6 Years Old Boy with Non-Hudgken Lymmphoma Preceded by Urticareal Reaction Episodes Several Years from the Cancer, an Reversed Event of the Common Scenario.
6 Years Old Boy with Non-Hudgken Lymmphoma Preceded by Urticareal Reaction Episodes Several Years from the Cancer, an Reversed Event of the Common Scenario.
Dr. Ahmed Moosa Yahya Assery *
*Correspondence to: Dr. Ahmed Moosa Yahya Assery, Paediatrics ambulatory care consultant. King Abdulaziz Medical City, National Guard Medical Affairs, Family Medicine-Ambulatory care, NGCSC.
Copyright
© 2024: Dr. Ahmed Moosa Yahya Assery. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 October 2016
Published: 18 November 2016
Abstract
Non-Hodgkin lymphoma in paediatrics represent one the almost save (non-killing) cancers after the huge upgrading in its early diagnosis and treatment. One of the well-known courses of such cancer in children are its association with a subsequent urticarial reactions and sometimes anaphylactic reactions but what was surprising thing in this case was the opposite where the patient here suffered from frequent urticarial skin episodes almost 5 years prior the onset of the clinical manifestations of the non-Hodgkin lymphoma? which very strange The thing attracted me to seek about a similar cases reported with the same disorder course to at least investigate any link between the two entities specifically the frank question? Are the urticarial reactions in paediatrics considered an alarm for a coming non-Hodgkin lymphoma or not?
Keywords: Non-Hodgkin lymphoma: NHL.
Hodgkin lymphoma: HL.
Lymph Node: LN.
Lymphadenopathy: LNY.
Anaplastic Large Cell Lymphoma: ALCL
Urticaria: URTC.
Central nervous system: CNS.
Follow Up: FU.
Angioimmunoblastic T cell lymphoma: AITL.
6 Years Old Boy with Non-Hudgken Lymmphoma Preceded by Urticareal Reaction Episodes Several Years from the Cancer, an Reversed Event of the Common Scenario.
Introduction
NHL consists of a diverse group of malignant neoplasms of the lymphoid tissues variously derived from B cell progenitors, T cell progenitors, mature B cells, or mature T cells. Unlike in adults where low-grade, clinically indolent NHL subtypes predominate, most paediatric NHL cases are of high grade and have an aggressive clinical behaviour. Whenever possible, children with NHL should be treated in a comprehensive paediatric oncology cancer by a multidisciplinary team experienced in the diagnosis and care of children with cancer.
Clinically and initially Potential emergency complications of NHL may be present at the time of diagnosis and need to be considered during the initial workup and evaluation of a patient with suspected paediatric NHL. Prompt recognition and therapy are critical for these situations, which may be life-threatening or may interfere with and delay treatment of the underlying NHL.
These can include:
- Superior or inferior vena cava obstruction.
- Acute airway obstruction.
- Intestinal obstruction, intussusception.
- Spinal cord compression.
- Pericardial tamponade.
- Lymphomatous meningitis and/or CNS mass lesions.
- Hyperuricemia and tumour lysis syndrome.
- Ureteral obstruction, unilateral or bilateral hydronephrosis.
- Venous thromboembolic disease.
Patients with large mediastinal masses are at increased risk of respiratory or cardiac arrest during general anaesthesia or heavy sedation. Patients who present with cardiorespiratory symptoms or radiographic evidence of tracheal obstruction are at greatest risk of perioperative respiratory morbidity.
Tumour lysis syndrome is an oncologic emergency that is caused by massive tumour cell lysis and the release of large amounts of potassium, phosphate, and uric acid into the systemic circulation. Deposition of uric acid and/or calcium phosphate crystals in the renal tubules can result in acute renal failure, which is usually anuric.
Signs and symptoms — The clinical presentation of paediatric NHL varies depending upon the type of lymphoma and the areas of involvement. Symptoms develop quickly, usually over one to three weeks. NHL commonly presents as enlarging, non-tender lymphadenopathy or as symptoms due to the compression of surrounding structures, such as new onset wheezing, facial swelling, respiratory distress, asymmetrical tonsils, or acute abdominal pain. Hepatic and/or splenic enlargement may be present in patients with advanced stage NHL.
