Theoretical Grounding for the use of Nanostructured and Nanomodified Carbon-Containing Coatings of Polymer Surfaces of Materials of Polymer Products, Widely used in Medicine and Biology.
Theoretical Grounding for the use of Nanostructured and Nanomodified Carbon-Containing Coatings of Polymer Surfaces of Materials of Polymer Products, Widely used in Medicine and Biology.
Alvina D. Musina*
*Correspondence to: Alvina D. Musina Senior Scientist, MD, Moscow Eugene E. Sidorenko, Prof, PhD, Head of the Dept of scientific- practical center.
Copyright
© 2024 Alvina D. Musina. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 March 2024
Published: 01 May 2024
Theoretical Grounding for the use of Nanostructured and Nanomodified Carbon-Containing Coatings of Polymer Surfaces of Materials of Polymer Products, Widely used in Medicine and Biology.
Abbrevations:
TCL – Therapeutic Contact Lenses
SCL – Soft contact lenses
CCF – Carbon-Containing Film
PET – Polyethylene Terephthalate
PTFE – Polytetrafluoroethylene
PVDF – Polyvinylidene fluoride
NSS – Nano Structurization of the Surface
NMS – Nanomodification of the Surface
Introduction
The trend of using disposable products in medicine, biology and everyday life for hygienic purposes was justified by the achievements of scientific and technological progress in obtaining new materials, in finding ways to comply with sanitary and hygienic requirements for various auxiliary products; everywhere, in addition to modern medicine and biology, various polymeric devices, primarily for the purpose of preventing bacterial complications.
However, paradoxically, the massive use of various polymer products, especially disposable ones, usually for hygienic purposes, has caused and continues to cause the manifestation of another, no less dangerous problem - Infections caused by microbes originating from biofilms, which certainly form on any polymer surfaces, especially on polymer surfaces of products made from cheap and readily available polymer materials. It is also known that polymer films can be quite successfully used in biological laboratories for the cultivation and selection of various microorganisms. The formation of microorganisms from biofilms on polymer surfaces has become such a formidable complication that it has become a separate nosologically class of diseases “caused by microbes from biofilms.” A solution to this problem was possible by selecting a different, more expensive polymer starting material or by treating the surface of the polymer to impart the desired physicochemical properties to the surface of the safe polymer product.
To ensure the compatibility and biocompatibility of various products made of polymer materials in contact with living tissues or tissue fluids, as well as to prevent the formation of biofilms on the surface of polymers, since the late 90s we have been developing various methods for modifying the polymer surface of polymer products, which are being developed, in particular, using nanotechnologies for processing polymer surfaces NSS&NSM (Nanostructurization and Nanomodification), for subsequent processing of polymer surfaces previously prepared in this way by applying carbon-containing films, for example, diamond-like films, nanotubes, fullerenes, onto an the already pre-treated polymer surface. In addition, carbon-containing films, as shown by the results of experimental studies, have pronounced adhesion to polymer surfaces under certain technological conditions aimed at improving the proper quality of polymer surfaces.
Various packaging materials and systems used in biology, medicine and made from synthetic polymeric materials, for example drainage tubes, catheters, etc., must have a certain set of properties, including: biocompatibility, in addition to aseptic properties, antibacterial activity and, if necessary, providing the phenomenon of bioepitaxy, as well as other programmable characteristics of the processed polymer surface. These characteristics and properties of the treated surface, as already noted, can be achieved by treating the surface of polymer materials, selecting and combining a certain composition of the gas mixture for deposition on the treated surface in each specific case, as well as varying the technological modes of surface treatment. The properties of surfaces are determined by: the topography of the surface, its atomic composition and the charge on its surface, a change in which can subsequently change the qualitative characteristics of the surface.
The main quality that polymers selected for medical devices must have been compatibility. Biocompatibility, characterized by the absence of toxicity and effective functioning throughout the practical use of the polymer product. Toxicity is a complex of phenomena that occur in vivo, which may include: direct cell damage, for example, cytotoxic effects or physiological effects (inflammatory and allergic reactions, etc.). These properties are difficult to study in a system, so most researchers’ base toxicity determinations on data from cell culture studies. The study of the cytotoxicity of various materials comes down to the analysis of cell culture parameters such as cell survival and growth: determination of metabolic activity or regenerative potential of cells and cell mass. To do this, it is necessary to focus on the growth curve of a cell culture in the presence of the material or substance being studied, the construction of which is individual in each specific case.
