Implantation of Intrastromal Corneal Ring Segments Plus Cataract Surgery in a Patient with Penetrating Keratoplasty for Advanced Keratoconus
Implantation of Intrastromal Corneal Ring Segments Plus Cataract Surgery in a Patient with Penetrating Keratoplasty for Advanced Keratoconus
Fermín Silva M. D1, Claudia E. Sotomayor M.D 1, Ana Luisa González M.D.*1, Robinson Barrientos M.D.1
1.Department of Ophthalmology, Research Department Clínica La Luz, Lima-Perú, Av. Arequipa 1148.
*Correspondence to: Ana Luisa González Méndez. Department of Ophthalmology, Research Department Clínica La Luz, Lima-Peru, Av. Arequipa 1148, Lima, Peru.
Copyright
© 2024 Ana Luisa González Méndez. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 March 2024
Published: 01 April 2024
DOI:https://doi.org/10.5281/zenodo.11097279
Abstract
Introduction: According to the knowledge of the authors, this is the first case informed at La Clínica La Luz, Lima-Peru in a patient with penetrating keratoplasty and high astigmatism managed with intrastromal corneal ring segments further cataract surgery.
Patient and Clinical Findings: Female patient 34- year - old female with a history of penetrating keratoplasty, to whom a intrastromal corneal ring segments was performed further cataract surgery.
Diagnosis, Intervention and Outcomes: After intrastromal corneal ring segments implantation, astigmatism topographic reduced at 8 D and BCVA was Log MAR 0.8 (20/150). Two months after cataract surgery, astigmatism reduced to 5.27 D and AVCC: Log MAR 0.2 (20/30).
Conclusions: It is shown that implantation of rings with femtosecond about keratoplasty penetrating combined with cataract surgery, it is safe to reduce astigmatism and improve vision.
Implantation of Intrastromal Corneal Ring Segments Plus Cataract Surgery in a Patient with Penetrating Keratoplasty for Advanced Keratoconus
Introduction
Keratoconus is a bilateral and asymmetric corneal ectasia that is characterized by progressive thinning of the cornea that produces decreased vision due to irregular astigmatism and progressive myopia. It was considered a non-inflammatory disease, although important alterations in inflammatory mediators have now been found. [1] It usually develops in the second and third decades of life, affecting all ethnic groups and both gender equally. Among the risk factors for developing it we find: family history of the disease, eye rubbing, ocular allergy, asthma and atopy [2].
Depending on the severity and progression of the disease, various treatments can be carried out, from the placement of rigid contact lenses, crosslinking (CXL) to increase biomechanical stability and rigidity of the cornea in cases of keratoconus progression, intrastromal corneal ring segments (ICRS) that they structurally stabilize ectasia and finally, for advanced cases, corneal transplantation: deep anterior lamellar keratoplasty (DALK) and penetrating keratoplasty (PK) [3].
It is estimated that a patient with keratoconus has a permanent risk of 10 to 20% of needing a corneal transplant [4]. Penetrating keratoplasty was the first technique to be established safely and with great success for the visual restoration of patients, although currently the most widely used is DALK. Regarding long-term complications, it was found that there is a higher incidence of cataracts in patients who underwent PK (19.2%) compared to DALK (8.3%). On the other hand, both surgeries have similar results in terms of BCVA, refraction, and topographic astigmatism [5].
Patient Consent
The patient reported in this report has provided written informed consent for their information to be released in a de-identified form.
Case Report
A 34-year-old female patient, Venezuelan nationality, housewife occupation who attends in Clínica La Luz. The case complies with the Declaration of Helsinki. The ethics committee and the institutional review board of Clínica La Luz approved the case report, obtaining the written informed consent of the patient.
The patient refers that she was diagnosed with advanced keratoconus, for which she underwent penetrating keratoplasty in her country of origin in 2013. Going for the first time in the cornea area at Clínica la luz, Lima - Peru in March 2021 due to decreased vision for a long time 2 years.
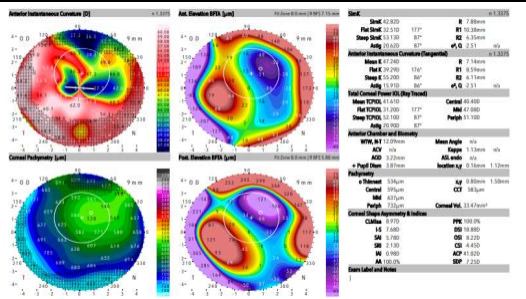
In the slit lamp ophthalmological examination, a transparent corneal button was observed with absence of sutures, the presence of a LOCS III NO2NC2P4 cataract, the rest of the anterior and posterior segment without alterations, intraocular pressure 13 mmHg. Uncorrected visual acuity (UCVA) of the right eye was finger counting (CD) at 30cm, corrected to LogMAR 2.1, and corrected visual acuity (UCVA) was 20/400, corrected to LogMAR 1.3. Its subjective refraction was: -7.00 -6.00 x 175°. Corneal topography was performed (Figure 1), with topographic values: Steep SimK: 53.13 D, astigmatism 20.62 D and IS 7.68 and specular microscopy with endothelial cell count 1425 cells/mm 2. It was decided to first perform intrastromal segment implant surgery with femtosecond to reduce topographic irregular astigmatism with 2 intrastromal segments of 160° x 250 um, the surgery was without complications.
