Could Rectal Spacers Spare the Neurovascular Bundle During Robotic SBRT in Prostate Cancer?
Could Rectal Spacers Spare the Neurovascular Bundle During Robotic SBRT in Prostate Cancer?
Sara Simões *1, Mário Esteves Leal 1, Guilherme Campos 2, Carlos Fardilha 2, Paulo Costa 2
1.Radiation Therapy Department, Hospital de Braga (Rua Sete Fontes, São Victor 4710-243, Braga, Portugal).
2.Radiation Therapy Department, Júlio Teixeira S.A, CUF Institute (Rua Fonte das Sete Bicas, nº170, Senhora da Hora 4460-188, Porto, Portugal).
*Correspondence to: Sara Simões. Radiation Therapy Department, Hospital de Braga (Rua Sete Fontes, São Victor 4710-243, Braga, Portugal).
Copyright
© 2024 Sara Simões. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2024
Published: 01 April 2024
DOI: https://doi.org/10.5281/zenodo.14512059
Abstract
Purpose or Objectives: To characterize the use of a prostate-rectum spacer during robotic stereotactic body radiation therapy (SBRT) for prostate cancer, concerning: dose to the neurovascular bundle (NVB); sexual impairment.
Materials and Methods: From September 2019 to August 2022, 64 patients were submitted to rectal spacer insertion, and twelve of these patients with histologically confirmed prostate adenocarcinoma, were enrolled into a prospective study at private health institute, clinical stage of T1c-2c and NCCN risk group between very low and favourable intermediate risk. No patients underwent androgen deprivation therapy (ADT). Enrolled patients underwent baseline CT scan and fiducial markers implant. Perirectal hyaluronic acid spacer (HAS) was injected and patients were rescanned with CT and MRI. NVB volumes were generated according to POTEN-C Trial in both pre and post HAS scans. Dosimetric plans were generated on both scans (pre-spacer and post-spacer) for dosimetric comparison of NVB. Dose prescribed to the prostate was 35-37.5Gy in 5 fractions. Patients sexual function was evaluated using Expanded Prostate Cancer Index Composite (EPIC 26) Questionnaire before starting treatment and again after 3 months. Comparison of dosimetric parameters was performed using the Paired-sample T Test and Wilcoxon Test, using the IBM SPSS Statistics version 26 software.
Results: The population (n=12) included males with a mean age of 66 (±4.61) years. Mean prostate volume (PV) was 53.98 (±14.42) cc. V5, V10, V20, V30, mean and maximum doses reductions were observed in the NVB before and after spacer. Mean EPIC scores did not change significantly before and after treatment (20.16±2.24 vs 19.25±2.73, p>0.04) with rectal spacer.
Conclusion: The presenting study proves that HAS significantly reduces dose to NVB with stereotactic robotic radiosurgery, which potentially might decrease sexual impairment. Mean EPIC scores did not change significantly indicating that in our cohort did not deteriorate compared to their pre-SBRT sexual scoring index. Longer follow up, and a larger number of patients without ADT will strengthen our results.
Key words: neurovascular bundle; stereotactic body radiation therapy; prostate-rectum spacer; hyaluronic acid; prostate cancer.
Could Rectal Spacers Spare the Neurovascular Bundle During Robotic SBRT in Prostate Cancer?
Introduction
Prostate cancer accounts for nearly 33,000 deaths annually, representing the second-most common cause of cancer death among men, ranking only behind lung cancer.[1] Prostate cancer can be grouped into early-stage cancer or advanced-stage cancer, and the first one is highly treatable and often curable. Most people with early-stage disease can live without cancer for many years, but the treatments are often accompanied by side effects that decrease the patient's quality of life. Definitive radiotherapy is a well-recognized treatment option for localized prostate cancer. Sexual dysfunction, anal-rectum toxicity and urinary symptoms are the three most common complaints following prostate radiotherapy. [2]
Prostate radiotherapy is associated with erectile dysfunction probably due to relationship between radiation dose to the NVB and the development of erectile dysfunction following prostate radiation therapy. The application of a spacer to increase the distance between the prostate and anterior rectal wall is an innovative technique, reducing the dose to the rectum and others healthy tissue. Hyaluronic acid is a potential material to create the desired effect since it is easily placed and is naturally absorbed over time. Furthermore, Stereotactic body radiation therapy (SBRT) uses high-energy radiation beams to treat in fewer treatments and allows for precise high dose radiation with minimal exposure to adjacent healthy tissue. The Cyber Knife SBRT system employs a robotic, arm-mounted, miniaturized 6 MV linac with 6 degrees of freedom. The system’s ability to deliver extremely precise and accurate treatment.[3]
Clinical results and randomized studies are needed to understand and better define the combined beneficial effect for the patient using SBRT and hyaluronic acid spacer to minimize exposure to neurovascular bundle (NVB). Data outlining sexual function and oncological outcomes are limited to date. Our purpose is to characterize the effect of a prostate-rectum spacer on the dose to neurovascular bundle (NVB) during robotic stereotactic body radiation therapy (SBRT) for prostate cancer. This study evaluated patient-reported sexual toxicities using Expanded Prostate Cancer Index Composite (EPIC 26) Questionnaire in patients who have had spacer insertion. Because it is known that ADT can cause sexual impairment, we selected patients that did not take it, and doing so, we are eliminating a bias to this study.