According to numerous previous studies, implantation of any foreign material, including biological tissues, into the tissues of another organism causes an inflammatory and reparative response, leading to the activation of fibroblast proliferation, the formation of new collagen fibers and other components of the extracellular matrix tissue and, as a result, the formation of connective tissue capsules around the implant. When a foreign material is introduced into the thickness of biological tissue, immediate adsorption of a thin layer of proteins occurs on its surface.
The implanted polymer, due to the initial attraction of polymorphonuclear cells and monocytes, becomes the main object of the reaction at the interface polymer-tissue. During the spectral analysis of the composition of the protein layer on the surface of the implant, it was found that this layer consists of 6 main proteins: albumin, fibronectin, transferrin, fibrin/fibrinogen, immunoglobulin and C3 fraction. The presence of these components on the surface of the implant changes its adhesive properties and leads to greater cell adhesion. Activation of cell adhesion to material located deep in the stroma leads to the formation of a capsule around it. In studies by Zavala E. et al (1984), it was found that the thickness of the capsule formed around a foreign body is a relative indicator of biocompatibility.
The placement of any foreign material into the thickness of the living tissue causes a response from the body. However, it is necessary to distinguish the development of tissue response to surgical trauma, which most often follows the type of inflammation with changes arising from the presence of the material. Restoration of tissue integrity after surgical trauma occurs within two weeks and ends with healing and the passage of all stages of inflammation. The result is the formation of scar tissue, which occurs due to the response of fibroblasts, macrophages and collagen formation. Only after a certain period of time can it be stated that the residual inflammatory reaction was caused directly by the presence of material in the tissue.
All biomaterials can be divided into toxic, practically inert, inert and biodegradable.
An ideally biocompatible material does not exist and cannot exist by definition.
A minor tissue reaction will manifest itself one way or another, and the occurrence of cell adhesion and, as a consequence, the formation of a capsule will depend on the surface properties of the implant itself: surface quality, atomic composition, degree of surface charge, its hydration, quality of surface treatment. The foreign body is usually rejected, destroyed, or encapsulated, depending on the surgical procedure and the health level of the recipient. A material is considered toxic if its chemical composition or substances in the material degrade or are leached from the implant in the body, causing toxic effects on cells and living tissue in general. Such materials are unacceptable for the production of biological implants.
Depending on the nature of the capsule formed around the foreign body, materials are divided into practically inert, when the defined capsule is thin and does not adhere to the surface of the implant, inert, in which the capsule is absent, or very thin and bioactive, in which the adjacent capsule is defined.
When biodegradable materials remain in body tissue for a long time, they dissolve and the material itself is replaced by human tissue; it is important that the dissolution products are non-toxic
We have used carbon-containing films to treat the polymer surface of medical products and products for their safe use in the future in medical practice and biology.
All natural materials and systems are built from nano-objects. It is in the Nano range, at the molecular level, that nature determines the main characteristics of substances, as well as their phenomena and processes. Features of the properties of substances and materials in the nanometer range are determined not only by a decrease in the size of structural elements, but also by the manifestation of quantum mechanical effects, the wave nature of transfer processes and the dominant role of interfaces. By controlling the size and shape of nanostructures, it is possible to impart completely new functional characteristics to materials, significantly different from the characteristics of bulk materials. In addition, in a number of special cases, NSS (nanostructurizated surfaces) must have special physicochemical or chemical properties, for example, biodegradability, or special strength, or flexibility, or have a porous structure for the formation of intercellular substance (matrix).
Four chemical elements are present most of all in the cells of living organisms and in the following proportions and greatest volume:
oxygen – from 65 to 70%;
carbon – from 15 to 18%;
hydrogen – from 8 to 10%;
nitrogen – from 2 to 3%.
Carbon is a solid substance with an atomic crystal lattice. The carbon molecule is monatomic; this substance has the largest number of allotropic modifications (more than 9 have been discovered to date).
