The Management of Isthomcele
The Management of Isthomcele
Rania Dahab *
*Correspondence to: Rania Dahab, Quttainah Medical Center (Department of Reproductive Medicine and Infertility) Kuwait.
Copyright
© 2024 Rania Dahab. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 January 2024
Published: 24 January 2024
The Management of Isthomcele
Introduction
Uterine niche, also known as uterine isthmocele, caesarean scar defect, and diverticulum, is an emerging complications of caesarean sections due to defective tissue healing. It occurs in up to 70% of women with previous caesareans, with 30% being symptomatic. Diagnosis is made radiologically by transvaginal sonography, saline instillation sonohysterography, or magnetic resonance imaging. The niche is located in the upper 2/3 cervix and isthmus, with 85% done electively or early labor, and lower 1/3 cervix, done at advanced dilatation with short cervix.
Prevalence varies between 24-70% with transvaginal sonography (TVS) and 56-84% with gel/saline instillation sonohysterography (SHG). However, this may be underestimated due to many women being asymptomatic and clinicians not recognizing niche as a cause of symptoms due to unawareness. A prospective observational study reported a prevalence of 45.6%, increasing with the number of previous caesareans.
Potential risk factors for uterine niche include poor healing of the caesarean scar, cervical dilatation of > 5 cm, > 5 hours duration of labor, and advanced foetal station. Lower uterine incision towards the cervix results in poor healing, as mucus secreted by cervical glands interferes with myometrial approximation. Caesarean done in advanced labor after cervical effacement and creation of uterovesical fold of peritoneum also influence the level of uterine incision.
Table 1 predisposing factors for cesarean scar defect
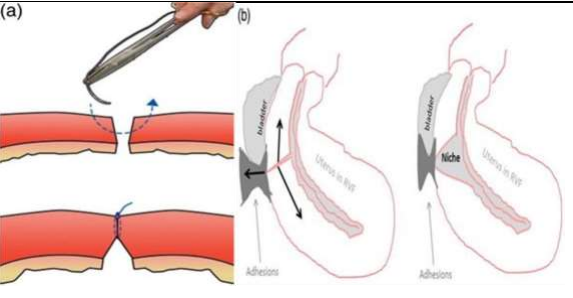
Isthmocoele formation can be attributed to various factors, including incision through cervical tissue, incomplete closure of the CS wound, early adhesion formation, meticulous hemostasis, impaired wound healing, and genetic factors. These theories help prevent bladder flap, bladder flap, and devascularization, while ensuring proper closure and avoiding infection and devascularization.
Figure 1a, 1b
Uterine closure techniques can impact the risk of niche formation. Single-layer, decidua sparing closures can lead to incomplete closure, with almost 95% of patients with niches having single-layer closure without closing the peritoneum. A strong myometrial scar with proper anatomical approximation minimizes the risk of niches. Double-layer uterine closure using non-locking sutures is the optimal closure technique, resulting in thicker residual myometrium and potentially lower risk of niche formation. Suboptimal surgical techniques, such as inadequate haemostasis, tissue ischemia, devascularization, and excessive tissue manipulation, contribute to poor scar healing and adhesions, resulting in niche formation. Adhesion formation with the abdominal wall and retroflexed uterus also increase counteracting forces, leading to large niches. Patient factors such as genetic predisposition, gestational diabetes, previous caesarean, advanced body mass index, and longer active labor prior to emergency caesarean also increase the risk. However, there is no difference between elective and emergency caesarean.
Clinical Presentation
Post-caesarean niche is a condition where the anterior edge of the niche obstructs the flow of menstrual blood, leading to post-menstrual spotting and brownish discharge after the end of menstruation. This symptom is most prevalent in women aged 6-12 months post-caesarean, with 20% experiencing post-menstrual spotting in women with isthmocele compared to 8.3% without isthmocele. Prolonged bleeding is another symptom, with impaired menstrual drainage resulting in prolonged flow. Intermittent spotting occurs due to in situ blood formation in the niche, resulting in intermenstrual spotting. Pain in women with niche may include dysmenorrhea, chronic pelvic pain, dyspareunia, or suprapubic pain. Midcycle intrauterine fluid accumulation may occur due to excess mucus formation by retained blood in approximately 45% of women.
