ECMO as a Novel Life Support in the Management of Diffuse Alveolar Haemorrhage.
ECMO as a Novel Life Support in the Management of Diffuse Alveolar Haemorrhage.
Dr Nirmala*, Dr Pavan Yadav1
1. Dr Pavan Yadav M.D Respiratory Medicine, FCCP, Lead consultant ,Interventional pulmonology and Lung transplant team , Aster RV hospital , Bangalore.
Correspondence to: Dr Nirmala. M.A, M.D, DNB Respiratory Medicine, Consultant, Interventional pulmonology and Lung transplant team, Aster RV hospital, Bangalore.
Copyright.
© 2024 Dr. Nirmala. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 March 2024
Published: 03 June 2024
Abstract
Diffuse alveolar haemorrhage(DAH) secondary to vasculitis usually presents with severe respiratory failure and persistent hypoxia, which is acute in presentation and requires immediate ventilator management . Some of these patients have persistent hypoxia despite conventional mechanical ventilation like lung protective ventilation strategies, recruitment maneuvers, vasodilators, proning protocols. In these patients ECMO can be initiated , because early initiation of ECMO helps in the early phase of the disease helps in adequate gas exchange , hence providing time for the immunosuppressive therapies to act. We hereby present to you a case report of a young female who presented Acute Respiratory Distress Syndrome (ARDS) who was evaluated and diagnosed as DAH secondary to ANCA associated vasculitis , successfully managed with ventilation and early initiation of ECMO. ECMO is not being widely used in DAH given the complications of bleeding. However we managed a strict ACT and APTT during the inititiation and the complete duration of ECMO . We were able to wean the patient of ECMO by Day 5 of initiation without any complications. There are multiple case reports and series recommending the use of ECMO in persistent hypoxia associated with DAH. However before initiating ECMO , complications of bleeding should always be considered and anticoagulants have to be used wisely. We have also reviewed the literature of few case reports and case series and compared the demographic data , complications and outcomes in all these patients initiated on ECMO.
ECMO as a Novel Life Support in the Management of Diffuse Alveolar Haemorrhage.
Introduction
Vasculitis are a group of disorders caused by the inflammation of the blood vessels. Anti Neutrophil Cytoplasmic Antibodies are autoantibodies produced against the antigens present in the cytoplasmic granules of the neutrophils and lysosomes of the monocytes(1,2).Major causes of vasculitis affecting the small and medium vessels of the lungs can be divided into Microscopic polyangitis(MPA), Granulomatosis with Polyangitis (GPA) and Easinophilic Granulomatosis with Polyangitis (EGPA).
Vasculitis causes damage to the endothelium thereby disruting the alveolar capillary basement membrane casusing extravasation of the red blood cells to the alveolar spaces .(3)This results in Diffuse Alveolar Haemorrhage(DAH) and sudden respiratory failure requiring the need for urgent mechanical ventilation . Some of these patients continue to be hypoxic even after ventilation , such patients can be initiated on ECMO as early as possible. We hereby present a case of a 27 year old female presented with DAH who was successfully managed with ECMO in Aster RV hospital, Bangalore.
