Pulmonary Embolism in a Neonate Following Endovascular Intervention of a Vein of Galen Aneurysmal Malformation.
Pulmonary Embolism in a Neonate Following Endovascular Intervention of a Vein of Galen Aneurysmal Malformation.
Mona Wahlers1, M.D., Rene Chapot2, M.D., Cornelius Deuschl3, M.D., Carsten Müntjes4, M.D., Annegret Schnabel5, M.D., Sibylle Leichtl5, M.D., Ursula Felderhoff-Müser1, M.D., Mark Dzietko1*, M.D.
1Department of Pediatrics I, University Hospital Essen, University of Duisburg-Essen, Essen, Germany; TNBS, Centre for Translational Neuro- and Behavioral Sciences, University Hospital Essen, University of Duisburg-Essen, Essen, Germany;
2Department of Radiology and Neuroradiology, Alfried Krupp Hospital, Essen, Germany;
3Institute of Diagnostic and Interventional Radiology and Neuroradiology, University Hospital Essen, University of Duisburg-Essen, Essen, Germany;
4Department of Pediatrics III, University Hospital Essen, University of Duisburg-Essen, Essen, Germany; 5University Department of Obstetrics and Gynecology, Clinic St. Hedwig of The Order of St. John, University of Regensburg, Regensburg, Germany.
*Correspondence to: Mark Dzietko, Department of Pediatrics I, Division of Neonatology, University Hospital Essen, Hufelandstrasse 55, 45147 Essen, Germany.
Copyright
© 2024: Mark Dzietko. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 May 2024
Published: 03 June 2024
Abstract
Background: Vein of Galen aneurysm malformations are rare, cerebrovascular malformations with high rates of morbidity and mortality. VGAM in neonates usually present with high-output cardiac failure (HOCF) and endovascular intervention became the gold standard of treatment.
Case presentation: We report a term born infant with late prenatal diagnosis and respiratory distress after birth. Clinical deterioration progressed and endovascular treatment was performed. As a complication radiopaque embolic agents migrated to pulmonary arteries causing pulmonary hypertension with the clinical problem to differentiate between lung arterial embolism and HOCF. Management for pulmonary hypertension following endovascular treatment was initiated but challenging due to persistent elevated pulmonary pressure and the need for unusual management. At 4 month of age, secondary endovascular treatment was necessary and embolic agent was still detectable in both pulmonary arteries without clinical signs of pulmonary hypertension.
Conclusion: Side effects due to endovascular treatment can complicate management of neonates suffering from VGAM and HOCF requiring modification of standard treatment.
Keywords: Vein of Galen, AV Malformation, Pulmonary embolism, Endovascular Treatment, Newborn, Cardiac failure.
Pulmonary Embolism in a Neonate Following Endovascular Intervention of a Vein of Galen Aneurysmal Malformation.