Caesarean scar ectopic pregnancy may implant in the niche, increasing the risk of rupture. Secondary infertility may be due to chronic inflammation or peri-ovulatory fluid accumulation interfering with sperm penetration, fertilization, and implantation. Obstetric complications in future pregnancy include increased risk of scar ectopic, placenta accrete, scar dehiscence, and uterine rupture. Scar abscess, though rare, has been reported up to 6 years after caesarean, due to residual blood and infected mucus.
Diagnosis
Niches can be visualized in non-pregnant states using various imaging techniques such as TVS, SHG, 3-D ultrasound, magnetic resonance imaging, or hysteroscopy. Diagnosis is based on an anechoic space at least 1 mm deep, with or without fluid, and at least 2 mm deep in the myometrium at the caesarean scar site. There is no consensus on diagnostic criteria, but features like residual myometrial thickness (RMT) and niche size are noted. Large niches are defined when RMT is less than 50% of adjacent myometrium, with a cut-off of 3 mm. A total defect is defined without residual myometrium.
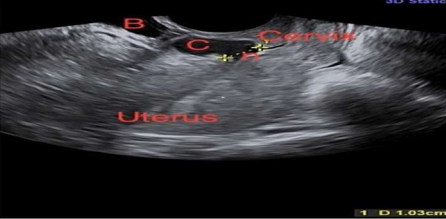
Figure 2 2-D ultrasound showing uterus, cervix, niche (n) measuring 1 cm, collection in the niche (C) and bladder (B) (courtesy Prof. Vatsla Dadhwal)
The uterine niche is a condition where the scar is positioned in the uterus, causing a bulging or retracted area. It can also be seen as an inward protrusion, outward protrusion, or inward retraction. Other niche features include concavity, abnormal vascularity, visible serosa, cyst- or polyp-like structure. Surface hemorrhage (SHG) is more accurate for diagnosing niches, with higher prevalence, identification of larger niches, and thinner residual myometrium. SHG is the investigation of choice, especially at 6-12 weeks post-partum when the scar is incompletely healed. Treatment is indicated for symptomatic women with secondary infertility, previous scar ectopic, recurrent miscarriage, AUB, and post-menstrual spotting. However, the efficacy of treatment is yet to be ascertained, and routine repair of the incidentally diagnosed niche without future childbearing plans is not recommended.
Treatment options for a uterine niche are as follows: Medical Treatment
Hormonal therapy relieves AUB symptomatically, while oral contraceptives are suitable for non-pregnant women. LNGIUS does not decrease menstrual length.
Uterine Sparing Surgical Treatment
Conservative surgical interventions should be considered after eliminating other causes of presenting symptoms. Options include resection by hysteroscopic route or excision plus repair by transabdominal (laparotomy, laparoscopic, robotic) or vaginal route. Hysteroscopic niche resection involves resection of only distal rim, or both distal and proximal edges with a resectoscope using bipolar or unipolar current, and coagulation of fragile vessels at the base or entire niche with a ball electrode. Resection facilitates drainage of menstrual blood but increases niche size.
Complications of hysteroscopic niche resection include uterine perforation, bladder injury, cervical incompetence with proximal rim resection, and uterine rupture in subsequent pregnancies. Bladder safety can be ensured by intraoperative ultrasound guidance and filling bladder with methylene blue.
Niche repair is the preferred method when RMT is < 3 mm and essentially involves identification of defect, excision of fibrotic tissue from the edges, and re-approximation in two layers. Simultaneous hysteroscopy, Hegar’s dilator, intracervical foley’s catheter, transvaginal or transrectal ultrasound can aid identification. Vervoort’s technique involves laparoscopic repair combined with hysteroscopy with round ligament plication in extremely retroflexed uterus, using hyaluronic acid as adhesion barrier.