Case History
27 year old female came with complaints of breathlessness and dry cough increased since 3 to 4 days. She also had history of ankle joint pain and asymmetrical swelling. She was recently admitted with membranous tonsillitis in an outside hospital and was treated with iv antibiotics. She also had a history of chronic iron deficiency which was evaluated with colonoscopy which showed terminal ileal ulcers. She was admitted in Aster RV hospital with the above mentioned complaints, she was not hypoxic at the time of admission and her vitals were stable. CT chest was done which showed diffuse patchy ground glassing in bilateral lung fields with relative sparing of the sub pleural zones predominantly involving lower lobes. Few nodular infiltrates and fibrotic foci in the left upper lobe also seen. Differentials included atypical viral pneumonia and rheumatoid lung. She was started on IV empirical antibiotics, antivirals and other supportive measures. The next day she became hypoxic with spo2 dropped to 89% on room air and she was started on supplemental oxygen. Hence fibreoptic bronchoscopy was done and lavage taken from both the lower lobes. Bronchoscopy showed haemorrhage in the tracheobronchial tree as shown in figure 1A. Indicative of DAH. Sequential BAL collected also indicated DAH. BAL samples were negative for Gene Xpert MTB/RIF, AFB smear , KOH mount and aerobic culture showed no growth . Since bronchoscopy showed a picture of intra alveolar haemorrhage , her connective tissue work up was done which showed PM scl 75, ANCA PR3 ( C ANCA ) were positive. Her Blood and urine cultures showed no growth. She dramatically worsened in a day and was intubated and started on mechanical ventilation in view of persistent hypoxia and low PaO2/FiO2 . She was put on volume controlled ventilation , Tidal volume 400 ml , PEEP- 6 cmH2o, Respiratory rate of 18 breaths / min were applied. Despite the continuous mechanical ventilation with a fio2 of 100 % , hypoxemia failed to improve and Pao2/ Fio2 continued to deteriorate. However she didn’t improve and had persistent hypoxia with hypercarbia despite maximum ventilator support. After detailed discussion she was initiated on Extra corporeal membrane oxygenation (ECMO) on Day 4 of hospitalisation after getting informed consent and explaining the risks and complications of the procedure. A 22 Fr cannula was inserted into the patients right femoral vein and 16 Fr cannula was inserted into the patient’s right jugular vein . The location of the cannulas were confirmed by the Trans Oeosophageal Echo (TEE) . The blood was then circulated from the femoral vein to the oxygenator and then to the internal jugular vein . The blood flow rate was started at 3.5 litres / min and sweep gas flow was set at 7 litres / min . She was given bolus of 5000 IU of heparin during ECMO initiation and then started maintainance dose of 1000 units per hour after 2 hours . Her ACT was checked every 6 hours and maintained around 180 and APTT was maintained around 60 seconds . Since BAL samples were negative for any infective foci , diagnosis of DAH was considered and she was given 3 doses pulse methylprednisolone 1gm/day .
She was started on intravenous cyclophosphamide. However since there was not much improvement in oxygenation and persistent lung infiltrates, after multidisciplinary discussion she was given 7 cycles of plasmapheresis and IV Rituximab. She gradually improved clinically , her serial chest x rays showed improvement , oxygenation improved and was eventually decannulated from ECMO on day 7.Sedation was slowly withdrawn , her GCS improved and she was gradually weaned off from ventilator support over next 5 days. She was mobilised, was given adequate chest and limb physiotherapy and was shifted to ward on minimal oxygen support over next 5 days. Eventually her oxygenation improved and she was discharged without oxygen support with tapering steroids and PCP prophylaxis. She had followed up at OPD and was free of symptoms, chest x ray showed significant improvement with complete clearing up of parenchymal infiltrates. Below are the serial Chest X rays taken during the course of hospital admission and follow up.
Figure 2: Fibreoptic Bronchoscopy image of DAH
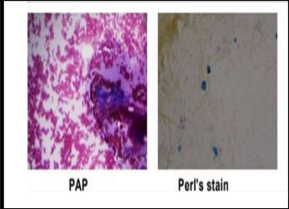
Figure 3: BAL for cytology in DAH
Discussion
Diffuse Alveolar Haemorrhage (DAH) is a syndrome characterised by bleeding into the alveolar spaces . It is caused by the disruption of the alveolar capillary basement membrane. Clinical presentation includes sudden onset of breathlessness , haemoptysis , hypoxia , sudden drop in haemoglobin and appearance of new bilateral pulmonary infiltrates on chest X ray. There are a variety of conditions causing DAH. However it is usually classified based on the histologic appearance as described below in Table 1(4,5,6).