Figure 1: Pre- ICRS implant corneal topography
On biomicroscopy, a clear corneal button with 2 segments of rings centered on the pupil, 2 mm from incisions. On the 1st postoperative day, BCVA was 20/400, corrected to LogMAR 1.3, and BCVA 20/150, corrected to LogMAR 0.9.
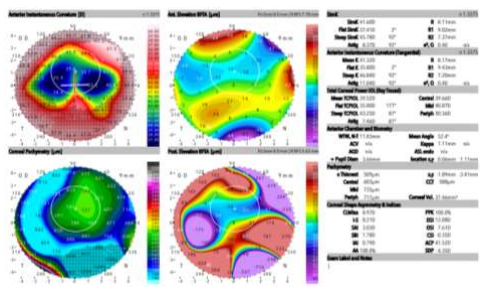
Two months after ring implantation, a new corneal topography was performed (Figure 2) with changes in topographic values: Kmax 45.78 D, astigmatism 8.37 D, IS 8.21 and it was decided to perform phacoemulsification surgery plus foldable hydrophobic IOL implantation with power + 16.5 D, without complications.
Figure 2: Post 2 month ICRS implant corneal topography
On evaluation day 1 of the cataract surgery postoperative period, the patient reported notable visual improvement, BCVA 20/150, corrected to LogMAR 0.9 and BCVA 20/80, corrected to LogMAR 0.6. On postoperative day 7, AVSC 20/80, corrected to LogMAR 0.6 and AVCC 20/50, corrected to LogMAR 0.4 with a refraction of +1.00 -4.00 x 170°. (Figure 3).
One month postoperatively AVSC 20/100, corrected to LogMAR 0.7 and AVCC 20/30, corrected to LogMAR 0.2 with a refraction of +1.00 -4.25 x 0°.
At one year of follow-up, BCVA 20/70 corrected to LogMAR 0.5 and BCVA remained at 20/30, corrected to LogMAR 0.2 with a refraction of +1.75 -3.50 x 175°. Topographic values were obtained: Steep simK 46.09 D, astigmatism 5.27 D, IS 6.13.
Figure 3: Photograph of the anterior segment 12 months postoperatively
Discussion
Residual and irregular astigmatism and postoperative refractive error associated with penetrating keratoplasty is a common condition, especially in patients undergoing it for advanced keratoconus. Likewise, it is considered a challenge for the anterior segment surgeon since it prevents satisfactory vision in this group of patients.
There are several ways to correct astigmatism such as the use of corrective or contact lenses, refractive surgery with excimer laser (LASIK or PRK), although due to high ametropia and decreased corneal thickness, this is not the first option, wedge resection of cornea, toric IOL implant, and intrastromal corneal ring segment implant. Coscarelli et all conclude that ICRS implantation is a promising treatment for post-PK astigmatism, especially in eyes with thin and irregular corneas [6].
Coskunseven et al consider the use of ICRS, a minimally invasive procedure, as a post-PK astigmatism correction method [7]. There are various advantages over other surgical techniques such as avoiding treatment with excimer laser since it generates scarring in the central cornea, which can generate an unsatisfactory result in post-PK corneas, in addition, ICRS implantation is a reversible technique in cases where the result is not is the right one for the patient, and lastly, it avoids the complications inherent to intraocular surgery.
Several studies confirm that the implantation of ICRS could be a good surgical option to correct severe astigmatism after PK and produces good results at a visual, refractive and topographic level.
In patients with keratoconus, it has been described that the use of the femtosecond laser to make the tunnel for the implantation of the ring is safer than the mechanical technique, since the latter brings with it possible complications such as epithelial defects, perforation, infectious keratitis , placement of superficial or asymmetric segments, stromal edema at the level of the incisions and extension of the incision towards the visual axis [8].
Coskunseven et al. evaluated the results and complications after one year of follow-up of patients who had intrastromal corneal ring segments implanted using femtosecond for tunnel creation, concluded that femtosecond-assisted intrastromal corneal ring segments implantation in most eyes with keratoconus improves BCVA and BCVA (improving more than six Snellen lines), reduces the patient's manifest refraction and corneal astigmatism (up to 4 D); refractive and topographic results are comparable with the results of creating tunnels mechanically. However, the use of the femtosecond helps make the procedure faster, easier and with greater precision in the depth of the implant [9].