Methods
Study Population:
From September 2019 to August 2022, 64 patients with histologically confirmed prostate adenocarcinoma and submitted to rectal spacers. Twelve patients were enrolled into a prospective study at a private health institute in North of Portugal, accordingly to the following inclusion criteria: age >= 18 years, clinical stage of T1c-2c, Karnofsky Performance Status > 70 and NCCN risk group between very low and favorable intermediate risk. No patients underwent androgen deprivation therapy (ADT).
The exclusion criteria were: patients with evidence of extra prostatic extension or seminal vesicle involvement; inability to undergo multi-parametric MRI; evidence of metastatic disease or clinical nodal involvement; previous pelvic radiotherapy; patients who have baseline severe urinary symptoms; patients with a known allergy or contraindication to spacer products; patients with uncontrolled coagulation disorder, inflammatory bowel disease and chronic renal disease; patients who have a history of significant psychiatric illness and patients who had pacemaker or bone prosthesis. The treatment was proposed during the initial consultation after a multidisciplinary group decision and was accepted by the patients. All patients provided written informed consent for treatment with robotic stereotactic body radiation therapy (SBRT) for prostate cancer. Patients sexual function was evaluated using Expanded Prostate Cancer Index Composite (EPIC 26) Questionnaire before starting treatment and 3 months after treatment. This EPIC-26 questionnaire, which is used for measuring health-related quality of life, was applied here, but only parameters related to sexual function were registered, which were questions numbered through 8 to 12. The mean of questions’ score was performed for each patient and compared with the mean questions’ score at 3 months. Higher score is associated with poorer quality of sexual function. Comparison of dosimetric parameters was performed using the Paired-sample T Test and Wilcoxon Test, using the IBM SPSS Statistics version 26 software. Chi-square test was used to find a correlation between the two EPIC scores.
Simulation:
All patients underwent a baseline history and physical examination. The following medication was prescribed: ciprofloxacin 500 mg every 12 hours, starting 48 hours before the implant, and a laxative Microlax (applied 2 the night before and applied 1 on the day of the procedure 1 to 2 hours before the procedure). The patient was provided with the following instructions verbally and in writing: do not take anti-inflammatory drugs in the week preceding the procedure; on the night before, choose light meals without consuming solid foods; continue with regular medication, except for anti-inflammatory drugs and on the day of the procedure, fast for 4 hours. Enrolled patients underwent baseline CT scan and four fiducial markers implants. Perirectal hyaluronic acid spacer (HAS) was injected via transperineal approach between the Denonvilliers fascia and the anterior rectal wall. Local or general anaesthesia and aseptic technique was observed. Antibiotic prophylaxis was administered before any manipulation as previously mentioned above. All patients were rescanned with CT and MRI with a comfortably full bladder and empty rectum. Planning scans are carried out on the same day, within a very short period of time between them (< 1 hour), to ensure the rectum and bladder are as similar as possible across the scans. Following the planning CT, a catheterised CT scan is always performed to delineate the urethra.
Planning and plan comparison: NVB volumes (OARs) were generated according with the POTEN-C clinical trial (Prostate Oncologic Therapy While Ensuring Neurovascular Conservation - NCT03525262) in both pre and post HAS CT scans, consisting of the neurovascular bundle, penile bulb and pudendal arteries. Planning Organ at Risk Volume (PRV) represents a 3mm expansion from NVB volume. Prostate GTV represented MR defined dominant radiographic disease, CTV as the full prostate with the insertion of the seminal vesicles, PTV defined as CTV+5mm margin excluding the urethra with a margin of 1 mm to spare this volume. Dosimetric plans were generated on both scans (pre-spacer and post-spacer) for dosimetric comparison of NVB. Dose prescribed to the prostate was 35-37.5Gy in 5 fractions. Treatments plans were performed with MLC collimator for 11 patients and Iris for one patient. All plans were normalized to a dose prescription curve to ensure at least a 95% dose coverage to the PTV. The average prescription curve was 87.2% for pre-spacer ranging from 83.1% to 89.9%. For post-spacer plans, the average prescription curve was 83.2% ranging from 69.5% to 88.9%. All plans were calculated with Monte Carlo algorithm with a 1% uncertainty.
