Natural Tooth Pontic: An Immediate Interim Restoration
Natural Tooth Pontic: An Immediate Interim Restoration
Arun Vashisht *1, Navjot Singh2, Kavneet Kaur Pelia3
1.BDS, MDS, PG Prosthodontics, Director GimmeSmile PPLC, Texas, North America
2. BDS, Genesis Institute of Dental Sciences and Research, Ferozepur, Punjab, India.
3. BDS, Dr. Harvansh Singh Judge Institute of Dental Sciences and Hospital, Chandigarh, India.
*Correspondence to: Arun Vashisht, BDS, MDS, PG Prosthodontics, Director GimmeSmile PPLC, Texas, North America.
Copyright
© 2022 Arun Vashisht. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 Dec 2022
Published: 15 Dec 2022
Abstract
The loss of anterior teeth can be psychologically and socially damaging to the patient. Restorations can vary between removable prosthesis, tooth-supported prosthesis, or implant-supported prosthesis. Irrespective of the final treatment, the first line of treatment would be provisionally restoring the patient’s esthetic appearance while functionally stabilizing the compromised arch.
Keywords: Pontic, Restoration, Prosthesis, Esthetics.
Natural Tooth Pontic: An Immediate Interim Restoration
Introduction
Fortuitous tooth loss in esthetic zone of the anterior region can be due to trauma, periodontal disease or endodontic failure.1 Following the tooth loss exigent need for replacement arises, in order to avoid aesthetic, masticatory and phonetic difficulties and to maintain the edentulous space.2
Conventional solution to this clinical problem has been the provision of single tooth, removable temporary acrylic prosthesis or resin-bonded bridges; each having their specific merits and demerits in terms of usage, aesthetics, and compatibility. 3,4 Analyzing various pros and cons, a treatment module is decided upon by the dentist in consonant with the patient. Using natural teeth as a pontic benefits of being right size, shape and color. Moreover, the positive psychological impact on the patient in using his or her natural tooth is an added benefit.2 The present case reports the utilization of an avulsed tooth as a natural tooth pontic.
Case Report
A 34-year-old healthy female patient reported at department of Periodontology and Oral Implantology with a complaint of highly mobile tooth in the lower left region of mouth. Clinical and radiographic findings stipulated it as generalized chronic periodontitis (Fig- 01).
Figure 1: PAN IMAGE
The concerned tooth was lower left first premolar and grade III mobile. 5 It was indicated for extraction. Scaling and root planing was done, and the patient was recalled after 3 days for extraction. The patient’s tooth got avulsed very next day and she reported back with avulsed tooth. Considering the patient’s request for immediate prosthesis, the idea of natural tooth pontic was proposed. The patient agreed to it and a written signed consent was obtained from her.
Technique:
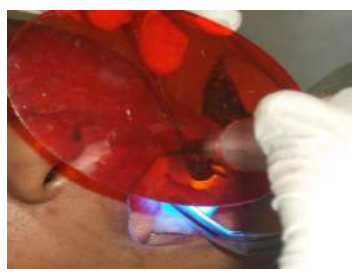
The apical opening of the pulp canal was cleaned, slightly enlarged, and sealed with resin composite. A modified ridge lap design was given to cervical area to facilitate cleaning and appearance of emerging profile. The apical portion of the root was removed to facilitate proper positioning of the tooth in an edentulous area. Intracoronal round 0.001” braided wire was inserted into the prepared tooth and bonded with composite. It was then bonded to the adjacent teeth using light cure composite. Finishing and polishing procedures were carried out using composite finishing discs and stones (Fig 02 - 05).
Figure 2 : Missing tooth
Figure 3 : Try in of Natural Pontic
Figure 4: Composite (Ribbond) Application and Curing
Figure 5: Natural tooth Pontic in Place
Oral hygiene instructions were given to the patient. The first recall appointment was made after 1 week. The patient’s sanguine countenance was result of the achieved desired esthetics improved ease of biting without any discomfort.
Discussion
The restoration of a smile is one of the most appreciating and gratifying services a dentist can render. Psychological and social trauma to the patient can be prevented by immediate replacement of lost tooth. Replacement can be provisional, semi provisional, or permanent in nature. Final restorations can vary between removable prosthesis, tooth supported prosthesis or implant-supported prosthesis. Irrespective of the final treatment, the first line of treatment would be to provisionally restore the patient’s esthetic appearance while functionally stabilizing the compromised arch.
Removable appliances or prostheses seem to be one suitable treatment opinion, but patient compliance is generally a major problem. Moreover, the clasps incorporated into removable partial denture can compromise esthetics. Removable partial denture is susceptible to fracture. In this regard, Natural tooth pontic may offer several advantages over removable appliances including enhanced esthetics, ease of use and avoidance of becoming accustomed to a removable prosthesis.6,7
The patient’s natural tooth can be used as a pontic which effaces the need of complicated laboratory procedures. The major advantage of retaining patient’s natural crown is that it instigates the patient to better tolerate the effect of tooth loss. 8 Natural tooth acts as an optimal pontic in terms of size, shape, and color.
In present case, natural tooth pontic was shaped as modified ridge lap pontic with a well-polished and smooth, convex surface that results in pressure free9 or mild contact with alveolar ridge for better preservation of soft tissue health10.
Albeit this technique demands increased chairside time; the key advantages are:
- excellent esthetic results
- preservation of natural crown structure
- extracted tooth can be replaced at the same visit.
- no laboratory work required.
- reduces psychological impact on the patient.
- technique is reversible and allows other restorative options to be available.
- can be used as interim or definitive prosthesis.
- Micro-resiliency of pontic allows stimulation of underlying tissue and avoids excessive ridge resorption. 2
Conclusion:
Natural tooth pontic offers a simple and cost-effective treatment option for replacement of a fractured or avulsed tooth. It can prove to be very hygienic; noninvasive and long-term provisional treatment providing preeminent esthetics and function if consummated proficiently. However, this procedure demands appropriate case selection and precise technique.
References
1. NathansonD, Moin K. Metal-reinforced anterior tooth replacement using acid-etch-composite resin technique. J Prosthet Dent. 1980,43(4):408-412.
2. Pariola A, Shenoy KM, Thomas MS, Mohan M. Use of a natural tooth crown as a pontic following cervical root fracture: A case report.
3. Ashley M, Holden V. An immediate adhesive bridge using the natural tooth. Br Dent J 1998; 184:18-20.
4. Safirstein JJ, Owens BM, Swords RL. The resin retained natural tooth pontic: a transitional esthetic solution. J Tenn Dent Assc 2001;31-33.
5. Miller SC. Textbook of Periodontia. Philadelphia: The Blakiston Company; 1950:125.
6. Fahl N. Restoration of the maxillary arch utilizing a composite resin build up and a fiber framework. Pract Periodontics Asthetic Dent 1998; 10:363-367.
7. Smidt A. Esthetic provisional replacement of a single anterior tooth during the implant healing phase: a clinical report. J Prosthet Dent 2002;6: 598-602.
8. Stein RS. Pontic-residual ridge relationship. Research report. J Prosthet Dent 1996; 16:251-285.
9. Edelhoff D, Spekermann H, Yildirim M. A review of esthetic pontic design options. Quinitessence Int 2002; 33: 736-746.