A Rare Case of Nodular Fasciitis Over the Wrist Dorsum
A Rare Case of Nodular Fasciitis Over the Wrist Dorsum
Dr Kassem El Houcheimi *
*Correspondence to: Dr Kassem El Houcheimi. FACS, MBA Orthopedic surgeon, Clemenceau Medical Center Dubai.
Copyright
© 2022 Dr Kassem El Houcheimi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 February 2022
Published: 01 March 2022
Abstract
Introduction: Nodular fascitis is a benign, reactive fibroblastic tumor that usually presents as a rapidly growing lesion with occasional involvement of the deep fascia and muscle We present a case of nodular fascitis over the dorsum of the wrist. In our knowledge, this is the first reported case of nodular fascitis at this location in literature.
Case Presentation: A 33 year old male with a desk job, presented with a rapidly growing lesion over the dorsum of left wrist over 5 months, associated with pain and restriction of dorsiflexion of wrist. The Xray, ultrasound and MRI images were inconclusve and excisional biopsy was done for definitive diagnosis.
Conclusion: Nodular fascitis is a relatively uncommon but important differential diagnosis for any rapid soft tissue growth. It is a self limiting proliferative fibroblastic lesion, with excisional biopsy as the gold standard for diagnosis of this condition.
Keywords: Nodular fascitis, dorsum of wrist, excisional biopsy.
A Rare Case of Nodular Fasciitis Over the Wrist Dorsum
Introduction
Nodular fasciitis is a rare, proliferative fibroblastic lesion that can be misdiagnosed as a soft tissue sarcoma (1). It typically develops in the subcutaneous fascia of the extremities and trunk, and sometimes in the superficial portions of the deep fascia of the underlying muscle sheath. This case report describes the clinical presentation, diagnostic work up, surgical in-tervention, and postoperative course of a rare case of nodular fasciitis over the dorsum of the wrist, marking the first documented case report of this lesion (2).
Case Report
A 33-year-old engineer with a desk job reported persistent left wrist pain with stiffness and movement restriction for the last five months. The pain was accompanied by swelling in the wrist's dorsum, which had progressively increased over time. The mass was firm, 2.5 cm in diameter, firmly anchored to the wrist's dorsum and immobile. The wrist's dorsiflexion was restricted to 10 degrees due to the mass effect, but no apparent tendon adhesion was noted. The patient had no prior history of injury or trauma.
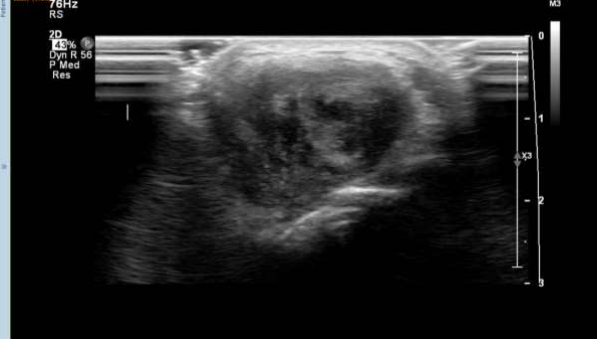
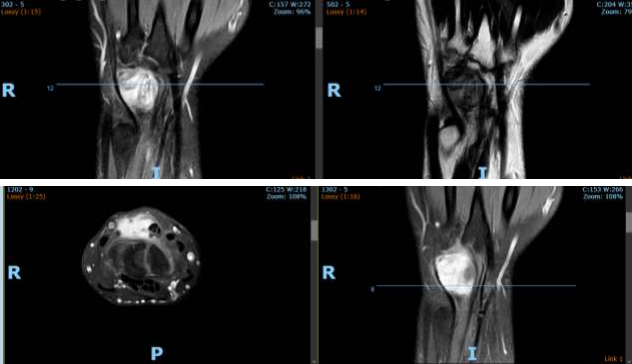
The patient had a solid hypoechoic lobulated mass lesion measuring 27x16mm on the dorsal aspect of his left wrist. The diagnosis was a giant cell tumor and soft tissue sarcoma, and fur-ther investigations were advised. X-rays showed a soft tissue shadow in the lateral view, but no bony abnormalities were noted. MRI scans revealed an irregular, intensely enhancing soft tissue mass at the wrist's dorsal aspect, interposed between the 4th and 5th extensor tendon compartments. The MRI findings were consistent with a benign soft tissue neoplasm.
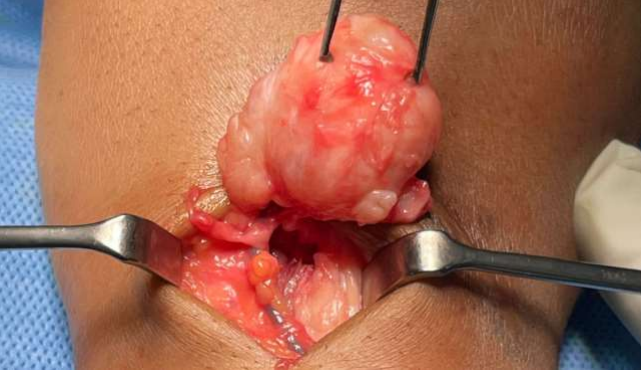
To obtain a definitive diagnosis, an excisional biopsy was performed under general anesthe-sia, revealing a 3x3 cm non cystic hard soft tissue mass attached to the dorsal joint capsule. The lesion was well circumscribed, and the encapsulated lesion was completely excisiond. The adjacent tendons and vessels were taken care of to avoid damage.
