Effect of Inhaled Anticholinergic Drugs on Intraocular Pressure in Patients with Chronic Obstructive Pulmonary Disease Patients
Effect of Inhaled Anticholinergic Drugs on Intraocular Pressure in Patients with Chronic Obstructive Pulmonary Disease Patients
Dr Amit Kumar Pandey*1, Dr Richa Tripathi2
1. 1Department of Respiratory medicine, GSVM medical college, Kanpur
Correspondence to: Dr Amit Kumar Pandey, N9/29 J-8 janki nagar colony , patiya p.o. bazrardiha ,kakarmatta Varanasi 221002,Uttar Pradesh
Copyright.
© 2024 Dr. Amit Kumar Pandey. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 March 2024
Published: 01 May 2024
Effect of Inhaled Anticholinergic Drugs on Intraocular Pressure in Patients with Chronic Obstructive Pulmonary Disease Patients
Introduction
Nebulized Beta2 agonists and ipratropium bromide used for the treatment of COPD patients are known to cause glaucoma due to accidental instillation in eyes. Significance of anticholinergic drugs used as pressurised metered dose inhalers (pMDI) or dry powder inhalers (DPI) by patients with Chronic Obstructive Pulmonary Disease (COPD) causing raised intraocular pressure is unknown in patients with risk factors for glaucoma.
Material and Methods
Initially 126 patients were included. 6 were taking oral antihistamine cetrizine did not fulfil the protocol. 10 patients were excluded because they were not co-operating with the study protocol. There remained 110 patients on whom study was done. These 110 patients were divided into study group (70) received Ipratropium 40µg eight hourly or Tiotropium 18 µg once a day and Formoterol 6 µg twice a day plus Fluticasone 125 µg twice a day.and control group (40) received above medicines minus Ipratropium or Tiotropium. All the inhalers were given as metered dose Inhaler (pMDI) with spacer device. Ophthalmic examination and Gonioscopy were done as pre-treatment. Intra ocular pressure (IOP) measurements were done by Applanation tonometer before starting treatment, and thereafter weekly for four weeks at 4.00pm every day.
Observation and Result
In study group maximum change in intraocular pressure at 28th day was +7.4 mmHg in left eye and +7.0 mmHg in right eye in one patient. In control group maximum change in intraocular pressure was 3 mmHg in right eye and 3.70 mmHg in left eye in one patient.
In study group patients, mean change in intraocular pressure was 3.25±2.3 mmHg right ,3.52±2.2mmHg left ,more in grade 2 than in grade 3 which was 1.52±1.5 mmHg right,1.55±1.3 mmHg left and least in grade 4 (1.37±1.06 mmHg right,1.38±1.2 mmHg left) mmHg. Also the change was statistically significant (p=0.035).
In control group the change was found to be almost same among different angles.
4 patients with narrow angle (grade 2) and 3 with open angle (grade 3) developed intraocular pressure (IOP) beyond normal range (>20 mmHg), but all were normal on fundoscopic examination (Ocular Hypertension).
Mean change in intraocular pressure (IOP) was more in female population (2.18±1.76 right eye and 2.21±1.46 left eye) than in male population (1.60±1.71 right eye , 1.66±1.72 left eye) in study group .The change was not statistically significant .The change was almost same in control group.
In study group there were 4 patients with ocular symptoms at the end of 28th day which disappeared after discontinuing Tiotropium inhaler .