A neutral carbon atom has six electrons. Two of them are located near the nucleus and form the first layer (1s state). The next four electrons form the second electron layer. Two of the four electrons are in the 2s state and the other two are in the 2p state. The neutral carbon atom in the ground state is divalent and has an electron-graphic configuration 1s22s22?2.
Despite the presence of two unpaired electrons in the outer level, carbon is tetravalent in most chemical compounds. Carbon acquires the ability to form four bonds when one electron passes from the 2s state to the 2p state - “pairing” occurs, that is, the transition of the carbon atom from a neutral to an excited state. This excited state of the carbon atom corresponds to the electronic configuration 1s22s12p3.
In a crystal lattice, carbon atoms are linked by covalent chemical bonds. The distance between all atoms is the same, so the bonds are strong in all directions.
Carbon exists in many allotropes with very diverse physical properties. The variety of modifications is due to the ability of carbon to form chemical bonds of different types.
Depending on the formation of modifications, two types of carbon are distinguished:
Crystalline carbon is part of solids (diamond, graphite, graphene, fullerene, carbyne). Amorphous carbon forms soft substances (coal, coke, soot).
Recently, we have seen advances in the field of nanotechnology, which arose and developed at the intersection of sciences.
The use of nanotechnology in medical and clinical practice, in addition to knowledge in the field of cell membrane physiology, molecular biology and regenerative medicine, requires fundamental knowledge, for example, in physics, chemistry, physical chemistry, materials science, chemical synthesis.
In the course of research on the topic “Polymer surface treatment” at the Tissue Bank of the Russian Center for Eye and Plastic Surgery (Ufa), we turned to achievements in the field of application of advanced nanotechnologies in medicine, namely in ophthalmology. As part of a joint project with the Department of High Technologies of MATI and the Department of Radio Electronics of Moscow State University, we have developed various technologies for producing NSS&NMS with different physical and chemical properties of the processed polymer. surface. The results obtained made it possible to initially develop and create a container for long-term aseptic storage of contact and intraocular lenses (RF patent No. 2120807; 10/27/1998, A.D. Musina).
Ensuring aseptic storage applies to almost all medical items. Therefore, preliminary research results showed that the resulting aseptic containers for storing polymer products (IOLs, CLs) could also be successfully used for transplantology, providing aseptic storage, as well as, the prolongation the shelf life and safe transportation of the different grafts, alloplants, viable donor tissues.
Based on the data presented, we formulated the goal of improving the method of prolonged storage of allogeneic transplants of appropriate quality by storing them in special containers or using film polymer packaging materials with carbon-containing NSS&NMS coatings on their surface, which would ensure guaranteed safe and reliable storage of various grafts, especially during their transportation.
Firstly, the effects that arise on the NSS&NMS polymer surface were studied when their polymer surfaces were treated with flows of particles of inert and chemically active gases and their mixtures, as well as when carbon-containing films were applied to their polymer surfaces. The effect of NSP on underlying biological tissues, including various allografts and donor materials, including donor cornea, has also been studied. Experimental studies were carried out on polymer materials: polyethylene terephthalate (PET), polytetrafluoroethylene (PTFE) and polyvinylidene fluoride (PVDF) with NSP obtained using ion-plasma surface treatment technology. Studies have shown that the chemical composition, charge of the surface under study, the degree of its dispersion and the method of its modification determine the presence and effectiveness of the achieved antibacterial activity of the treated polymer surface, as well as their biocompatibility and adhesiveness. polymer surface using NSS&NMS
It has been established that the application of carbon-containing films by ion-plasma methods in various processing ranges makes it possible to control the charge characteristics on the surface of polymers used in the manufacture of containers and packaging material for storing allografts and donor materials. It has been shown that the biocompatibility of carbon films is directly proportional to the magnitude of the electrostatic potential, and the antibacterial activity is determined by the structure and topography of the treated surface.
Thus, for the first time, a system was developed and proposed: donor tissue - nanomodified, biocompatible, aseptic surface - nutrient medium (if necessary), which, according to research results, is a more advanced dynamic model for storing viable donor material (donor cornea) compared with existing methods for preserving viable allografts.