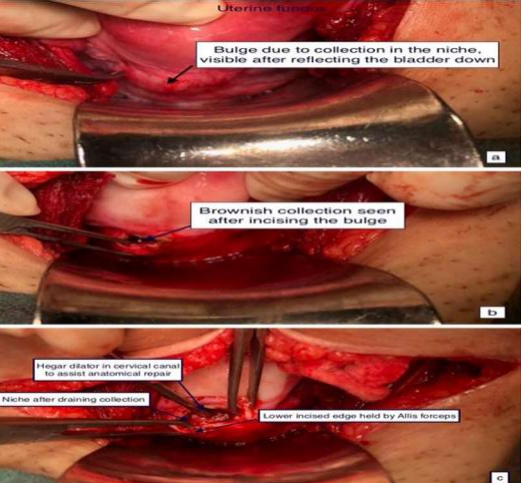
Transabdominal route is preferred for large defects, especially if residual myometrium is < 3 mm, as bladder can be mobilized out of the surgical field offering better niche visualization with lesser bladder injury. It is a better approach for women desiring future pregnancy since uterine wall thickness and strength increase. Among transabdominal routes, laparoscopy and robotic surgery offer advantages of being minimally invasive with lesser morbidity.
Figure 3 Intraoperative findings of transabdominal repair a bulge prior to incision, b after incision over niche, c after excision of fibrotic tissue from the niche edges (courtesy Prof. Vatsla Dadhwal)
Hysterectomy is a surgical procedure that provides definitive treatment for niche-related gynecological symptoms.
Outcomes of Surgical Management of Post?caesarean Niche
Hysteroscopic niche resection can significantly reduce post-menstrual spotting and pain in 72.4% of cases, with complete resolution in 97% of cases. AUB can be cured in 87.5% of patients within the first month and 96.8% in the second month after surgery. However, up to 5% of patients may experience recurrence. A study by Vervoort found that 79% of women with large niches and < 3 mm RMT treated laparoscopically experienced symptom relief, post-menstrual spotting reduced by 7 days at 6 months, dysmenorrhea reduced, and myometrial thickness increased. Interestingly, after laparoscopic repair, 93% of patients reported symptom-free status, an increase in mean myometrial thickness, and a 44% pregnancy rate in infertile women.
Pregnancy rates varied from 22-71% in various studies. In a retrospective study, isthmocele was identified as the primary cause of infertility in 45.7% of patients, with all 16 women relieved of AUB and pain, and 9/16 (56.3%) conceived after hysteroscopic isthmoplasty. However, women who failed to conceive had higher BMI, higher isthmocele grade, higher number of prior caesareans, and advanced age.
Prevention of niche formation involves primary prevention by minimizing caesarean rates and secondary prevention by adopting correct surgical techniques. A recent study showed that uterine closure using a double-layer unlocked technique may help reduce isthmocele formation and ensure sufficient residual myometrium.
Conclusion
Post-caesarean uterine niche is a new clinical entity with high suspicion rates. It requires careful selection for surgical correction, a possible learning curve, and yet to be proven efficacy. Hormonal treatment is preferred for bleeding symptoms, while subfertility may require surgical correction. Hysteroscopic resection is preferred for smaller niches, transvaginally for lower niches, and transabdominal for large defects and future pregnancy. Laparoscopy and robotic surgery offer minimal invasiveness and lower morbidity. Future studies may explore factors influencing treatment preferences and success.