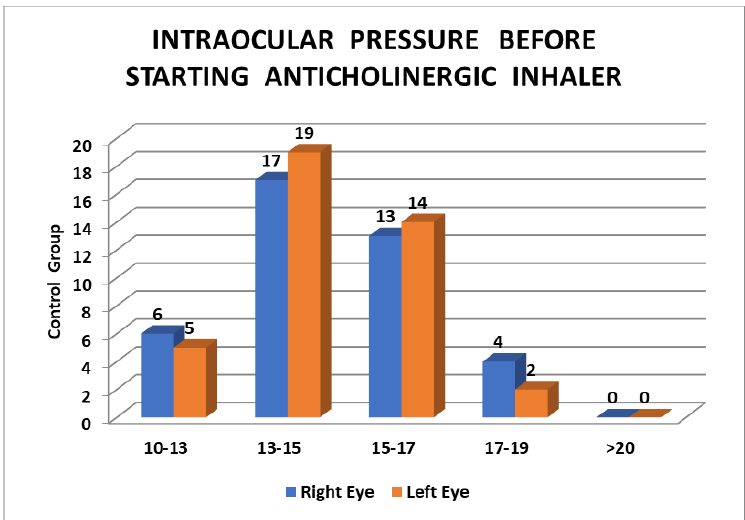
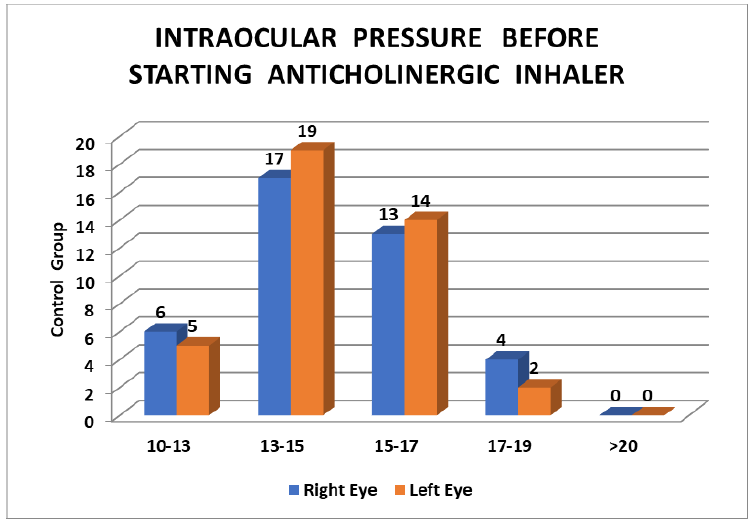
Table 1: Intra Ocular Pressure Before Starting Anticholinergic Inhaler
|
Intraocular pressure (iop) |
Study group |
Control group |
||
|
Right eye |
Left eye |
Right eye |
Left eye |
|
|
mmHg |
No. (%) |
No. (%) |
No. (%) |
No. (%) |
|
10-13 |
24 (34.28) |
24 (34.28) |
06 (15) |
05 (12.5) |
|
13-15 |
29 (41.42) |
31 (44.28) |
17(42.5) |
19 (47.5) |
|
15-17 |
09 (12.85) |
09 (12.85) |
13(32.5) |
14 (35) |
|
17-19 |
07 (10) |
06 (8.57) |
04 (10) |
02(5) |
|
More than 20 |
01(1.42) |
01 (1.42) |
00 |
00 |
|
Mean IOP |
13.931 ±1.968 |
13.931 ±2.221 |
13.774±1.540 |
13.689±1.789 |
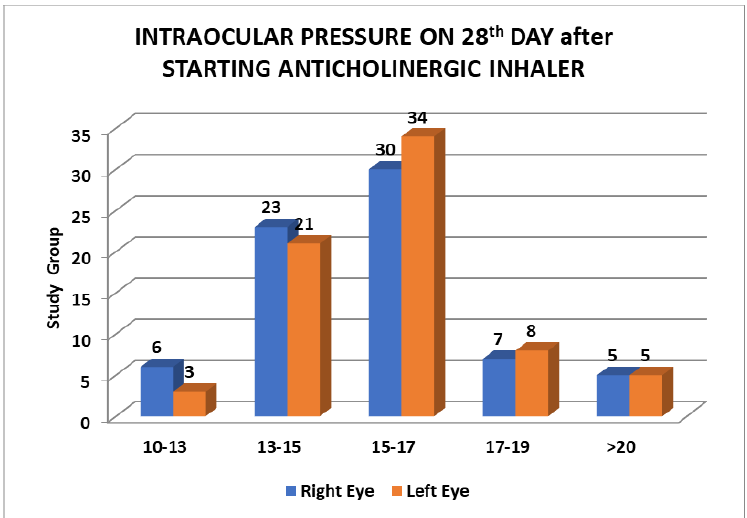
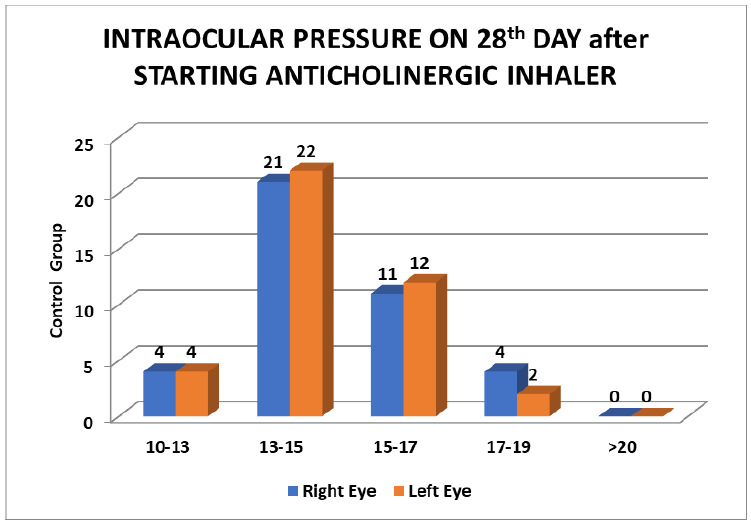
Table 2: Intraocular Pressure 28th Day After Starting Anticholinergic Inhaler
|
Intraocular Pressure (IOP) |
Right eye |
Control group |
||
|
mmHg |
No. (%) |
No. (%) |
No. (%) |
No. (%) |
|
10-13 |
06 (8.57%) |
03 (4.28%) |
04 (10%) |
04(10) |
|
13-15 |
23 (32.85%) |
21 (30%) |
21 (52.50%) |
22 (55%) |
|
15-17 |
30(42.85%) |
34 (48.57%) |
11 (27.5%) |
12(30%) |
|
17-19 |
07 (10%) |
08 (11.42%) |
04 (10%) |
02(5%) |
|
>20 |
05(7.14%) |
05 (7.14%) |
00 |
00 |
|
Mean IOP |
15.701±2.405 |
15.755±2.370 |
14.305±1.365 |
14.128±1.709 |
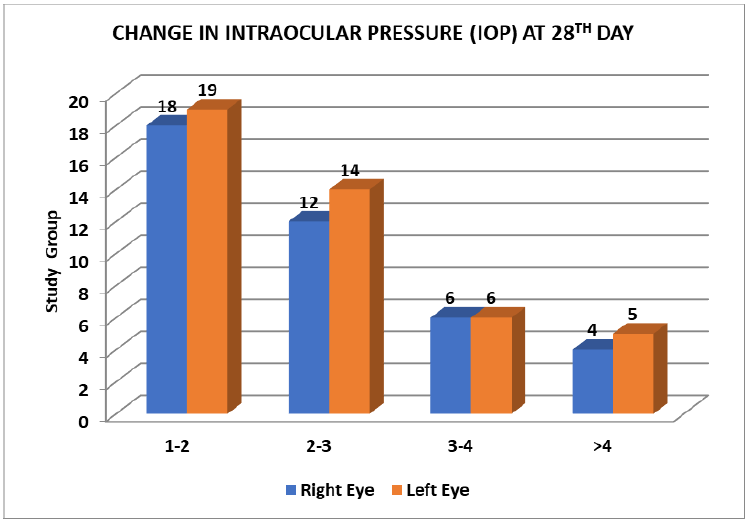
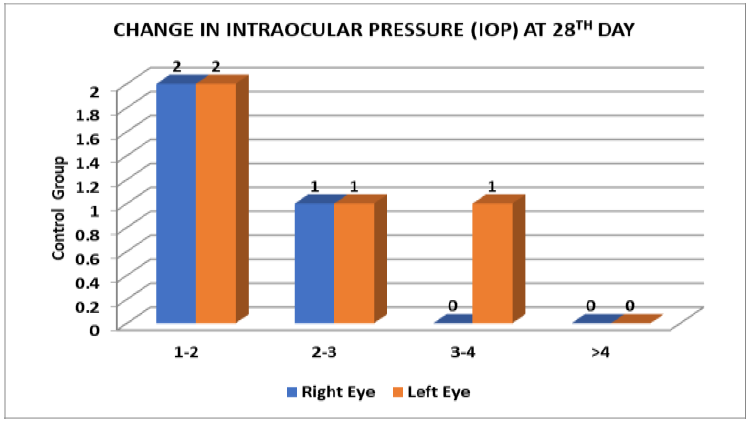
Table 3: Change In Intraocular Pressure (Iop) At 28th Day
|
Change in intraocular pressure (iop) |
Study group |
Control group |
||
|
mmHg |
Right eye |
Left eye |
Right eye |
Left eye |
|
1-2 |
18 |
19 |
2 |
2 |
|
2-3 |
12 |
14 |
1 |
1 |
|
3-4 |
6 |
6 |
0 |
1 |
|
>4 |
4 |
5 |
0 |
0 |
|
TOTAL |
40 |
44 |
3 |
4 |
Table 4; Mean Change In Intraocular Pressure Among Different Angles
|
Angle of anterior chamber (grade) |
Study group |
Control group |
||||||
|
Right eye |
Left eye |
Right eye |
Left eye |
|||||
|
No.of patients |
Mean change |
No.of patients |
Mean change |
No.of patients |
Mean change |
No.of patients |
Mean change |
|
|
2 |
13 |
3.25±2.3 |
11 |
3.52±2.2 |
3 |
0.53±0.3 |
3 |