Table 1
Pulmonary capillaritis- Neutrophilic infiltration of the lung interstitium leading to necrosis of the capillary endothelium and spillage of the red blood cells into the alveoli
Bland Pulmonary haemorrhage – Haemorrhage into the alveolar spaces without inflammation or destruction of the alveolar structure
Diffuse alveolar damage - DAD can cause damage to the alveolar interstitium and formation of hyaline membrane that lines the alveolar space.
Clinical presentation and evaluation of DAH
DAH usually presents with fever, haemoptysis, hypoxia, drop in haemoglobin although haemoptysis is present only in one third of the patients. Some patients present with acute onset breathlessness and requiring mechanical ventilation as described in the above case. CT picture shows bilateral ground glassing / consolidation which is diffuse. Recurrent DAH occurs in Idiopathic Pulmonary Hemosiderosis (IPH) resulting in pulmonary fibrosis later. DAH is usually associated with drop in haemoglobin, also since certain conditions are associated with renal damage like glomerulosclerosis, crescentic glomerulonephritis etc, hence associated with the elevation of serum creatinine. The characteristic bronchoscopy picture shows intra bronchial bleeding and sequential progressive haemorrhagic BAL sample. The definitive diagnosis is done by cytology which shows hemosiderin laden macrophages on Prussian blue stain . DLCO will be increased in DAH in stable patients if it can be performed.
Presentation in specific etiologies
Any drugs causing DAH should be immediately stopped to prevent respiratory failure . The drugs which can cause the illness are listed in the above table.
* Covid 19 is associated with DAH. A study conducted in Switzerland (7), which investigated post mortem lung findings in 20 patients who died of Covid 19 . In this study 3 patients had DAH , and one had changes of vasculitis in the post mortem histopathological examination of the biopsy specimen.
* Vaping is associated with DAH. Even though vaping has been associated with eosinophilic pneumonia, lipoid pneumonia, organising pneumonia , DAD , ARDS , giant cell interstitial pneumonitis , a case report of vaping associated with DAH was also published (8)
* Systemic vasculitis like SLE or APLA should be treated adequately with immunosuppression r plasmapheresis depending on the severity . In patients with nasal or oral ulcers, uveitis, foot drop , malar rash an underlying vasculitis to be suspected .
* Leptospirosis can present as a serious complication called weils disease (fever, jaundice, renal
failure) , in which less than 5 percent of the individuals develop DAH amongst which 50 to 70% may result in fatal disease especially in areas with high endemicity (9,10).
Specific Lab abnormalities
* Specific microbiological and lab investigations to be done to identify the specific etiology in case of DAH. Blood urea nitrogen to be obtained in patients suspected with pulmonary renal syndrome. An elevated plasma creatinine concentration , abnormal urine analysis like RBC, red cell and white cell casts are present in such cases .
* A positive C ANCA ( antiproteinase 3 ) antibodies is most consistent with GPA , while P ANCA ( anti MPO antibodies ) are more consistent with MPA or eosinophilic GPA . Anti GBM antibodies are seen in goodpasteurs disease and a renal biopsy is also required unless contraindicated.
* SLE usually presents with anti ds DNA antibodies, however drug induced lupus presents with anti histone antibodies.
* Anti- transglutaminase or anti-endomysial ( Ig A) antibodies in a patient with DAH may represent a combination of celiac disease and pulmonary haemosiderosis collectively known as Lane Hamilton syndrome.
* Also covid 19 to be ruled out in any patients with Diffuse Alveolar haemorrhage .
BAL is an important diagnostic tool for DAH. Bronchoscopy usually reveals progressive haemorrhagic BAL. BAL cytology may sometime reveal hemoisiderin laden macrophages. BAL is also important in severe ARDS since it helps in diagnosing any associated viral, parasitic or bacterial illness.
In case of any vasculitis, lung biopsy is more specific than kidney and skin biopsy in the diagnosis.