List of Abbreviations
EF extraction function
EVT Endovascular treatment
PCA Posterior cerebral arteries PCA
HOCF High output cardiac failure
NICU Neonatal intensive care unit
DOL day of life
LMWH Low molecular weighted heparin
PFO Patent foramen ovale
PDA Patent ductus arteriosus
VGAM Vein of Galen aneurysmal malformation
Background
Vein of Galen aneurysmal malformation (VGAM) is a rare cerebral vascular anomaly accounting for 1 out of 25,000 deliveries with a predominance for males.1 In pediatric population, it is the most frequent arteriovenous malformation accounting for 30% of all vascular malformations.2 This high flow-low resistance malformation is characterized by the presence of multiple arteriovenous shunts, typically forming between the choroidal arteries and the embryonic precursor of the vein of Galen, known as the median prosencephalic vein of Markowski.3 This vein fails to regress between the 6th and 11th weeks of gestation.4 A genetic background has been identified, including mutations of RASA1 (RASp21 Protein Activator 1) and EPHB4 (Ephrin type-B receptor 4), genes encoding proteins involved in vascular development.5,6 In utero diagnosis is usually made in the third trimester and has increased to 73% with advances in antenatal ultrasound.7,8 Survival rate of neonates affected by VGAM is 60% when diagnosed prenatally but morbidity and mortality are still high despite a progressive, pathophysiological understanding of the disease and advances in treatment strategies.7 Endovascular treatment (EVT) including embolization and specialized management in neonatal intensive care has made VGAM a treatable and viable disease but the postnatal clinical course can be discrepant to antenatal findings making prediction of necessity and timing for intervention challenging.9 Prognosis is mainly influenced by cardiac and cerebral consequences. Up to 88% of newborns require an urgent embolization due to high output cardiac failure (HOCF), with high risk for morbidity and mortality.10-12 Here we report on a male neonate with late, antenatal diagnosis of VGAM, who underwent EVT on the second day of life. EVT consisted of transarterial embolization of macroshunts with a non-adhesive liquid embolic agent with the aim to reduce fistula volume of the VGAM. Further closure of the VGAM was planned in subsequent sessions. As a severe complication, perilous embolization of both pulmonary arteries occurred, which, to our knowledge has not been described in detail for the neonatal population yet.
Case Presentation
Following an uneventful pregnancy, VGAM and moderate ventriculomegaly was prenatally diagnosed by ultrasound at 39+6 weeks of gestation resulting in antenatal referral to our hospital. Incipient cardiomegaly with dilation of the right ventricle, mild tricuspid regurgitation, and an increased heart-to-thoracic volume ration (0,6) was already evident in fetal echocardiography. Diagnoses was confirmed 2 days after admission by fetal MRI as a type III VGAM using classification of Yasargil or choroidal type using classification of Lasjaunias with multiple fistulas between the posterior cerebral arteries (PCA) bilaterally, pericallosal arteries and the vein of Galen with the nidus being the ampulla of the vein of Galen.13,14 The VGAM was 6 x 2,5 cm in size, a detectable aqueduct of Sylvius with moderate dilatation of both lateral ventricles, no signs of ischemia or hemorrhages and mild brain volume reduction. Delivery with immediate postnatal intervention capabilities, was planned and a male child was born to a non-consanguineous couple after 40+2 weeks of gestation. The infant, weighing 3270 grams, was spontaneously delivered in a cephalic presentation. Initially, regular postnatal cardiorespiratory transition with an APGAR of 10/10/10 and normal arterial cord gases (pH 7,3). At 1 hour of life, the infant was admitted to our neonatal intensive care unit (NICU) for further work-up, monitoring and preparation for a possible endovascular intervention of VGAM. On the first day of life (DOL), due to persistent arterial hypotension, we administered a bolus of isotonic saline and initiated circulatory support using dopamine infusion. He also required respiratory support by high flow nasal canula due to increased oxygen demand. Markers of poor organ perfusion like oliguria or elevated lactic acid were still within normal limits. An echocardiography before intervention on DOL 2 revealed normal anatomy with dilatation of the right ventricle, mild bowing of the septum to the left and tricuspid regurgitation with a pressure gradient of 33 mmHg indicating elevated pulmonary resistance. In addition, right-to-left shunting over a persistent ductus arteriosus (PDA), left-to-right shunting via a patent foramen ovale (PFO), normal left ventricle function and diastolic backflow in the descending aorta were detected. A head ultrasound confirmed VGAM, measuring 4 x 2 cm with a turbulent flow (50 cm/sec). 3 vascular feeders on the left and 2 on the right with a maximum flow of 105 cm/sec were depicted. Due to high risk of clinical deterioration, we proceeded with EVT under general anesthesia on DOL 2 to reduce effects on cardiac function.