Our work was preceded by the receipt, in addition to the results of microbiological studies, primarily of convincing and substantiated results of experimental work carried out on experimental animals.
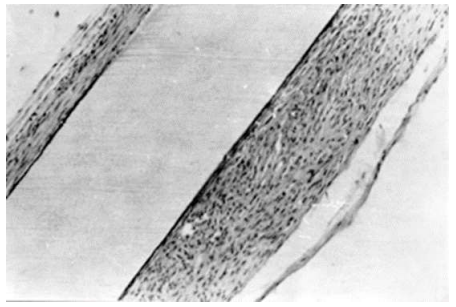
Thus, when investigating, for example, the adhesive properties of the surface of a nanomodified polymer during experimental studies, the results of “in vivo” experiments with the implantation of polymer strips treated with applied carbon-containing film (CCF) were obtained. The results of the experiment showed that 4 months after implantation of the strip treated by applying a carbon-containing coating (CCF) to its surface, connective tissue in the form of a capsule began to form around the implant plate with the treated surface, as shown in Fig.1
Fig. 1. Capsule formed around a fluoroplastic plate coated with a carbon film 4 months after subcutaneous implantation of a mouse.
Thin (a) and multilayered (b) sections of the capsule.
Magnification x 60
A capsule around the implanted fluoroplastic plate coated with CF began to form 4 months after its subcutaneous implantation in mice. Thin (a) and multilayer (b) sections of the capsule. An increase in X60 a b is a standard reaction to the biocompatibility of the implant; its thickness around the same plate varied significantly: in some areas the capsule was thin (no more than 2-4 rows of cells), in other places it looked multilayered (Fig. 1). Thin sections of the capsule consisted of young, poorly differentiated fibroblasts, sometimes in direct contact with the surface of the plate; Thin collagen fibers were found between the cells. In thick sections of the capsule, three layers can be distinguished: the inner layer (immediately adjacent to the plate), morphologically similar to the thin sections of the capsule described above; a middle layer consisting of mature fibroblasts and collagen fibers oriented parallel to the surface of the plate; the outer layer consists of fibroblasts of varying degrees of maturity and loosely arranged collagen fibers. In no case was leukocyte infiltration observed, indicating the absence of an inflammatory reaction. The described morphological picture of the capsule structure was similar in all implanted plates. Experimental studies conducted on the surface of PET, PTFE, PVDF polymers with NSS&NMS surfaces obtained using ion-plasma technology for processing the polymer surface showed that the degree of surface dispersion and the method of its modification determine the presence and effectiveness of the resulting surface characteristics, in particular: biocompatibility, antibacterial activity, lack of toxicity, presence of a developed surface with good adhesive properties for living cells. Research on nanostructured surfaces (NSS) has revealed phenomena such as tracking, correction, design and control of biological systems at the molecular level.
Biocompatibility is the ability of a synthetic material, in our study, for example, to integrate into another living organism without causing adverse clinical manifestations or reactions in the living tissues of the recipient, which is necessary to achieve an optimal therapeutic effect. Previously, the term "Biocompatibility" was used in the context of implantable devices for long-term clinical use. Initially, the main requirement for materials was safety, which was achieved due to their chemical and biological inertness. The materials had to be non-toxic, non-carcinogenic, non-allergenic, non-thrombogenic, etc. This list of missing properties defined the concept of biocompatibility. It was understood that materials of this type included metal alloys based on titanium and platinum, as well as polymers based on polyethylene and silicone.
Today, the complexity of treatment methods, especially surgical ones, is increasing, as is the expectation of better results from surgical interventions. Thus, the use of various artificial materials has led to the realization that the implanted material will be forced to interact with a living organism, and not simply “not be perceived” by the surrounding living tissues of the recipient. To ensure effective engraftment, it is necessary that the material induces a specific, controlled and regulated response in the living tissue surrounding the graft. The achievements in this area are significant. An example of a bioactive material is ceramic Nano coatings of bone replacement implants, which can induce bone formation. Finally, safe resorption of the material and its replacement with natural tissue is important for many applications such as various suture material and orthopedic implants.