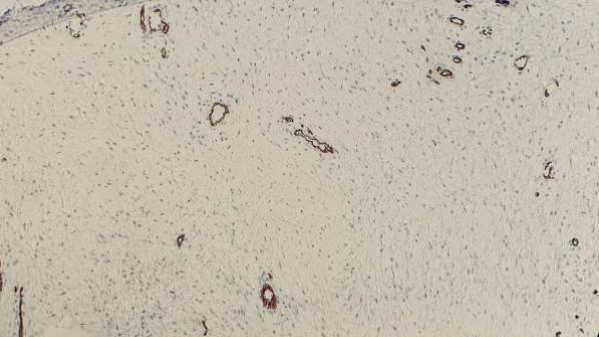
Histopathology findings showed a well-circscribed neoplasm composed of interlacing and intersecting fascicles of bland smooth muscle cells. Few thick-walled blood vessels were visible, and mitoses were absent. No evidence of atypia or malignancy was found in the sec-tions studied.
The patient had an uneventful post-operative recovery, with complete recovery of range of motion and wrist function without complications. There was no recurrence until a year of follow-up.
Figures 1,2,3,4,5,6
Discussion
Nodular fasciitis is a rare, benign reactive lesion that rapidly grows in young adults between 20 and 40 years old. It is usually subcutaneous, with occasional cases involving muscle and fascia. The macroscopic appearance of nodular fasciitis is well-circscribed single masses, usually measuring less than 2 cm in diameter. The rapid growth of the lesion often makes biopsy essential to rule out sarcoma. The aetiology of nodular fasciitis remains unclear, with 38.5% of cases in hand and wrist having a history of trauma (3,4,5,6).
The features of nodular fasciitis on ultrasound and magnetic resonance imaging (MRI) are non-specific, with the lesions appearing as well-circscribed, round to oval masses. Signal intensity of the condition is variable, with intramuscular lesions appearing mildly inhomo-geneous and hyper intense to skeletal muscle on T1-weighted spin-echo images, and subcu-taneous lesions being markedly hypo intense to skeletal muscle on all spin-echo sequences and appearing homogeneous in texture. High cellularity and micro-vessel density may di-rectly influence the early enhancement after intravenous gadolinium injection and compact cellularity with a prominent capillary network. A myxoid pattern may be responsible for the enhancement on MRI (7,8).
Historopathology of nodular fasciitis suggests regular spindle-shaped fibroblasts or myofi-broblasts lacking nuclear hyper chromatic and pleomorphism with high cellularity. Spindle-shaped fibroblasts, clefts separating the fibroblasts, extravasated erythrocytes, interstitial mucoid material, and a loosely textured 'feathery' pattern of the mucopolysaccharide ground substance are diagnostic of nodular fasciitis (9, 10). Immunostains of Desmin, cytokeratin, and S-100 are typically negative. In view of the inconclusiveness of imaging for diagnosis, biopsy is often the gold standard (11,12).
Conclusion
Nodular fasciitis of the wrist is a rare and inconclusive condition, with a prognosis of excel-lent with low recurrence risk. It is important to differentiate it from non-cystic soft tissue mass, as clinical and radiological findings are inconclusive. This differential diagnosis helps avoid anxiety and overtreatment associated with malignancy, ensuring a more accurate di-agnosis.
Reference
1.Konwaler, 8. E., Keasbey, L. & Kaplan, L.: Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Alii. l. Clill. Pathol. 1955: 25: 241-252
2.Yamane, Hideki, Tanaka, Yoichi, Shimono, Masaki, Yamamura, Takeo, Takano, Nobuo, Saito, Chikara, Takahashi, Shojiro Nodular fascitis of the mandible in a child International Journal of Oral & Maxillofacial Surgery1986 Vol. 15; Iss. 4 499-502
3.Bernstein KE, Lattes R. Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: clinicopathologic study of 134 cases. Cancer. 1982;49:1668–78.
4. Rankin G, Kuschner SH, Gellman H. Nodular fasciitis: a rapidly growing tumor of the hand. J Hand Surg Am. 1991;16A:791–5.
5.Shimizu S, Hashimoto H, Enjoji M. Nodular fasciitis: an analysis of 250 patients. Pathology. 1984;16:161–6.
6.Kijima H, Okada K, Ito H, Shimada Y, Nanjo H, Itoi E. Nodular fasciitis of the finger. Skeletal Radiol. 2005;34:121–3.
7.Nodular fasciitis of the hand in a young athlete. A case report Hitomi Hara, Ikuo Fujita, Takuya Fujimoto, Keisuke Hanioka, Toshihiro Akisue, and Masahiro Kurosaka Ups J Med Sci. 2010 Oct; 115(4): 291–296.
8.Katz MA, Beredjiklian PK, Wirganowicz PZ. Nodular fasciitis of the hand. Clin Orthop Relat Res. 2001;382:108–11.
9.Frei S, de Lange EE, Fechner RE. Case report 690. Nodular fasciitis of the elbow. Skeletal Radiol. 1991;20:468–71.
10.Hymas DC, Mamalis N, Pratt DV, Scott MH, Anderson RL, Langer PD. Nodular fasciitis of the lower eyelid in a pediatric patient. Ophthal Plast Reconstr Surg. 1999;15:139–42.
11.Leung LY, Shu SJ, Chan AC, Chan MK, Chan CH. Nodular fasciitis: MRI appearance and literature review. Skeletal Radiol. 2002;31:9–13.
12. Meyer CA, Kransdorf MJ, Jelinek JS, Moser RP., Jr MR and CT appearance of nodular fasciitis. J Comput Assist Tomogr. 1991;15:276–9.