEA and GOM analysis. The treatment algorithm presented in the paper provides predictable reconstruction without time-consuming bone augmentation with the help of 3D CAD-CAM technology. It has made possible to virtually plan surgery and implant designing thus enabling digital simulation and execution leading to shortening of operating time and improving patient outcome.
References
1. Andrades P, Militsakh O, Hanasono MM, Rieger J, Rosenthal EL. Current Strategies in Reconstruction of Maxillectomy Defects. Arch Otolaryngol Head Neck Surg (2011) 137:806–12.
2. Jehn P, Spalthoff S, Korn P, Stoetzer M, Gercken M, Gellrich N-C, et al.Oral Health-Related Quality of Life in Tumour Patients Treated With Patient-Specific Dental Implants. Int J Oral Maxillofac Surg (2020) 49:1067–72.
3. U V, Mehrotra D, Howlader D, Singh PK, Gupta S. Patient Specific Three-Dimensional Implant for Reconstruction of Complex Mandibular Defect. J Craniofac Surg. 2019 Jun;30(4):e308-e311.
4. Matros E, Albornoz CR, Rensberger M et al (2014) Computer assisted design and computerassisted modeling technique optimization and advantages over traditional methods of osseous flap reconstruction. ReconstrMicrosurg 30(5):289–296.
5. Darwich K, Ismail MB, Al-Mozaiek MYA, Alhelwani A. Reconstruction of mandible using a computer-designed 3D-printed patientspecific titanium implant: a case report. Oral Maxillofac Surg. 2021 Mar;25(1):103-111.
6. Chowdhury, Sanjay Kumar Roy, Karan Padha, Rahul Kumar, and Soumyajit Santra. "Three patient specific implant designs with integrated dental implant components for reconstruction of mandibulectomy defects." Advances in Oral and Maxillofacial Surgery 8 (2022): 100351.
7. Chowdhury, S.K.R., Padha, K., Kumar, R. et al. Scope of PSI in Maxillofacial Region: Our Experience. J. Maxillofac. Oral Surg. 22 (Suppl 1), 124–132 (2023).
8. Sanjay Kumar Roy Chowdhury, Karan Padha, Sneha Singh, Pradeep Yadav, Ravi Prajapati. The ideal patient specific implant. Part II: An eight step checklist for maxillary class I, II Brown defects, Journal of Oral Biology and Craniofacial Research, Volume 13, Issue 5, 2023, Pages 604-609.