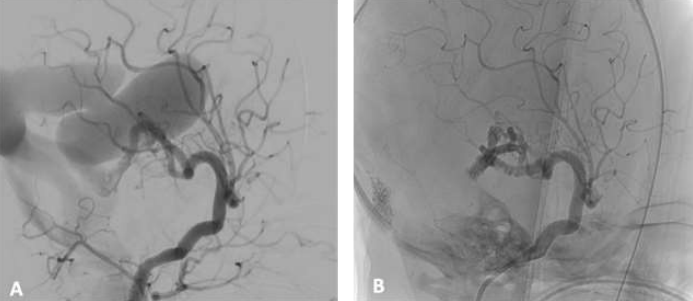
Umbilical artery was chosen for neurointerventional access. Diagnostic digital subtraction angiography identified 4 macroshunts from the right and one from the left PCA. In a first treatment session, strategy was to close several macroshunts with a microcatheter balloon (scepter miniballoon catheter, MicroVention) to achieve reduction of fistula volume and clinical stabilization. EVT should then be continued in 12 months, or earlier in the event of clinical deterioration. Therefore, microcatheter balloon was placed in the largest macroshunt via the right PCA. With an inflated microcatheter balloon, 4 macroshunts were embolized with 1.1 ml PHIL25% (MicroVention), a non-adhesive liquid embolic agent comprised of a biocompatible polymer dissolved in dimethyl sulfoxide covalently bonded to an iodine component to provide radiographic visualization.15 Reduction of flow was successfully accomplished by about 70% (Fig. 1). During embolization, a circumscribed transvenous embolization could be delineated twice. Immediate fluoroscopy of the thorax identified radiopaque embolic agent in the lung and revealed significant bilateral pulmonary arterial embolism. The newborn showed a delayed clinical deterioration with an increase in heart rate and oxygen requirements, decrease in CO2 and hypotension necessitating norepinephrine infusion to support blood pressure. After clinical stabilization with increased FiO2 up to 1.0, the infant was transferred back to the NICU. Chest x-ray after arrival on the NICU confirmed arterial embolism of the embolic agent in both lungs (Fig. 2). Clinically, higher ventilatory pressures were required until DOL 4 along with supplemental oxygen. Noradrenaline as cardiovascular support was necessary for a total of 5 days. Postinterventional echocardiography identified significant dilatation of the right ventricle, severe tricuspid regurgitation (suprasystemic pressure gradient 57mmHg), right-to-left shunting over the PDA and bidirectional shunt over the PFO indicating severe pulmonary hypertension and right heart strain despite significant endovascular reduction of shunting via the VGAM. Therefore, we started a prostaglandin E1 infusion to maintain the PDA serving as a pop-off valve into the systemic circulation decreasing right ventricle afterload and to prevent left ventricular strain and failure. In addition, we nebulized iloprost to reduce vascular pulmonary resistance for 11 consecutives days. Furosemide treatment was introduced due to fluid overload with oliguria and increase in B-type natriuretic peptide (BNP) levels. Due to pulmonary artery embolism and to prevent further thrombi formation or growth, systemic heparinization (400 IU/kg/day) was initiated on day of intervention, reduced to 200 IU/kg/day the following day, and finally switched to low molecular weighted heparin (LMWH) supported by aspirin treatment. With this therapy, we saw a gradual clinical improvement, with reduction in respiratory support and improved oxygenation. Extubation to high flow nasal cannula was successful 5 days after embolization, with supplemental oxygen requirement for 5 additional days. Echocardiographically, a physiological tricuspid insufficiency without pressure gradient with left-to-right shunting over the PDA was achieved by DOL 4 and prostaglandin E1 infusion was discontinued. On DOL 8 PDA was closed, and both ventricles showed a satisfying function with a normal left-sided extraction function (EF, 68%). In a cranial MRI three days after embolization, a regression in the volume of VGAM was observed. Only a microembolic infarct in the right thalamus was visible without any evidence of cerebral hemorrhages. The infant was transferred back closer to the family’s home 17 days after embolization and was finally discharged on aspirin, LMWH and diuretics on DOL 21. At discharge, the newborn presented with mild muscular hypotonia, recurrent opisthotonos, and mildly impaired sucking reflex. 4 months after the first embolization, the second EVT in our hospital was performed due to increase in size of VGAM with accelerated progression in head circumference. This procedure proceeded without complications, resulting in complete closure of the remaining VGAM. Interestingly, the chest x-ray at 4 month of age still showed embolic agent in both pulmonary arteries without clinical and echocardiographic signs for pulmonary hypertension (Fig. 3). The infant's psychomotor development at the age of 4 month is regular, and signs for hydrocephalus were not evident.