Biocompatibility of polymer materials
The main quality by which polymers could be selected for medical products should have been biocompatibility, characterized by the absence of toxicity and effective functioning throughout the entire period of use. Toxicity is a complex of phenomena that occur in vivo, which may include: direct damage to cells of cytotoxic action and physiological effects (inflammatory and allergic reactions, etc.) It is quite difficult to study these properties in a system, so most researchers determine toxicity using cell cultures as an example. The study of the cytotoxicity of various materials comes down to the analysis of cell culture parameters such as cell survival and growth: determining the metabolic activity or regenerative potential of cells and cell mass. To do this, it is necessary to focus on the growth curve of a cell culture in the presence of the material or substance being studied, the construction of which is individual in each specific case.
According to the results of many previous studies, implantation of any foreign material and, in some cases, especially biological tissues, into the recipient’s body tissue causes an inflammatory-reparative reaction, leading to the activation of fibroblast proliferation, the formation of new collagen fibers and other components of extracellular matrix tissue and, as a consequence, the formation of a connective tissue capsules around the implant.
When a foreign material is introduced into the thickness of biological tissue, immediate adsorption of a thin layer of proteins occurs on its surface. The implanted polymer, due to the initial attraction of polymorphonuclear cells and monocytes, becomes the main object of the reaction at the polymer-tissue interface. During the spectral analysis of the composition of the protein layer on the surface of the implant, it was found that this layer consists of 6 main proteins: albumin, fibronectin, transferrin, fibrin/fibrinogen, immunoglobulin and C3 fraction. The presence of these components on the surface of the implant changes its adhesive properties and leads to greater cell adhesion. Activation of cell adhesion to material located deep in the stroma leads to the formation of a capsule around it. In studies by Zavala E. et al (1984), it was found that the thickness of the capsule formed around a foreign body is a relative indicator of biocompatibility.
Biocompatible NSS&NMS assumes a certain chemical composition, atomic structure, charge on the surface and is capable of providing the effect of polarization of cell membranes, the shape and functioning of living tissue cells when they come into contact with NSS&NMS - interface interaction - (for example: avascular structure of corneal tissue - NSS&NMS). The development of the “Method for preserving the donor cornea” was a continuation and generalization of the previous ones, based on the study of already accumulated data from theoretical and experimental research in this field of knowledge, issued in the form of scientific publications and Patents.
Method of allogeneic implants, donor tissues storage and secure transporting; using the example of donor cornea aseptic storage and safely transportation in a special polymeric container which surface is treated by means of surface Nanomodification. 06/28/2017, Russian Patent (RU Patent 28.06.2017; RU 2690153 C2)
So, the development and implementation of a “Method for preserving viable cells of a donor cornea” was proposed, which was fully justified theoretically and in the course of experimental studies and was not accidental; The results of these studies further expanded and deepened the study of the possibilities of using the proposed method using NSS&NMS on other biological tissues. The choice of corneal tissue in our study was also due to the fact that the cornea is a living tissue formed from 3 germ layers: endothelium, stroma and epithelium; These are the layers of the body of a multicellular embryo, formed during the process of gastrulation and giving rise to various organs and tissues, which in subsequent studies will allow further investigations and development in order to expand the possibilities for development the successful use of NSS&NMS of the polymer surfaces in other areas of Medicine and Biology Applications.
Polymer materials with NSS&NMS represent a separate class of synthetic nanomaterials. NCC&NMC treatment is necessary on the surface of implants and cell culture matrices, especially when they are introduced, for example, into the skeletal system; for the creation of drugs and therapeutic systems for external use, in particular transdermal forms that provide drug delivery through the skin; for the formation of matrices for internal targeted delivery of drugs (Stillman M., 2002; Sevastyanov V.I., 1999).
The study of the basic physicochemical characteristics of aseptic carbon-containing coatings applied using nanotechnology for the treatment of polymer surfaces was carried out after studying the antibacterial and adhesive properties of nanostructured coatings and their toxicity.