CNS involvement occurs in 6 percent of paediatric NHL with rates ranging from 8.8 percent in Burkitt lymphoma to <3 percent in diffuse large B cell lymphoma. A significant minority of patients will have systemic complaints of fever, weight loss, or night sweats. While certain clinical presentations are suggestive of specific NHL histologist, a definitive diagnosis requires a biopsy of involved tissue, as described below. (1).
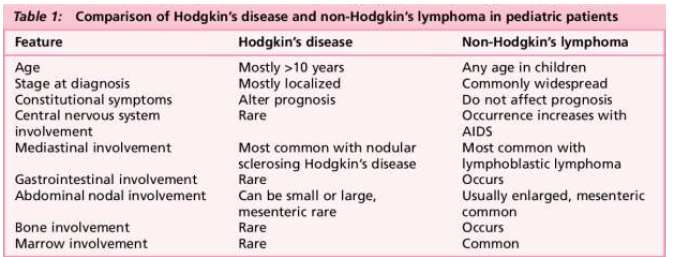
Still there are some medical general practitioners and paediatrician confused between the NHL and HL so here briefly I passed about that point as a summary in the table down of the article. (Table No 1). (2).
URTC or hives (sometimes referred to as welts or wheals), is a common disorder, with a lifetime prevalence of approximately 20 percent in the general population. A typical urticarial lesion is an intensely pruritic, erythematous plaque (picture 1). Urticaria is sometimes accompanied by angioedema, which is swelling deeper in the skin. A presumptive trigger, such as a drug, food ingestion, insect sting, or infection, may be identifiable in patients with new onset urticaria, although no specific cause is found in many cases, particularly when the condition persists for weeks or months. URTC classified as:
Acute urticaria — Urticaria is considered acute when it has been present for less than six weeks.
Chronic urticaria — Urticaria is considered chronic when it is recurrent, with signs and symptoms recurring most days of the week, for six weeks or longer.
The period of six weeks is somewhat arbitrary and simply represents a timeframe in which new cases of urticaria usually resolve. More than two-thirds of cases of new-onset urticaria prove to be self-limited (acute). The lesions of acute and chronic urticaria are identical in appearance, so when the problem first develops, it is not possible to differentiate the two disorders.
URTC can be triggered by many causes sunnitized in (Table No 2). (3).
Table No 1. The major differences between HL and NH
picture 1: The skin manifestations of the URTC
Table No 2: The common aetiologies of URTC
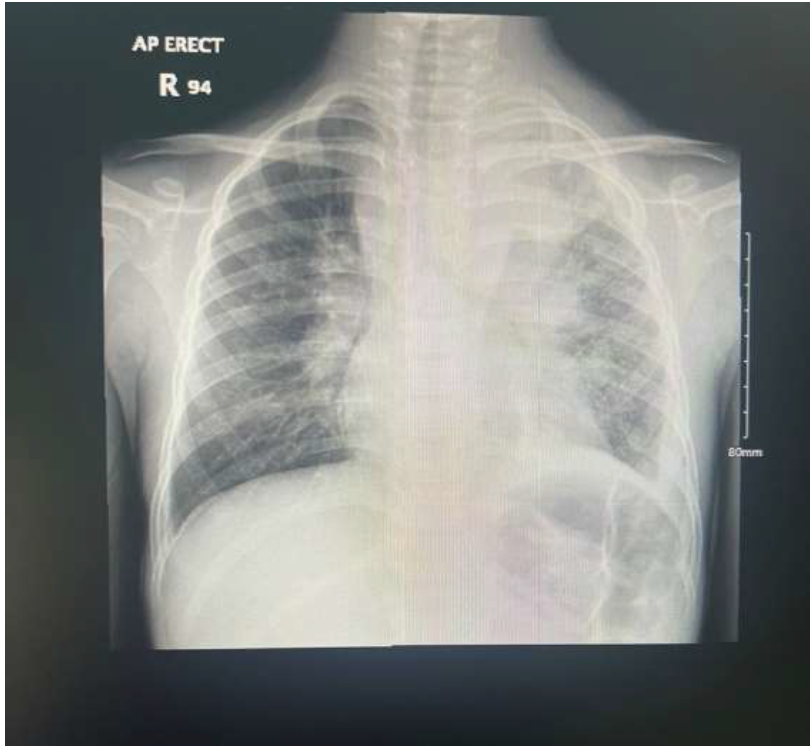
Picture No 2: The patient chest x-ray with striking broncho-pneumonia
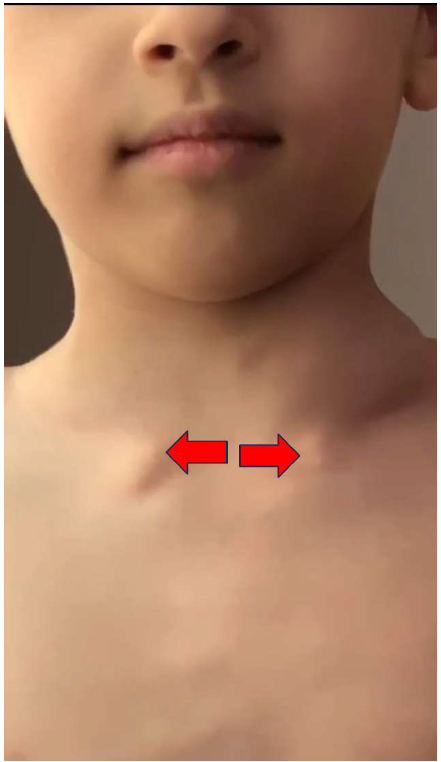
picture 3: The patients supraclavicular and suprasternal lymphadenopathies
Our Case Presentation:
The story of our case started with symptoms of fever and cough that managed in the ward as a pneumonia where CXR done that incidentally showed a hailer lymphadenopathy (picture 2).among the FU in the floor the treating team noticed a selling of the left supraclavicular LN also the suprasternal one (picture 3).. Haematology-oncology team consulted, and they decided to perform further imaging that came with presence of massive hailer LNY (picture 4). Blood smear requested