Figure 1: Digital subtraction angiography of the right internal carotid artery before and after embolization of feeding arteries for VGAM. Using a scepter miniballoon catheter, 4 shunts feeding the vein of Galen were identified (A). Under fluoroscopic guidance 4 shunts were embolized with PHIL25%. Reduction of flow was successfully accomplished by about 70% (B).
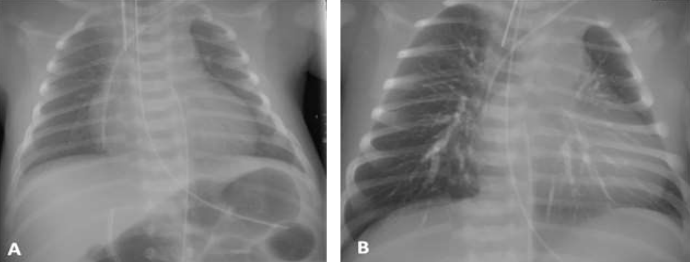
Figure 2: Before/after chest radiograph of patient who underwent embolization for VGAM.
The infant was intubated, received a subclavian venous catheter on the left and arterial umbilical catheter in preparation for embolization (A). During procedure the infant developed lung arterial embolism due to embolic agent (PHIL25%) and chest x-ray displayed radiopaque pulmonary deposition of embolic material in main stem, lobar branches and segmental arteries feeding the dedicated bronchopulmonary segments (B).
Figure 3: Chest radiographs before second endovascular embolization for VGAM at 4 month of age. The infant was intubated and received a subclavian venous catheter on the left. Chest x-ray 4 month after lung arterial embolism still displayed radiopaque pulmonary deposition of embolic material although to a lesser extent.
Discussion and Conclusion
In our case, VGAM was prenatally diagnosed with multiple large feeding vessels and incipient cardiomegaly suggesting a rapid progressive into heart failure after birth.16 Indeed, the infant displayed hemodynamic instability, necessitating the use of catecholamines and respiratory support shortly after birth, an indication for urgent EVT to successfully reverse this condition.17 Echocardiography before EVT identified signs of pulmonary hypertension and reversed flow in the descending aorta, both signs associated with poor prognosis especially if they persist following embolization of cerebral shunts.17 By now EVT is a well recognized therapy for VGAM. Overall periprocedural complications are frequent especially among newborns but in the literature, complication rates mainly focus on neurologic difficulties.16,18 Kjellin et al. explored pulmonary embolization as a complication following EVT of AV malformations in children. In general, pulmonary embolization of embolic material is not uncommon. It is noteworthy that occurrence of clinical symptoms for lung arterial embolism, despite a conspicuous X-ray displaying signs of microemboli, is rare. Eight children out of 34 patients had abnormal chest X-rays with bilateral scattered foci but remained asymptomatic. Only a total of 4% (two patients) of children were symptomatic and one patient developed severe ARDS. This patient stabilized within 7-10 days post-intervention.19 A thorough search of the relevant literature yielded no related article for neonates with respiratory compromise, lining of both main pulmonary arteries and smaller branches following EVT as in our case. After EVT, we used inhaled iloprost, a synthetic prostacyclin analog to support pulmonary vasodilation and improve oxygenation and prostaglandin E1 to maintain ductus arteriosus patency to reduce right ventricle strain and heart failure. Usually, pulmonary vasodilators should be avoided in VGAM especially before EVT, promoting pulmonary overflow with altered gas exchange and compromise of pulmonary vessel maturation. However, in our scenario, clinical decision to promote pulmonary vasodilation was hindered and could finally not be proof but pulmonary hypertension after EVT was most likely related to significant bilateral embolism to pulmonary