A comparative morphological analysis of native transplants was carried out using the example of a donor cornea using various preservation methods. For example, as a result of a morphological study of the donor cornea material, it was found that after storing the donor cornea for 1-2 days, the quality and quantity of endothelial cells (EnC) of the donor cornea (DC), as well as the Main indicator of the qualitative state of the DC and suitability for further transplantation, are significant. No morphological changes were detected regardless of the research method and storage conditions: type of preservation medium, duration and temperature of storage of the donor cornea. Pathological morphological changes began to be detected on the 4th day of storage of the donor cornea in a moist chamber and on the 5-6th day of storage in Eagle's medium.
In special containers, in preservative media Optisol, Dexol, donor corneas were stored at a temperature of 25-27°C, maintaining the proper quality of the donor cornea for up to 18 days. Encouraging results were obtained when storing the donor cornea in a special container with donor blood plasma. The donor cornea retained its structure: preservation of the apical and, more importantly, lateral borders of the EC for more than 20 days. As is known, the state of the lateral boundaries of EC cell membranes is of great importance for the mechanism of fluid transport through EC (J. Fitchburg, 1997), indicating the viability of the preserving tissue.
The study of the basic physicochemical characteristics of aseptic carbon-containing coatings applied using nanotechnology for the treatment of polymer surfaces was carried out primarily by studying the antibacterial and adhesive properties of nanostructured coatings and testing their toxicity.
Thus, the system parameters: preserved viable tissue - nanostructured surface, were optimized
Many articles are devoted to therapeutic contact lenses (TCLs) and bandage contact lenses (BCLs). As well as articles about the prospects of wearing conventional SCLs, which have a number of undeniable advantages in correcting refractive errors of the eye, for which SCLs were originally invented. Nevertheless, complications associated with the use of random SCLs instead of TCLs and BCLs are well known. For example, in the postoperative period, after corneal surgery, especially after corneal cross-linking (CLS surgery), when the use of TCL and BCL is indicated for all patients who have undergone this corneal surgery. Unfortunately, traditional SCLs are still used instead of TCL and BCL. When the untreated surface of the SCL polymer material comes into contact with the surface of an operated or damaged cornea, microbial contamination can occur even within the first hours of contact. After all, it is common knowledge that polymer films are widely used as polymer substrates in laboratories, for example, for seeding, culturing and growing microorganisms. Hemodialysis is also carried out through a polymer film, as trough porously barrier.
The proposed modern achievements in the field of high technology, as well as in the production of new materials, including composites, as well as nanomodification of the surface of polymer materials with specified surface properties, make it possible to obtain biologically active systems, which today are only possible with the use of nanotechnology. The use of biologically active systems opens up new prospects in the development of certain areas of medicine, makes it possible to treat and prevent unwanted, but possible postoperative injuries and damage to the cornea, which can lead to complications, for example, after popular refractive surgeries, cataract extraction, corneal cross-linking procedures and other interventions in the anterior segment eyeball. Therefore, it appears that the most promising contact lenses currently available in corneal rehabilitation are those with NMPS (nano-modified polymer surface) lenses. Having different natures and origins, epithelial and stromal cells of the cornea change their shape and functional activity differently depending on the characteristics of the extracellular matrix, its biochemical properties and geometric configuration. The biochemically mediated adhesive properties of the matrix and its Nano relief are the determining and orienting centers that determine the direction of the cell migration vector, the concentration of certain types of cells in the regeneration zone, as well as the regulation of cell proliferation and their further development, as well as functional activity. Cells have a unique ability to sense surface curvature and the size of micro-irregularities in nano-sized units, to which a living cell reacts, the size of which is incomparable to micro-irregularities. Nanoscale topography is the fundamental rationale for modulating cell behavior on surfaces. Since topography can be modified to either stimulate or suppress specific cell behaviors, improving its implementation requires the development of a specific target nanomodified surface, its application, and the study of such interface, for example, to understanding corneal cell interactions and interactions. the structure of the extracellular matrix, which opens up new opportunities for understanding, monitoring and treating the cornea both in a healthy state and at various stages of pathological changes in the cornea.
