Ectopic Trantas Nodules
Ectopic Trantas Nodules
Yonli yempabou Hugues Arnaud1, Lucrèce Joanelle Vydalie Eriga, Fadhloullahi Khidrou Sambou Oumarou, Djibril Adéotin Yaya-Oye,Yassine Mouzari, Abdelbarre Oubaaz
*Correspondence to: Yempabou Hugues Arnaud Yonli, Moracco, Department of ophthalmology,Hôpital militaire d’instruction Mohammed V-Rabat, Morroco.
Copyright
© 2024 Yempabou Hugues Arnaud Yonli. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 March 2024
Published: 01 May 2024
Ectopic Trantas Nodules
The patient was 11 years old, with a history of chronic allergic conjunctivitis, untreated or poorly treated, who consulted us because of tingling and the discovery of ocular nodules.
On clinical examination, visual acuity was preserved at 10/10 in both eyes, with no ocular redness.
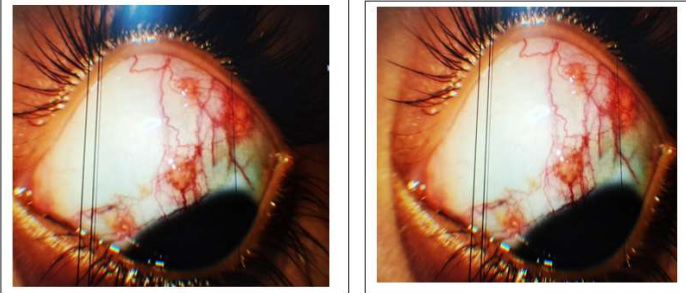
The adnexa showed healthy eyelids, papillae in the tarsal conjunctiva and scattered Trantas nodules in the bulbar conjunctiva. No conjunctival fibrosis was found.
Examination of the anterior segment was unremarkable.
The fundus was normal in both eyes.
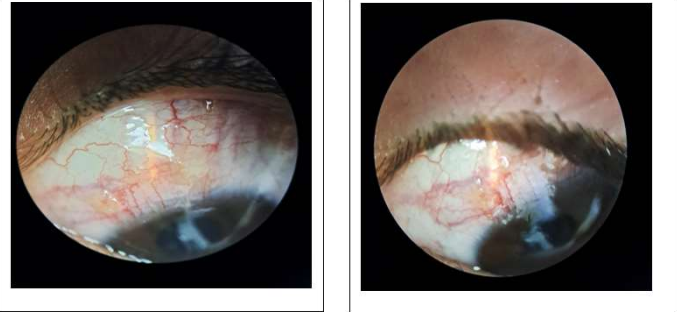
Treatment consisted of a combination of antihistamines and corticoids. The evolution was marked by a reduction in nodules and an improvement in the patient's comfort.
Figure 1: ectopic nodules
Figure 2: Nodule regression under treatment