Results
The population (n=12) included males with a mean age of 66 (±4.61) years, presenting with a mean PSA 6.37 (± 2.53) ng/mL. 58% (7 patients) presenting a gleason score of 6. Mean prostate volume (PV) was 53.98 (±14.42) cc. Mean volume of HAS administered was 16.58 (±0.36) mL. The mean follow up was 3 (±0.53) months. Table 1 show the results of our study.
|
Neurovascular bundle (NVB) dosimetry |
Non - hyaluronic acid spacer plans |
Hyaluronic acid spacer plans |
P value |
|
Mean dose (Gy, DP) |
36.55± 3.50 |
33.85±2.66 |
0.007 |
|
Maximum dose (Gy, DP) |
40.40± 1.87 |
39.16±1.68 |
0.01 |
|
V5Gy (cc, DP) |
3.27±0.86 |
2.54 ±0.54 |
0.019 |
|
V10Gy (cc, DP) |
3.20±0.92 |
2.45 ±0.55 |
0.016 |
|
V20Gy (cc, DP) |
3.09±1.01 |
2.32 ±0.56 |
0.026 |
|
V30Gy (cc, DP) |
3.02±1.06 |
2.24 ±0.50 |
0.025 |
Table 1: Dosimetric results.
As seen in Table 1, there was observed a statistically significant decrease in mean dose in NVB when comparing non-hyaluronic acid spacer plan with hyaluronic acid spacer plan, from 36.55± 3.50Gy to 33.85±2.66Gy (p=0.007). The same observation was found regarding maximum dose, with a reduction from 40.40± 1.87Gy to 39.16±1.68Gy. The amount of volume of NVB irradiated with 5Gy, 10Gy, 20Gy and 30Gy also significantly decreased (p=0.019, p=0.016, p=0.26, p=0.025).
|
EPIC Questionnaire results (Regarding impotence) |
Before RT |
After RT |
P value |
|
Mean score |
20.16±2.24 |
19.25±2.73 |
>.04 |
Table 2: EPIC results
The mean score of EPIC questionnaire previous treatment compared with score after treatment also reduced, from 20.16±2.24 to 19.25±2.73, however, this difference was not statistically significant(p>0.04).The PV does not correlate significantly with the mean dose (p=0.067), maximum (p=0.359), V5 (p=0.157), V10 (p=0.157), V20 (p=0.157) and V30 (p=0.299) to NVB after placing the HAS. There were no reports of any long term adverse events including rectal perforation, or infection after HA injection. Results are similar using PRV with 3 mm of margin. There were no reports of any adverse events including rectal perforation, or infection after HA injection.
Discussion
NVB is localized posterolaterally to the prostate and is one of the structures responsible for erectile function. Prostate radiotherapy is associated with erectile dysfunction probably due to radiation dose to the NVB or penile bulb, but this is not clear. Several studies have investigated the impact of spacer insertion on dosimetry to penile bulb, however, most did not show significant changes to the penile bulb dosimetry.[4] Only a secondary analysis of a Phase 3 randomized trial showed a lower dose in patients who had spacer insertion compared to those who did not. [5] This study also evaluated patient- reported sexual toxicities using EPIC questionnaires and they reported that in subgroup of patients who had adequate baseline sexual function, spacer insertion was associated with better sexual function at 3 years (p=0.03). The authors correlate these data with the lowest dose in the bulb of the penis. Nowadays, it is not clear whether the sexual dysfunction is due to the dose effect on the bulb or on the neurovascular bundle. Another study randomized by Pinkawa et al. showed better sexual function in patients who had spacer insertion. [6] Besides that, data from the randomized trial PACE-A (Prostate Advances in Comparative Evidence) indicates that SBRT better preserves sexual function in men with localized prostate cancer in comparison to surgery. With these data, it becomes clear that it is necessary future research to integrate the use of spacers with Robotic SBRT. POTEN-C is a Phase 2 trial, currently recruiting, and aims to evaluate the impact of spacer use in neurovascular-sparing prostate SBRT on erectile function maintenance (NTC03525262). In our cohort, prostate rectum spacer was associated with lower dose in the NVB during SBRT, therefore our hypothesis is that further preservation of erectile function can be achieved with this approach.
