Apical Ballooning Syndrome or Takotsubo Syndrome: A Case Report
Apical Ballooning Syndrome or Takotsubo Syndrome: A Case Report
Aravind-Kumar Radhakrishnan 1 2 3, Otar Kvavadze 1, Gaioz Tsetskhladze 1, Vazha Chelidze 1,
Anzor Makharadze 1, Kati jamburidze 1, Erekle Turabelidze 1, Giorgi Gafrindashvili 1,
Natia Khubua 1, Zurab Leladze 1, Zviad Kipiani 1
1.Jerarsi Clinic, Tbilisi, Georgia.
2.Charité University Medicine, Charité Campus Virchow, Berlin, Germany.
3.SCIRENT Clinical Research and Science, Berlin Germany.
*Correspondence to: Dr. Aravind-Kumar Radhakrishnan M.D, Jerarsi Clinic, Tbilisi, Georgia, Charité University Medicine, Charité Campus Virchow, SCIRENT Clinical Research and Science, Berlin Germany.
Copyright
© 2024 Dr. Aravind-Kumar Radhakrishnan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2024
Published: 29 March 2024
Abstract
Takotsubo syndrome or an apical ballooning syndrome is a rare, nonischemic, heart condition which usually mimics acute myocardial infarction, which is characterized by similar clinical, ECG changes and elevation of troponins. Echocardiography shows transient wall motion abnormality occurring usually at the apical segment of the heart, still now it is misdiagnosed in many primary hospitals. However, coronary angiography report shows the absence of obstructed coronary atherosclerosis or acute plaque rupture. We describe a case report of a patient who developed Takotsubo cardiomyopathy in the post-operative period following Rhinoseptoplasty.
Keywords: Takotsubo Cardiomyopathy, Apical ballooning syndrome, Stress cardiomyopathy, Acute coronary syndrome.
Apical Ballooning Syndrome or Takotsubo Syndrome: A Case Report
Background
Takotsubo Cardiomyopathy (TC), first discussed in Japan in 1990s, The term takotsubo is a Japanese name for an octopus trap. Due to the shape that is similar to the systolic apical ballooning appearance of the left ventricle. According to the statistical results, TTS is estimated to account for approximately 1–3% of all patients with suspected acute coronary syndrome and the incidence of TS has been increasing worldwide. Often triggered by severe physical or emotional stress and its predominantly affects post- menopausal women, however males end up having more cardiac complications
Case Presentation
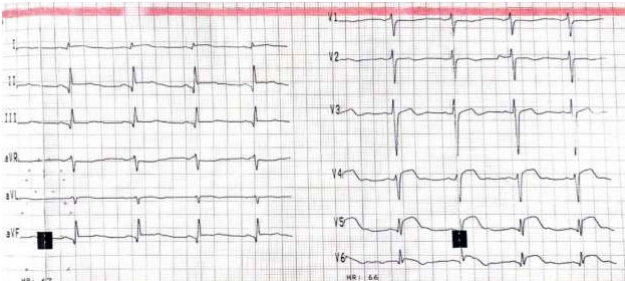
A 39-year-old female with chest pain arrived at the emergency department, H/o no HTN, no DM, not a Smoker, no Family H/o Cardiac disease, Rhinoseptoplasty was performed 3 weeks ago, An electro cardiogram (ECG) was performed Figure 1, which shows ST Segment elevation in pre-cordial leads from V4 to V6 and ST Segment elevation in II, III & aVF. Transthoracic echocardiography (TTE) revealed Global systolic function of the ventricle decreased EF - 40% shows transient wall motion abnormality in apex, septum apical, anterior-lateral, apical segments of the wall Hypo-akinesia Figure 2.
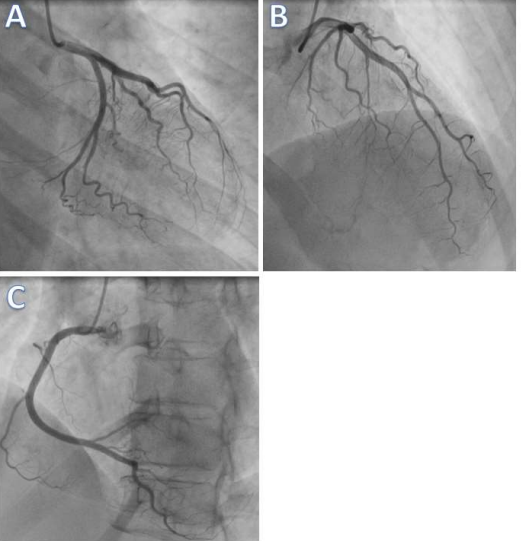
The subsequent Serum Troponin levels of the patient were done and its sharply increased to 22827 ng/mL, Immediately the patient was shifted to catheterization procedure room However, coronary angiography report shows the absence of obstructed coronary atherosclerosis or acute plaque rupture Figure 3, A B C.
Figure 1. Dynamic ECG changes at the beginning of the onset
Figure 2 Echocardiography Image Apical Hypokinesis
Figure 3 Coronary angiography showed no significant stenosis of the coronary arteries (left coronary artery [A,B] and right coronary artery [C]).
Discussion
Takotsubo Cardiomyopathy (TC), first discussed in Japan in 1990s, The term takotsubo is a Japanese name for an octopus trap. Due to the shape that is similar to the systolic apical ballooning appearance of the left ventricle. The incidence of TS has been increasing worldwide. The diagnosis of apical ballooning syndrome is based on the clinical presentation and differential diagnosis should always include acute coronary syndromes.