Histopathology of he specific biopsy findings are described as below:
1. Linear Ig G deposition in the alveolar capillary basement membrane – Good pasteurs syndrome.
2. Granular immune complex deposition in the alveolar capillary basement membrane- SLE, RA and if these immune deposits are Ig E- Henoch Schonlein Purpura
3. Isolated pulmonary capillaritis- GPA, MPA
Respiratory system involvement in systemic vasculitis:
* Among patients with GPA , 90 percent have nasal , sinus or ear involvement, compared to 35 percent of the patients with MPA , usually presented with hearing loss (11). Respiratory symptoms in MPA and GPA are usually cough, haemoptysis , dyspnoea and pleuritic chest pain . The severity of all these symptoms may vary from a mild illness to a severe fulminant alveolar haemorrhage . However , in GPA it is unusual for the patient to present with
respiratory symptoms without upper respiratory tract involvement. Keeping in consideration all the above facts , the diagnosis of MPA was made in our patient as she presented with fulminant alveolar haemorrhage , no upper respiratory tract involvement and C ANCA positive.
* Airway complications like subglottic stenosis is very common in GPA sometimes severe enough to necessitate tracheostomy (12), however this is usually not seen in MPA .
* Lung parenchymal nodule may be identified as an incidental finding in both GPA and MPA.
* Interstitial lung disease is also more in MPA than GPA. In MPA , ILD can suggest a disease onset and may present as an initial finding before any other organ involvement. Prevalance of ILD is more common in MPA than GPA.(13)
* DAH is the presenting symptom in 5 to 45 percent of patients with ANCA associated vasculitis (13.14).These patients usually present with hemoptysis , hypoxia, dyspnoea, drop in haemoglobin ,respiratory failure.
* Pulmonary artery stenosis is also seen in few cases with GPA or MPA. These patients might have a normal pulmonary artery pressure and diagnosis is made only with CT pulmonary angiogram .
Treatment of DAH
Treatment of DAH involves 3 important measures :(15)
1. Supportive care , haemodynamic stability, vetilatory management with high PEEP , which produces a tamponade effect to reduce the bleeding into the alveoli.
2. Treat the underlying cause with immunosuprresives , plasmapheresis , antibiotics or antivirals in case of any secondary infections
3. Rapid and effective local hemostasis .
* AH in a vasculitis is usually treated with glucocorticoids , pulse iv dose methyl prednisolone (500 to 1000 mg ) for 1-3 days (15) followed by transition to oral tapering doses cam be done. A study was performed comparing the dose effect of corticosteroids for DAH. This study concluded that patients treated with low dose (<250 mg/ day ) corticosteroids had significantly lower ICU mortality rate compared to those treated with medium dose
(250-1000 mg/ day ) or high dose (> 1000 mg/ day ), however the overall mortality did not differ(16).We had given similar pulse doses of methylprednisolone. Despite this, patient’s Pao2/ Fio2 was still low and hence was started on cyclophosphamide
* Other treatment options include rituximab, a chimeric monoclonal antibody targeting CD20 has been used. It causes antibody mediated depletion of the CD20 positive plasma cells thereby decreasing the autoantibody production and controlling the disease activity (17,18) .
* Rituximab is given at a dose of 375 mg/m2 per week for 4 weeks as used in the RAVE trial .A study was conducted regarding efficacy and complications of administering rituximab as an induction and /or maintainance therapy in GPA / MPA showed that there is better reversal of the acute illness, however long term therapy resulted in higher rates of infection(19).
* A randomised control trial was conducted comparing the efficacy of combination therapies of glucocorticoids plus rituximab (375 mg/m2once weekly for 4 weeks ) and glucocorticoids plus cyclophosphamide (2 mg/kg/day) showed comparable efficacy of rituximab in remission induction in severe ANCA associated vasculitis , also rituximab showed better efficacy in preventing recurrent renal disease , alveolar haemorrhages(20).