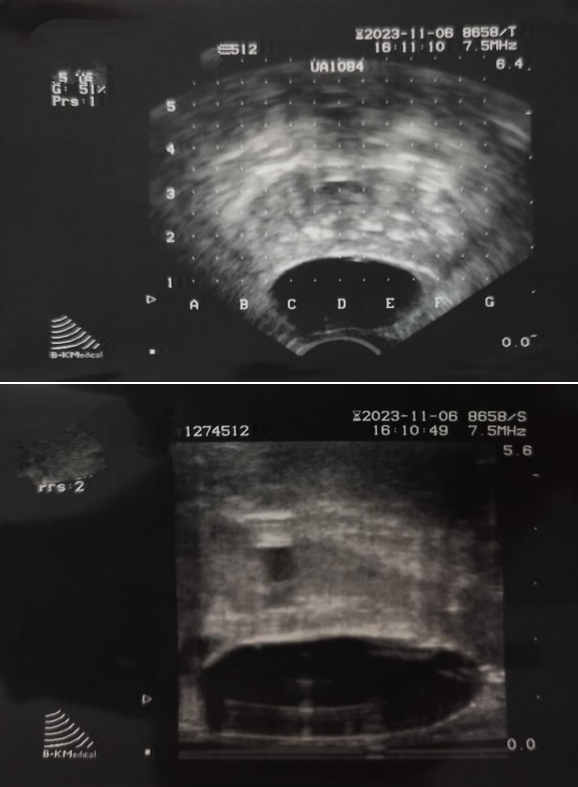
Figure 1: Rectal spacer seen on transrectal ultrasound.
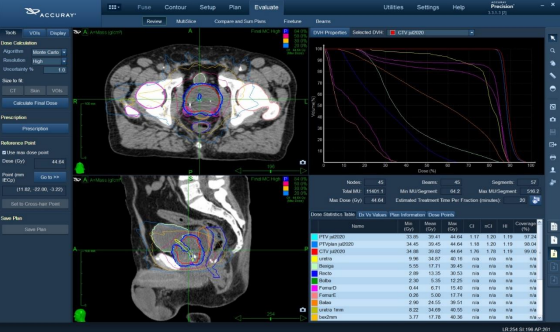
Figure 2: Example of a radiotherapy treatment planning
Conclusion
HAS can be used to reduce radiation dose to the rectum, and presenting study proves that HAS significantly reduces dose to NVB with stereotactic robotic radiosurgery. V5, V10, V20, V30, mean and maximum doses reductions were observed in the NVB, which potentially might decrease sexual impairment. None of the patients underwent androgen deprivation therapy (ADT). Mean EPIC scores did not change significantly indicating that in our cohort did not deteriorate compared to their pre-SBRT sexual scoring index. Longer follow up, and a larger number of patients without ADT will strengthen our results.
References
1. Siegel RL, Miller KD, Jemal A. Cancer Statistics 2020. CA Cancer J Clin. 2020; 70: 7-30. doi:10.3322/caac.21590.
2. Hoffman RM, Hunt WC, Gilliland FD, Stephenson RA, Potosky AL. Patient satisfaction with treatment decisions for clinically localized prostate carcinoma. Results from the Prostate Cancer Outcomes Study. Cancer. 2003;97:1653–1662. doi: 10.1002/cncr.11233.
3. Lei S, Piel N, Oermann EK, Chen V, Ju AW, Dahal KN, et al. Six-Dimensional Correction of Intra-Fractional Prostate Motion with CyberKnife Stereotactic Body Radiation Therapy. Front Oncol. 2011;1:48. doi: 10.3389/fonc.2011.00048.
4. Chao M, Ow D, Ho H et al. Improving rectal dosimetry for patients with intermediate and high-risk prostate cancer undergoing combined highdose-rate brachytherapy and external beam radiotherapy with hydrogel space. J Contemp Brachytherapy 2019; 11: 8–13.
5. Hamstra DA, Mariados N, Sylvester J et al. Sexual quality of life following prostate intensity modulated radiation therapy (IMRT) with a rectal/prostate spacer: secondary analysis of a phase 3 trial. Pract Radiat Oncol 2018; 8: e7–15.
6. Pinkawa M, Berneking V, Schlenter M, Krenkel B, Eble MJ. Quality of life after radiation therapy for prostate cancer with a hydrogel spacer: 5- year results. Int J Radiat Oncol Biol Phys 2017.