Endoscopic Findings of Ulcerative Ileitis due to the use of Mycophenolate Mofetil in Capsule Endoscopy: A Case Report
Endoscopic Findings of Ulcerative Ileitis due to the use of Mycophenolate Mofetil in Capsule Endoscopy: A Case Report
Julio Cesar de Soares Veloso1*; Barbara Elizabeth das Neves Alves Fortes2; Rebeca Cristina Souza de Andrade3; Maria Carolina Santos Menezes4; Marina Toscano Silveira5; Caio de Carvalho Motta de Souza6; João Pedro Abbott Cabral de Oliveira7, Julia Schettini Veloso8
*Correspondence to: Julio Cesar de Soares Veloso, MD – Gastroenterologist and Endoscopist at Hospital Anchieta and Hospital Santa Helena, Brasilia (Brazil).
Copyright
© 2024 Julio Cesar de Soares Veloso. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 April 2024
Published: 01 May 2024
Abstract
Mycophenolate mofetil (MMF) is an immunosuppressive drug widely used after organ transplantation to prevent rejection, as well as an off-label treatment of some autoimmune diseases1,2,4. MMF’s mechanism of action is through the inhibition of the enzyme inosine monophosphate dehydrogenase, essential in the synthesis of purines by some cells in the body1. T and B lymphocytes preferentially use this pathway for cell proliferation1. The most common side effects are mainly related to the gastrointestinal tract, the most frequent being diarrhea, abdominal pain, nausea, and vomiting1. More rarely, severe effects such as ulcers, bleeding and perforation may occur. The reasons for the occurrence of these adverse events are not fully known and may be related to direct irritative toxic effects1. Generally, these adverse events usually disappear with the reduction or suspension of the drug use1,2,3. Although the association with gastrointestinal toxicity is well known, there are few reports of the associated endoscopic findings4.
Endoscopic Findings of Ulcerative Ileitis due to the use of Mycophenolate Mofetil in Capsule Endoscopy: A Case Report
Case Report
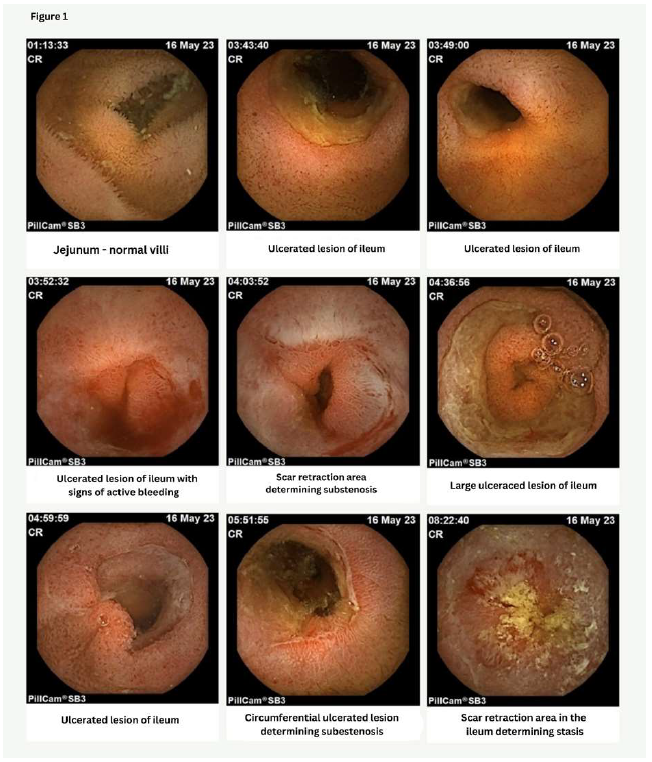
This is a 65-year-old female patient who came to the consultation for video capsule endoscopy (VCE) to investigate digestive bleeding of obscure origin. The patient reported melena, anemia and constipation that had started months before the current appointment. She denied any history of abdominal pain. She had Systemic Lupus Erythematosus and had been treated with MMF for 6 years due to lupus nephritis. She also used prednisone, hydroxychloroquine, acetylsalicylic acid, calcium, and enalapril maleate. Upper and lower gastrointestinal videoendoscopy performed previously were normal. Fecal occult blood test was positive and fecal calprotectin was normal. CT enterography showed small segments of thickening and parietal stratification of intestinal loops. In the VCE several ulcerated lesions were observed in the ileum, some of which determined substenosis, without alterations in the jejunum (Figure 1). The capsule was retained in the small intestine during the examination, but a few days later, it was no longer visualized on a plain X-ray of the abdomen. The use of MMF was discontinued and the use of oral budesonide was started for 8 weeks. Following the ending of the treatment, the patient reported complete improvement of the symptoms and a new follow-up CT scan did not show the changes previously seen.