Ramirez et. al evaluated the early keratometry and refractive results of patients with keratoconus operated on with ICRS and concluded that their placement significantly reduces keratometry, spherical equivalents, and astigmatism in patients with early keratoconus [10]. These same data can be extrapolated to patients who have undergone penetrating keratoplasty and then ICRS implantation.
On the other hand, the preoperative study for cataract surgery in patients with moderate to severe keratoconus presents greater challenges, mainly the calculation of the intraocular lens (IOL) since we know that these can have unpredictable results and a greater risk of hyperopic refraction after surgery . [11]. This is because the IOL calculation formulas are based on keratometric values and a precise and stable measurement is necessary to determine the correct IOL power. High keratometric values in advanced keratoconus will result in selection of a low power IOL or a negative power IOL and may lead to postoperative refractive surprises [12]. For this reason, we decided to place the ICRS in the corneal button with femtosecond prior to cataract surgery in order to decrease keratometric values and improve the accuracy of IOL calculations.
Femtosecond intrastromal corneal ring segments implantation in patients with penetrating keratoplasty for advanced keratoconus is a safe technique on the corneal button that guarantees improvement in keratometric values, especially effectively reducing the cylinder, improving visual acuity and quality. In addition to a better intraocular lens calculation for cataract surgery.
What was Known
- The use of ICRS for the correction of post-PK residual astigmatism is a minimally invasive and effective technique, it improves AVSC and AVCC and topographic values.
What this Paper Adds
- The implantation of ICRS with femtosecond after PK is a faster, easier technique, with greater precision in the depth of the ring and with less possibility of complications.
- The implantation of ICRS helps in the preoperative study by improving the keratometric levels to determine the correct power of the IOL.
References
1. Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: An updated review. Contact Lens Anterior Eye J Br Contact Lens Assoc. 2022;45(3):101559. doi:10.1016/j.clae .2021.101559
2. Woodward MA, Blachley TS, Stein JD. The Association Between Sociodemographic Factors, Common Systemic Diseases, and Keratoconus: An Analysis of a Nationwide Heath Care Claims Database. Ophthalmology . 2016;123(3):457-465.e2. doi:10.1016/j.ophtha .2015.10.035
3. Arnalich -Montiel F, Alió Del Barrio JL, Alió JL. Corneal surgery in keratoconus: which type, which technique, which outcomes? Eye Vis Lond Engl . 2016;3:2 . doi:10.1186/s40662-016-0033-y
4. Thanitcul C, Varadaraj V, Canner JK, Woreta FA, Soiberman US, Srikumaran D. Predictors of Receiving Keratoplasty for Keratoconus. Am J Ophthalmol . 2021;231:11-18 . doi:10.1016/j.ajo .2021.05.013
5. Khattak A, Nakhli FR, Al- Arfaj KM, Cheema AA. Comparison of outcomes and complications of deep anterior lamellar keratoplasty and penetrating keratoplasty performed in a large group of patients with keratoconus. Int Ophthalmol . 2018;38(3):985-992. doi:10.1007/s10792-017-0548-9
6. Coscarelli S, Ferrara G, Alfonso JF, et al. Intrastromal corneal ring segment implantation to correct astigmatism after penetrating keratoplasty. J Cataract Refract Surg. 2012;38(6):1006-1013. doi:10.1016/j.jcrs .2011.12.037
7. Coskunseven E, Kymionis GD, Talu H, et al. Intrastromal corneal ring segment implantation with the femtosecond laser in a post-keratoplasty patient with recurrent keratoconus. J Cataract Refract Surg. 2007;33(10):1808-1810. doi:10.1016/j.jcrs .2007.05.042
8. Follow us D, Ferrara P, Chatzinikolas K, Bessis N, Papastergiou G. Ferrara intrastromal corneal rings for the correction of keratoconus. J Cataract Refract Surg. 2002;28(11):1947-1951. doi:10.1016/s0886-3350(02)01495-5
9. Coskunseven E, Kymionis GD, Tsiklis NS, et al. One-year results of intrastromal corneal ring segment implantation ( KeraRing ) using femtosecond laser in patients with keratoconus. Am J Ophthalmol. 2008;145(5):775-779. doi:10.1016/j.ajo .2007.12.022
10. Ramírez M, Manzanillo C, Estrada A, et al. Early keratometric and refractive results after intra-corneal rings surgery in keratoconus patients. Cir Cir . 2022;90(S1):92-95. doi:10.24875/CIRU.22000018
11. Moshirfar M, Ziari M, Ronquillo YC. Cataract surgery considerations in patients with prior history of keratoconus and ectasia. Curry opinion Ophthalmol . 2023;34(1):41-47. doi:10.1097/ICU.0000000000000908
12. Bozorg S, Pineda R. Cataract and keratoconus: minimizing complications in intraocular lens calculations. Semin Ophthalmol . 2014;29(5-6):376-379. doi:10.3109/08820538.2014.959193.