* For achieving hemostasis, Thromboxane A2 can be used intravenous or inhalation form in case of DAH which helps to stabilize the clot inhibiting the conversion of plasminogen to plasmin inhibiting fibrinolysis (21,22,23).
* Cartin Ceba et al (19) conducted a study to evaluate the efficacy of plasma exchange and of rituximab versus cyclophosphamide in patients with DAH secondary to ANCA associated vasculitis with or without respiratory failure. This study was conducted in an institution , where among 73 patients with DAH , 34 of them experienced respiratory failure. This study concluded that no clear benefit in addition of plasma exchange to standard remission induction therapy was seen , however patients receiving rituximab had a higher rate of complete remission by 6 months compared to cyclophosphamide
ECMO in the management of DAH
- We have reviewed case reports and series of 15 patients in the past years where ECMO was used as a tool in the management of DAH(Table 2) , In all these patients it was observed that application of ECMO provides valuable time for the management of the underlying disease with immunosuppression , plasmapheresis or renal replacement therapy. It was also observed that only a few case series were reported with increased risk of bleeding on initiating ECMO, however most of the reports had a better patient outcome. Evaluation in a patient presenting as ARDS.
- It was also observed that early initiation of ECMO resulted in a better patient outcome . Despite the advantages ECMO has its own complications like bleeding due to continuous anticoagulation and consumption coagulopathy .Review of literature had shown development of hemothorax at the ICD site which was inserted for pneumothorax in one patient and development of asymptomatic thrombocytopenia in the other treated with ECMO(35,36). However the overall bleeding risk is similar to other patients on ECMO but this needs more research. Moreover ECMO has its balancing harms and benefits in managing DAH , it can exacerbate the underlying DAH and can also provide time for the application of immunosuppressive therapy.
Table 2
DAH- Diffuse Alveolar Haemorrhage , RF- Respiratory failure , ARF- Acute Renal failure , MPO - Myeloperoxidase , PR3- Proteinase 3 , NM- Not mentioned , CYC- Cyclophosphamide, GC- Glucocorticoids , PLEX - Plasmapheresis , RRT- Renal replacement Therapy , IVIG- Intravenous immunoglobulins ,GGO- Ground glass opacities, NM- Not mentioned
Please Click here to view tables
Conclusion
DAH is an acute life threatening condition which requires timely diagnosis and early initiation of treatment. The case described above was a diagnostic challenge for any pulmonologists given the fulminant course of illness and progressive respiratory failure. This case is a diagnostic challenge for us since the patient was not a previously diagnosed case of vasculitis and this was her first time admission.However timely bronchoscopy, and diagnosis helped us in early diagnosis and ruling out any other associated infections. Also early initiation of ECMO in this patient provided adequate time for immunosuppression induction thereby treating the underlying condition. Hence vigilant work up has to be done in any patient coming with ARDS, keeping in mind rare causes like DAH, because this condition is reversible if diagnosed and treated during the earlier stages of presentation. Also even though ECMO is a highly invasive procedure with increased bleeding risk, it should always be considered in patients with vasculitis associated DAH who has persistent hypoxia post conventional mechanical ventilation. The bleeding risk in ECMO due to administration of anticoagulants and consumption coagulopathy can be managed with vigilant monitoring of ACT/ aPTT.
References
1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1-11.
2. Alba MA, Jennette JC, Falk RJ. Pathogenesis of ANCAAssociated Pulmonary Vasculitis. Semin Respir Crit Care Med 2018;39:413-24.
3. . Delvino P, Monti S, Balduzzi S, et al. The role of extracorporeal membrane oxygenation (ECMO) in the treatment of diffuse alveolar haemorrhage secondary to ANCA-associated vasculitis: report of two cases and review of the literature. Rheumatol Int 2019;39:367-75.