References
1. Tulandi et al. Emerging Manifestations of Cesarean Scar Defect in Reproductive-aged Women. Journal of Minimally Invasive Gynecology, Vol 23, No 6, September/October 2016 . http://dx.doi.org/10.1016/j.jmig.2016.06.020
2. Donnez et al. Gynecological and obstetrical outcomes after laparoscopic repair of a cesarean scar defect in a series of 38 women. Fert Ster 2016. http://dx.doi.org/10.1016/j.fertnstert.2016.09.033
3. Brook AJ, Clarke FR, Bhatia K. Gynaecological morbidity associated with caesarean niche: increasing awareness, prevention and management. The Obstetrician & Gynaecologist 2020;22:122–30. https://doi.org/10.1111/tog.12642
4. Jordans IPM et al. Sonographic examination of uterine niche in non-pregnant women: a modified Delphi procedure. Ultrasound Obstet Gynecol 2019; 53: 107–115
5. Vervort et al. The HysNiche trial: hysteroscopic resection of uterine caesarean scar defect (niche) in patients with abnormal bleeding, a randomised controlled trial. BMC Women's Health (2015) 15:103 DOI 10.1186/s12905-015-0260-8
6. SipahiS et al. The minimally invasive approach to the symptomatic isthmocele
– what does the literature say? A step-by-step primer on laparoscopic isthmocele – excision and repair. Curr Opin Obstet Gynecol 2017, 29:000 – 000 DOI:10.1097/GCO.0000000000000380
7. Vervoort et al. Why do niches develop in Caesarean uterine scars? Hypotheses on the aetiology of niche development. Human Reproduction, Vol.30, No.12 pp. 2695–2702, 2015
8. Mashiach R, Burke YZ. Optimal Isthmocele Management: Hysteroscopic, Laparoscopic, or Combination. J Minim Invasive Gynecol. 2021 Mar;28(3):565-574. doi: 10.1016/j.jmig.2020.10.026. Epub 2020 Nov 2. PMID: 33152531.
9. Iannone P, Nencini G, Bonaccorsi G, et al. Isthmocele: from risk factors to management. Rev Bras Ginecol Obstet. 2019;41(1):44–52.
10. Kulshrestha V, Agarwal N, Kachhawa G. Post-caesarean Niche (Isthmocele) in Uterine Scar: An Update. J Obstet Gynaecol India. 2020 Dec;70(6):440-446. doi: 10.1007/s13224-020-01370-0. Epub 2020 Sep 21. PMID: 33417629; PMCID: PMC7758379.
11. Antila-Långsjö RM, Mäenpää JU, Huhtala HS, et al. Cesarean scar defect: a prospective study on risk factors. Am J Obstet Gynecol. 2018;219(5):458.e1–.e8.
12. Bij de Vaate AJ, van der Voet LF, Naji O, et al. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: systematic review. Ultrasound Obstet Gynecol. 2014;43(4):372–82.
13. Vervoort AJ, Uittenbogaard LB, Hehenkamp WJ, et al. Why do niches develop in Caesarean uterine scars? Hypotheses on the aetiology of niche development. Hum Reprod. 2015;30(12):2695–702.
14. Vervoort AJ, Van der Voet LF, Witmer M, et al. The HysNiche trial: hysteroscopic resection of uterine caesarean scar defect (niche) in patients with abnormal bleeding, a randomised controlled trial. BMC Womens Health. 2015;15:103. https ://doi. org/10.1186/s1290 5-015-0260-8.
15. Antila-Långsjö RM, Mäenpää JU, Huhtala HS, et al. Cesarean scar defect: a prospective study on risk factors. Am J Obstet Gynecol. 2018;219(5):458.e1–.e8
16. Vervoort A, Vissers J, Hehenkamp W, et al. The effect of laparoscopic resection of large niches in the uterine caesarean scar on symptoms, ultrasound findings and quality of life: a prospective cohort study. BJOG. 2018;125(3):317–25.
17. Zhang X, Yang M, Wang Q, et al. Prospective evaluation of five methods used to treat cesarean scar defects. Int J Gynaecol Obstet. 2016;134(3):336–9. https ://doi.org/10.1016/j.ijgo.2016.04.011.
18. Nirgianakis K, Oehler R, Mueller M. The Rendez-vous technique for treatment of caesarean scar defects: a novel combined endoscopic approach. Surg Endosc. 2016;30(2):770–1.
19. Donnez O, Donnez J, Orellana R, Dolmans MM. Gynecological and obstetrical outcomes after laparoscopic repair of a cesarean scar defect in a series of 38 women. Fertil Steril. 2017;107(1):289–96.