then for the child came suggestive of type ALCL after which the child started soon on the chemotherapy till, he cured completely. This patient since he was 2 years old was suffering from frequent episodes of urticarial skin reactions in form of itching, heaves and wheals approached to the degree of anaphylactic shock needed an admission to the PICU and was put in stand-up epinephrine pin (picture 5).again what triggered my curiosity in this case that the URTC problem preceded the NHL made me so excited to search in the articles what is the real link between the two entities, how percent and who should precede the other?
Picture 4: The radiologist report of the enhanced chest CT scan demonstrated What was most likely malignant process of the hailer LN
picture 5: The epinephrine pins the patient given for any anaphylactic reactions and here it looks he was receiving one pin as an urgent tretment
The Case Report Discussion:
NHL represents the fifth most common diagnosis of paediatric cancer in children under the age of 15 years, and it accounts for approximately 7 percent of childhood cancers in the developed world. In the United States, approximately 800 new cases of paediatric NHL are diagnosed annually with an incidence of 10 to 20 cases per million people per year. This incidence appears to be increasing overall, largely thought to reflect a rise in NHL among adolescents. The median age at diagnosis is approximately 10 years, and the incidence increases with age. Lymphomas are rare in infants (≤1 percent) and account for approximately 4, 14, 22, and 25 percent of neoplasms in children aged 1 to 4, 5 to 9, 10 to 14, and 15 to 19 years, respectively. There is a male predominance, and White children are more commonly affected than African American children.
The incidence and distribution of specific NHL subtypes differs by population (e.g., age, race) and geographical region. In general, the most common subtypes of paediatric NHL are derived from B cell progenitors. In the United States and other developed countries, the most common subtypes are Burkitt lymphoma, diffuse large B cell lymphoma, lymphoblastic T cell or B cell lymphoma, and ALCL. Other subtypes (e.g., follicular lymphoma, marginal zone lymphoma) are less common, accounting for approximately 7 percent of paediatric NHL. (1).
Regarding UTRC the exact prevalence is unknown because reliable epidemiologic studies are scarce in children with chronic urticaria. In a recent population-based German birth cohort study, the incidence and cumulative prevalence of urticaria in infants and children were reported. The incidence of urticaria was approximately 1% per year of age and the cumulative prevalence of urticaria in children at the age of 10 years was 14.5% for boys and 16.2% for girls, but the prevalence of chronic urticaria was not evaluated separately.