Thus, the safety of the eyeball of SCL users from bacterial contamination can be ensured by maintaining hygiene and using SCLs made either from expensive high-quality polymer, which is unprofitable, or by using nanotechnology to treat the polymer surface of polymer products, otherwise Lenses made of porous polymer material can easily become infected with bacterial colonies, which leads to the inevitable formation of a biofilm on the surface of SCL, as well as on the polymer surface of aseptic containers for their storage. The successful use of BCL, TCL for preventive and therapeutic purposes, for example, during the period of postoperative rehabilitation of patients who have undergone surgery on the anterior segment of the eyeball, can provide a successful prospect for early corneal restoration. Equally important is the creation of an empirically modeled aspherical shape of the SCL, as close as possible to the shape of the native cornea, considering the topographic properties of the surface relief of the SCL, taking into account the structure and nature of migration of living corneal cells under and along the inner surface of the SCL, providing for the so-called “topographic reactions of living cells” on the properties and topography of a particular surface.”
There is a need to create the due quality for TSL and BL, replicating the shape of the cornea with a qualitatively improved nanomodified surface for therapeutic purposes.
To summarize, it can be noted that the presented work highlights issues of theoretical justification for the use of nanotechnology in the processing of polymer surfaces of various polymer products, widely used in medicine, biology and simply in our everyday life, are covered. The chemistry and structure of polymer products, the effect on their polymer surface of deposition, for example, composite films formed in the gas phase, under various surface treatment modes, thus determining the specified chemical properties of the treated surface, are presented in detail.
References
1. Journal of MAR Ophthalmology (Volume 5 Issue 5) Citation: Alvina D. Musina, “Therapeutic Contact Lenses with A Nanomodified Surface for Corneal Rehabilitation After Donor Corneal Transplantation or other Eye Surgery Interventions on the Anterior Segment of the Eyeball” MAR Ophthalmology, Volume 5 Issue 5
2. Journal of MAR Ophthalmology (Volume 5 Issue 5) Citation: Alvina D. Musina, “Containers and Various Packaging Devices Made of Polymeric Material for Storage of Allogeneic Grafts, the Surface of Which is Treated by Applying Carbon-Containing Nanofilms to their Polymeric Surface.
3. Journal of MAR Ophthalmology (Volume 6 Issue 1) Preservation Conditions of Donor Cornea Ensure its Proper Quality, As Optical Characteristics and Biocompatibility Citation 1. Alvina D. Musina 2. Eugene E. Sidorenko 2 1. Senior Scientist, PhD, Ophthalmologist, Moscow. 2. Prof, PhD, head of the Dept. of Scientific-Practical Center, Moscow
4. Journal of MAR Ophthalmology (Volume 6 Issue 1) Artificial Iris Surface Modification by Means of Carbon Film Deposition for Providing the Eye Diaphragm Loss Compensation Alvina D 1 *, Eugene E
5. Journal of MAR Ophthalmology and Ocular Therapeutics, (Volume 7 Issue 1) Modern Therapeutic Contact Lenses with a Nanomodified Surface, Offered to Shorten the Effective Rehabilitation Period of the Restoring the Anatomical Structures of the Anterior Segment of the Eye Ball and its Visual Functions. Biocompatibility Citation 1. Alvina D. Musina 2. Eugene E. Sidorenko 2 1. Senior Scientist, PhD, Ophthalmologist, Moscow. 2. Prof, PhD, head of the Dept. of Scientific-Practical Center, Moscow
6. Journal of MAR Ophthalmology and Ocular Therapeutics, (Volume 6 Issue 6) Modern Therapeutic Contact Lenses with a Nanomodified Surface, Offered to Shorten the Effective Rehabilitation Period of the Restoring the Anatomical Structures of the Anterior Segment of the Eye Ball and its Visual Functions.
6. Patent (RU Patent 06/28/2019; RU 2690153 C2) A method for storing and safely transporting allogeneic implants using the example of aseptic storage and safe transportation of the donor cornea in a special polymer container, the surface of which is nano-modified.
7 th Euro BioMat 2021 Presentations:
7. The relief of surface migration determines the structure and behavior for each moving living cell
8. THE EYE DIAPHRAGM LOSS COMPENSATION BY MEANS OF ARTIFICIAL IRIS USE
9. The allogeneic transplants preservation
10. Dissertation “Ensuring prolonged aseptic storage and transportation of the high-quality donor cornea”, 2006