Discussion
MMF is an immunosuppressive drug widely used after organ transplantation1,4. It exerts its immunosuppressive effect by preventing the replication of T and B lymphocytes1. Its mechanism of action involves the inhibition of the enzyme inosine monophosphate dehydrogenase, which is responsible for the de novo purine synthesis pathway1.
It is known that enterocytes are 50% dependent on the de novo purine synthesis pathway for the occurrence of cell proliferation1. The intestinal epithelium has high proliferative activity and is therefore particularly susceptible to injury due to the action of antimitotic medications that interfere with normal cell proliferation1. These intestinal cells of the gastrointestinal tract also have a high intracellular concentration of mycophenolic acid, and one of its metabolites, acyl glucuronide, can induce the production of pro-inflammatory cytokines such as IL-6 and TNF-alpha1,3,4.
The most frequently observed adverse events with the use of MMF are diarrhea, abdominal pain, nausea and vomiting, most of which are due to direct irritative action1. Severe gastrointestinal adverse events are rare and may include ulcers, gastrointestinal bleeding, and perforation. In the event of ulcerative disease in patients receiving MMF, discontinuation of the drug is recommended1,3. Generally, MMF is usually administered as a fixed dose of 2 g/day, as recommended by the manufacturer, and it is known that the dose may be directly related to the occurrence of these side effects1. In this context, dose individualization based on laboratory tests could help avoid these complications1.
On VCE examination, skip lesions were seen in the topography of the ileum, characterized by the presence of large circumferential ulcerated lesions, edema, friability, active bleeding and substenosis. The capsule was retained in one of these lesions during the examination, but it was not visualized days later on a plain X-ray of the abdomen.
In the present case, the use of MMF was suspended together with the use of acetylsalicylic acid, which could be potentializing the occurrence of ulcerative lesions in the ileum. Consequently, complete remission of both the bleeding symptoms reported by the patient and the normalization of the radiological findings in CT enterography were observed.
Figure 1
Conclusion
MMF is an immunosuppressive drug widely used in transplant patients and in some autoimmune diseases. The most commonly reported adverse reactions are due to gastrointestinal tract toxicity and include diarrhea, abdominal pain, nausea, and vomiting. Severe effects such as ulcers, bleeding, and perforation of the gastrointestinal tract are rarer. In this article, we report the infrequent occurrence of ulcerative lesions and substenosis in the ileum in a patient using MMF. In the event of severe adverse reactions, discontinuation of the drug is generally recommended.
References
1.Behrend, M. 2001. “Adverse Gastrointestinal Effects of Mycophenolate Mofetil: Aetiology, Incidence and Management.” Drug Safety 24 (9): 645–63. https://doi.org/10.2165/00002018-200124090-00002.
2. Bhattacharya, Sumona, Gianna Stoleru, Preet Patel, Ameer Abutaleb, Kristen Stashek, and Raymond K. Cross. 2022. “Characterization of Mycophenolate Mofetil Gastrointestinal Toxicity and Risk Factors for Severe Disease and Poor Prognosis.” Inflammatory Bowel Diseases 28 (5): 811–14. https://doi.org/10.1093/ibd/izab254.
3.Bunnapradist, Suphamai, and Patrice M. Ambühl. 2008. “Impact of Gastrointestinal-Related Side Effects on Mycophenolate Mofetil Dosing and Potential Therapeutic Strategies.” Clinical Transplantation 22 (6): 815–21. https://doi.org/10.1111/j.1399-0012.2008.00892.x.
4.Sonoda, Akira, Kurato Wada, Kazuhiro, Kensuke Fukuda, Mitsutaka Shuto, Kazuhisa Okamoto, Ryo Ogawa, Tadayoshi Okimoto, and Kazunari Murakami. 2017. “Deep Ulcers in the Ileum Associated with Mycophenolate Mofetil.” Internal Medicine 56 (21): 2883–86. https://doi.org/10.2169/internalmedicine.8815-17.