In the current issue of the Allergy, Asthma and Immunology Research, Lee et al. reported a valuable study on the prevalence and risk factors of acute and chronic urticaria in Korean children, and it is the first population-based epidemiological study to estimate the prevalence of chronic urticaria in children. This cross-sectional study examined children from the general paediatric population aged 4-13 years, and a total of 4,076 children who completed full sets of questionnaires were enrolled. The lifetime prevalence’s of any type of urticaria and current urticaria were 22.5% and 15.3%, respectively. Among the current urticaria, the prevalence’s of acute, chronic, chronic continuous, and chronic recurrent urticaria were 13.9%, 1.8%, 0.7%, and 1.1%, respectively. (4).
From the search through medical articles in adults that connecting the NHL and URTC I found many contradictions and paradoxes as you will see here:
1_ Under the title Angioimmunoblastic T Cell Lymphoma Mimicking Chronic Urticaria published as a case report in Case Rep Med. 2016; 2016: 8753235.
Published online 2016 Jan 26. doi: 10.1155/2016/8753235 by Mohleen Kang, Nitasha Bhatia, Adrienne Sauder, and Mirela Feurdean reported a rare case of AITL presenting with chronic, recurrent angioedema and urticaria-like lesions and no palpable peripheral adenopathy. Primary Care physicians, dermatologists, and allergists must maintain a high index of suspicion for cutaneous manifestations of lymphoma, especially if the skin lesions are refractory to standard treatment. (5). Though the different subtype of lymphoma that NHL but here as you see the strange presenting symptom and sign that mimic the urticarial eruption.
2_ under the title Cancer Risk in Patients with Chronic Urticaria research published in ArchDermatol. 2012;148(1): 103-108.doi: 10.1001/archdermatol .2011.682 by Yi-Ju Chen, MD, PhD; Chun-Ying Wu, MD, PhD; Jui-Lung Shen, MD; et al which concluded that Patients with chronic urticaria are at increased risk of cancer, especially hematologic malignant tumours. Further studies are needed to delineate the associations. (6). That research though done on small sample of patients, but it strongly supports what we are facing in our case report.
3_under the title Allergic conditions are not associated with the risk of non-Hodgkin’s lymphoma or Hodgkin’s lymphoma: a systematic review and meta-analysis published in Onco Targets Ther. 2017; 10: 2189–2198.Also online 2017 Apr 18. doi: 10.2147/OTT.S128849 by Jia Yang, Hong’en Xu, Xiaodong Liang, Shiliang Lv, Baihua Lin, and Yongshi Jia. which clearly here opposing those results in the previous study (NO 2) in the same time unsupportive to our reassumed thinking in our case report and being done on huge number of patients sample in different nations make such study overcoming the previous one. This study mentioned that History of any allergic condition was not significantly associated with the risk of NHL or HL. Several specific allergic conditions, including asthma, hay fever, food allergy, and allergic rhinitis, might be associated with a reduced risk of NHL, while individuals with hay fever or food allergy may have a reduced risk of HL. Further large-scale prospective cohort studies are warranted to clarify the association between history of allergic diseases and the risk of lymphoma. (7).in this point of the discussion, I will ask myself and my medical collages shall we worry about the presence of many cases in paediatrics who is known to have urticarial skin eruption regarding the futural risk of NHL. Also, what is the real secrete behind those correlation and which of them should precede the other? URTC or NHL.
Conclusion:
For sure NHL and URTC are a usual inseparable two medical problems, why? Which should come first? how percent of their associations? Questions need more studies and case reports published to be answered.
References
1_ https://www.uptodate.com/contents/overview-of-non-hodgkin-lymphoma-in- children-and- adolescents?search=non%20hodgkins%20lymphoma&source=search_result&selec tedTitle=1%7E150&usage_type=default&display_rank=1.
2_https://www.semanticscholar.org/paper/Hodgkin's-and-non-Hodgkin's-lymphomas.-Rademaker/361ad6558837e1641f2a5d8d3d7c11cf1cc80556.
3_https://www.uptodate.com/contents/new-onset-urticaria?search=urticaria&source=search_result&selectedTitle=1%7E150&usage_ type=default&display_rank=1.
4_https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5352569/5-https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4746400/
6_https://jamanetwork.com/journals/jamadermatology/fullarticle/1105196. 7_https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5403013/