arteries. Use of prostaglandin E1 led to a reduction in right ventricular afterload supporting left ventricular output and coronary perfusion. This concept is rarely used in VGAM but for other forms of pulmonary hypertension it has been shown to have beneficial effects on ventricular heart function and clinical improvement .21,22 Initially, a main difficulty in this clinical scenario after EVT was to discriminate, whether pulmonary hypertension still originated from VGAM or was caused by lung arterial embolism. The chest x-ray showed opacification in both pulmonary main stem, lobar branches and segmental arteries feeding the dedicated bronchopulmonary segments due to contrast enhanced embolic agent. To further explore the degree of pulmonary embolism, a computed tomography pulmonary angiogram, pulmonary perfusion magnetic resonance imaging (MRI) or cardiac catheterization with angiography of the pulmonary artery would be challenging due to the fact that they are impeded by the embolic contrast agent. A lung perfusion scintigraphy (VQ scan) would have been a possibility but is a tremendous challenge to be realized in a newborn.22 No attempts were made to retrieve lost embolic material. Therefore, we awaited the clinical course and postponed further workup for possible long-term cardiac and lung problems with regular clinical follow-up. Long-term effects of pulmonary deposition of embolic material are not well known. Perivascular fibrosis two month after embolization has been shown in an animal study but timely recanalization of vessels following occlusion with cyanoacrylate agents is reassuring.23 At the age of 4 month, the infant exhibits no obvious pulmonary problems and a normal cardiac function. In addition, physiological high pulmonary pressure on DOL 2 may have protected him from more severe embolism and chronic pulmonary vascular hypertensive disease with detrimental consequences for future life.24 Nevertheless, EVT for VGAM was a life-saving procedure in our patient and it outweighs the risk of pulmonary embolism.
Ethics approval and consent to participate: Not applicable
Consent for publication: Consent for publication was obtained from both parents.
Availability of data and materials: The datasets used and analysed for the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests
Funding: Not applicable
Acknowledgements: None
References
1. Gillet de Thorey A, Ozanne A, Melki J, Dumery G, Benachi A, Vivanti AJ. State of the art of antenatal diagnosis and management of vein of Galen aneurysmal malformations. Prenat Diagn. 2022;42(9):1073-1080.
2. Yan J, Wen J, Gopaul R, Zhang CY, Xiao SW. Outcome and complications of endovascular embolization for vein of Galen malformations: a systematic review and meta-analysis. J Neurosurg. 2015;123(4):872-90.
3. Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology. 1989;31(2):109-28.
4. Bhattacharya JJ, Thammaroj J. Vein of galen malformations. J Neurol Neurosurg Psychiatry. 2003;74 Suppl 1:i42-4.
5. Tas B, Starnoni D, Smajda S et al.: Arteriovenous Cerebral High Flow Shunts in Children: From Genotype to Phenotype. Front Pediatr. 2022;10:871565.
6. Duran D, Karschnia P, Gaillard JR et al.: Human genetics and molecular mechanisms of vein of Galen malformation. J Neurosurg Pediatr. 2018;21(4):367-374.
7. Paladini D, Deloison B, Rossi A et al.: Vein of Galen aneurysmal malformation (VGAM) in the fetus: retrospective analysis of perinatal prognostic indicators in a two-center series of 49 cases. Ultrasound Obstet Gynecol. 2017;50(2):192-199.