0.56±0.8 |
|
3 |
38 |
1.52±1.5 |
42 |
1.55±1.3 |
21 |
0.54±0.7 |
21 |
0.58±0.8 |
|
4 |
19 |
1.37±1.06 |
17 |
1.38±1.2 |
16 |
0.48±0.6 |
16 |
0.03±0.9 |
|
TOTAL |
70 |
70 |
40 |
40 |
||||
Table 5: Distribution Of Change In Intraocular Pressure According To Sex
|
Change in intraocular pressure (iop) |
Study group |
Control group |
||||||
|
Male (n=50) |
Female (n=20) |
Male (n=30) |
Female (n=10) |
|||||
|
Right eye |
Left eye |
Right eye |
Left eye |
Right eye |
Left eye |
Right eye |
Left eye |
|
|
Increase |
44 |
44 |
17 |
20 |
27 |
24 |
10 |
10 |
|
Decrease |
6 |
6 |
3 |
0 |
6 |
6 |
0 |
0 |
|
Angle of anterior chamber(grade) |
Number of patients with intraocular pressure beyond normal(>20mmhg) |
Fundoscopy |
|
2 |
4 |
NORMAL |
|
3 |
3 |
NORMAL |
|
4 |
0 |
NORMAL |
Table 7: Distribution Of Mean Change In Intraocular Pressure With Sex
|
|
Study group |
Control group |
||
|
|
Mean change in intraocular pressure(mmhg) |
Mean change in intraocular pressure(mmhg) |
||
|
|
Right eye |
Left eye |
Right eye |
Left eye |
|
MALE (n=50) |
1.60±1.71 |
1.66±1.72 |
0.56±0.73 |
0.31±0.98 |
|
FEMALE (n=20) |
2.18±1.76 |
2.21±1.46 |
0.41±0.24 |
0.82±1.08 |
Fig 1, Fig 2, Fig 3, Fig 4, Fig 5, Fig 6
Conclusion
1. The inhaled anticholinergics (Tiotropium) once in a day given along with Formetrol and Fluticasone twice a day in COPD patients, all by Metered Dose Inhalers with spacer led to significant change (mainly increase) in intraocular pressure (IOP) after 4th week of starting treatment.
2. In control group where COPD patients were given only Formoterol plus Fluticasone by Metered Dose Inhalers did not lead to any significant change in intraocular pressure (IOP) after 4th week of starting treatment. Minor changes seen in some patients were within clinical therapeutic range.
3. Inhaled Anti-cholinergic drugs given as Metered Dose Inhalers can lead to Ocular Hypertension in COPD patients whose eyes were normal at initial clinical examination.