Transthoracic echocardiography provides a quick method of diagnosing wall motion abnormalities typically seen in apical ballooning syndrome, specifically hypokinesis or akinesis of the midsegment and apical segment of the left ventricle Figure 2.
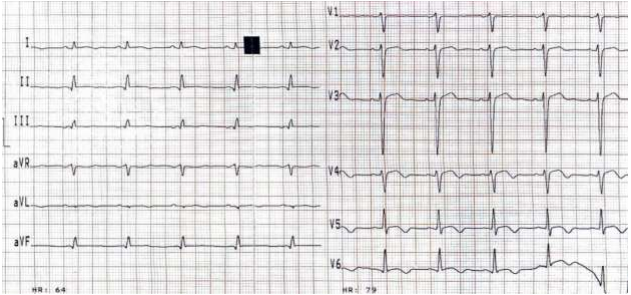
ECG recording after 5 days’ hospitalization showing resolution of ST segment elevation to inverted T waves in precordial leads Figure 4.
It is important to maintain the airway, breathing, and circulation; establishing intravenous access, providing supplemental oxygen and initiating cardiac monitoring should take priority. Since the initial presentation of takotsubo cardiomyopathy is similar to an acute coronary syndrome, the initial protocol of treatment involves aspirin, beta-blockers, ACE inhibitors, lipid-lowering agents, once diagnosed we can start beta-blockers and ACE inhibitors for a short period of around 3 to 6 months with regular series of Echo imaging of the wall movement and to check ventricular Ejection fraction to determine progression or improvement
So Close follow-up care is very essential to ensure the prognosis with series of Echocardiography and annual checkup is advised since the history of the disease is not clear and moreover The recurrence rate varies but is estimated at 3%.
Figure 4: ECG recording after 5 days hospitalization showing resolution of ST segment elevation to inverted T waves in precordial leads.
Conclusion
Since Takotsubo syndrome heart condition resembling that of an acute coronary syndrome, All physicians and health care worker in Emergency department should be aware of Takotsubo syndrome with differentiate diagnose to approach the patient quickly with proper care and treatment.
Awareness of the existence of this syndrome which often triggered by severe physical or emotional stress and easier access to early echocardiography and coronary angiography will help us to diagnose the Takotsubo syndrome or an apical ballooning syndrome.
Reference
1. Sansen V, Holvoet G. Takotsubo cardiomyopathy presenting as multivessel coronary spasm syndrome: case report and review of the literature. Acta Cardiol. 2007 Oct;62(5):507-11. doi: 10.2143/AC.62.5.2023415. PMID: 17982973.
2. Dias A, Núñez Gil IJ, Santoro F, Madias JE, Pelliccia F, Brunetti ND, Salmoirago-Blotcher E, Sharkey SW, Eitel I, Akashi YJ, El-Battrawy I, Franco E, Akin I, Jaguszewski M, Dawson D, Figueredo VM, Napp LC, Christensen TE, Hebert K, Ben-Dor I, Ozaki Y, García-Garcia HM, Kajita AH, Akasaka T, Kurisu S, Lerman A, Waksman R. Takotsubo syndrome: State-of-the-art review by an expert panel - Part 1. Cardiovasc Revasc Med. 2019 Jan;20(1):70-79. doi: 10.1016/j.carrev.2018.11.015. Epub 2018 Nov 17. PMID: 30528096.
4. Baltzer Nielsen S, Stanislaus S, Saunamäki K, Grøndahl C, Banner J, Jørgensen MB. Can acute stress be fatal? A systematic cross-disciplinary review. Stress. 2019 May;22(3):286-294.
5. Nandal S, Castles A, Asrar Ul Haq M, van Gaal W. Takotsubo cardiomyopathy triggered by status epilepticus: case report and literature review. BMJ Case Rep. 2019 Jan 29;12(1) [PMC free article]
6. Awad HH, McNeal AR, Goyal H. Reverse Takotsubo cardiomyopathy: a comprehensive review. Ann Transl Med. 2018 Dec;6(23):460. [PMC free article]
7. Zhang L, Piña IL. Stress-Induced Cardiomyopathy. Heart Fail Clin. 2019 Jan;15(1):41-53.
8. Khalid N, Iqbal I, Coram R, Raza T, Fahsah I, Ikram S. Thrombolysis In Myocardial Infarction Frame Count in Takotsubo Cardiomyopathy. Int J Cardiol. 2015 Jul 15;191:107-8.
9. Khalid N, Ahmad SA, Shlofmitz E, Umer A, Chhabra L. Sex disparities and microvascular dysfunction. Int J Cardiol. 2019 May 01;282:16.
10. Khalid N, Ahmad SA, Shlofmitz E, Chhabra L. Racial and gender disparities among patients with Takotsubo syndrome. Clin Cardiol. 2019 Jan;42(1):19. [PMC free article]
11. Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, Schunkert H, Radke PW. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest. 2007 Sep;132(3):809-16.
12. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006 Jul;27(13):1523-9.
13. Prasad A, Dangas G, Srinivasan M, Yu J, Gersh BJ, Mehran R, Stone GW. Incidence and angiographic characteristics of patients with apical ballooning syndrome (takotsubo/stress cardiomyopathy) in the HORIZONS-AMI trial: an analysis from a multicenter, international study of ST-elevation myocardial infarction. Catheter Cardiovasc Interv. 2014 Feb 15;83(3):343-8.