8. Taffin H, Maurey H, Ozanne A et al.: Long-term outcome of vein of Galen malformation. Dev Med Child Neurol. 2020;62(6):729-734.
9. Cory MJ, Durand P, Sillero R et al.: Vein of Galen aneurysmal malformation: rationalizing medical management of neonatal heart failure. Pediatr Res. 2023 Jan;93(1):39-48.
10. Heuer GG, Gabel B, Beslow LA et al.: Diagnosis and treatment of vein of Galen aneurysmal malformations. Childs Nerv Syst. 2010;26(7):879-87.
11. Jones BV, Ball WS, Tomsick TA, Millard J, Crone KR. Vein of Galen aneurysmal malformation: diagnosis and treatment of 13 children with extended clinical follow-up. AJNR Am J Neuroradiol. 2002;23(10):1717-24.
12. Berenstein A, Fifi JT, Niimi Y et al.: Vein of Galen malformations in neonates: new management paradigms for improving outcomes. Neurosurgery. 2012;70(5):1207-13
13. Mortazavi MM, Griessenauer CJ, Foreman P et al.: Vein of Galen aneurysmal malformations: critical analysis of the literature with proposal of a new classification system. J Neurosurg Pediatr. 2013;12(3):293-306.
14. Lasjaunias PL, Chng SM, Sachet M, Alvarez H, Rodesch G, Garcia-Monaco R. The management of vein of Galen aneurysmal malformations. Neurosurgery. 2006;59(5Suppl3):S184-94;
15. Vollherbst DF, Chapot R, Bendszus M, Möhlenbruch MA. Glue, Onyx, Squid or PHIL? Liquid Embolic Agents for the Embolization of Cerebral Arteriovenous Malformations and Dural Arteriovenous Fistulas. Clin Neuroradiol. 2022;32(1):25-38.
16. Brinjikji W, Krings T, Murad MH, Rouchaud A, Meila D. Endovascular Treatment of Vein of Galen Malformations: A Systematic Review and Meta-Analysis. AJNR Am J Neuroradiol. 2017;38(12):2308-2314.
17. Geibprasert S, Krings T, Armstrong D, Terbrugge KG, Raybaud CA. Predicting factors for the follow-up outcome and management decisions in vein of Galen aneurysmal malformations. Childs Nerv Syst. 2010;26(1):35-46.
18. Buratti S, Mallamaci M, Tuo G et al.: Vein of Galen aneurysmal malformation in newborns: a retrospective study to describe a paradigm of treatment and identify risk factors of adverse outcome in a referral center. Front Pediatr. 2023;11:1193738.
19. Kjellin IB, Boechat MI, Vinuela F, Westra SJ, Duckwiler GR. Pulmonary emboli following therapeutic embolization of cerebral arteriovenous malformations in children. Pediatr Radiol. 2000;30(4):279-83.
20. Singh Y, Lakshminrusimha S. Pathophysiology and Management of Persistent Pulmonary Hypertension of the Newborn. Clin Perinatol. 2021;48(3):595-618.
21. Karam O, da Cruz E, Rimensberger PC. VGAM induced high-flow congestive heart failure responsive to PGE1 infusion. Int J Cardiol. 2009;132(2):e60-2.
22. Takahashi K, Kuwahara T, Nagatsu M. Changes in 99mTechnegas ventilation lung scan in a newborn with absent pulmonary valve syndrome. Cardiol Young. 2001;11(6):673-5.
23. Brothers MF, Kaufmann JC, Fox AJ, Deveikis JP. n-Butyl 2-cyanoacrylate--substitute for IBCA in interventional neuroradiology: histopathologic and polymerization time studies. AJNR Am J Neuroradiol. 1989;10(4):777-86.
24. Khurana J, Orbach DB, Gauvreau K et al.: Pulmonary Hypertension in Infants and Children with Vein of Galen Malformation and Association with Clinical Outcomes. J Pediatr. 2023;258:113404.