4. Increase in intraocular pressure was more in patients with narrow angle of anterior chamber in eyes than in open angle. Therefore, narrow angle of anterior chamber appeared to be a risk factor for intra ocular hypertension.
5.Increase in intraocular in study group was more among females (100%).
Recommendation
Initial evaluation of angle of anterior chamber and intraocular pressure and regular follow up monitoring of intraocular pressure is recommended in COPD patients receiving Tiotropium metered dose inhalers. This would possibly apply to DPIs as well.
References
1. Akhtar MA, Latif PA. Prevalence of chronic bronchitis in urban population of Kashmir. J Indian Med Assocl 999; 97 : 365-6.
2. Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV. TheLung health Study. JAMA 1994;272(19):1497505.
3. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE. et al. The effects of smoking cessation intervention on 14.5 year mortality: a randomized clinical trial. Ann Intem Med 2005;142(4):2339.
4. Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis 1986;133:14-20.
5. Augusti A, Farer R: Systemic inflammation and comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2012; 9 : 43 – 6.
6. Bestall, JC, Paul, EA, Garrod, R, et al Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 999;54,581-586.
7. Brreintos F, Jimenez SM, Delacasa M JM, Hernandez MC. Acute angle-closure glaucoma resulting from treatment with nebulised bronchodilators. Garcia-Feijoo J 2006;81(11):657-60.
8. Brusasco V, Hodder B, Miraitles M, Korducki L, Towse L; Kester S.: Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salnetherel in patients with COPD: Thorax 2003 May; 58(5) ; 399 – 404.
9. Chhabra SK, Rajpal S, Gupta R. Patterns of smoking in Delhi and comparison of chronic respiratory morbidity among beedi and cigarette smokers. Indian J Chet Dis Allied Sci 2001; 43 : 19-26.
10. Dada T, Konkal V, Tondon R, Sihota R: Comeal toperlapin response to TOP reduction is steroid induced Glaucoma with VKC Eye 2005, 5 : 122 – 29.
11. Devereux, Graham (May 2006). "ABC of chronic obstructive pulmonary disease. Definition, epidemiology, and risk factors". BMJ 332 (7550): 1142–4.