4. Franks TJ, Koss MN. Pulmonary capillaritis. Curr Opin Pulm Med. 2000 Sep;6(5):430-5. doi: 10.1097/00063198-200009000-00008. PMID: 10958235.
5. Mark EJ, Ramirez JF. Pulmonary capillaritis and hemorrhage in patients with systemic vasculitis. Arch Pathol Lab Med. 1985 May;109(5):413-8. PMID: 3838654.
6. Mark EJ, Ramirez JF. Pulmonary capillaritis and hemorrhage in patients with systemic vasculitis. Arch Pathol Lab Med. 1985 May;109(5):413-8. PMID: 3838654.
7. Menter T, Haslbauer JD, Nienhold R, Savic S, Hopfer H, Deigendesch N, Frank S, Turek D, Willi N, Pargger H, Bassetti S, Leuppi JD, Cathomas G, Tolnay M, Mertz KD, Tzankov A. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology. 2020 Aug;77(2):198-209. doi: 10.1111/his.14134. Epub 2020 Jul 5. PMID: 32364264; PMCID: PMC7496150.
8. Edmonds PJ, Copeland C, Conger A, Richmond BW. Vaping-induced diffuse alveolar hemorrhage. Respir Med Case Rep. 2020 Jan 7;29:100996. doi: 10.1016/j.rmcr.2020.100996. PMID: 31956478; PMCID: PMC6957782.
9. Segura ER, Ganoza CA, Campos K, Ricaldi JN, Torres S, Silva H, Céspedes MJ, Matthias MA, Swancutt MA, López Liñán R, Gotuzzo E, Guerra H, Gilman RH, Vinetz JM; Peru-United States Leptospirosis Consortium. Clinical spectrum of pulmonary involvement in leptospirosis in a region of endemicity, with quantification of leptospiral burden. Clin Infect Dis. 2005 Feb 1;40(3):343-51. doi: 10.1086/427110. Epub 2005 Jan 10. PMID: 15668855; PMCID: PMC2366057.
10. Carvalho CR, Bethlem EP. Pulmonary complications of leptospirosis. Clin Chest Med. 2002 Jun;23(2):469-78. doi: 10.1016/s0272-5231(01)00010-7. PMID: 12092040.
11. Sugimoto T, Sakaguchi M, Deji N, Uzu T, Nishio Y, Kashiwagi A. The occurrence of sensorineural hearing loss in a patient with myeloperoxidase-anti-neutrophil cytoplasmic antibody-related microscopic polyangiitis. Rheumatol Int. 2007 Mar;27(5):503-5. doi: 10.1007/s00296-006-0213-5. PMID: 16969635.
12. Polychronopoulos VS, Prakash UB, Golbin JM, Edell ES, Specks U. Airway involvement in Wegener's granulomatosis. Rheum Dis Clin North Am. 2007 Nov;33(4):755-75, vi. doi: 10.1016/j.rdc.2007.09.004. PMID: 18037115.
13. Arulkumaran N, Periselneris N, Gaskin G, Strickland N, Ind PW, Pusey CD, et al. Interstitial lung disease and ANCA-associated vasculitis: a retrospective observational cohort study.Rheumatology (Oxford) 2011;50:2035–43. [PubMed: 21873269]
13. Pesci A, Pavone L, Buzio C, Manganelli P. Respiratory system involvement in ANCA-associated systemic vasculitides. Sarcoidosis Vasc Diffuse Lung Dis. 2005 Dec;22 Suppl 1:S40-8. PMID: 16457016.
14. Schwarz MI, Brown KK. Small vessel vasculitis of the lung. Thorax. 2000 Jun;55(6):502-10. doi: 10.1136/thorax.55.6.502. PMID: 10817800; PMCID: PMC1745770.
15. Heslet, L.; Nielsen, J.D.; Nepper-Christensen, S. Local pulmonary administration of factor VIIa (rFVIIa) in diffuse alveolar hemorrhage (DAH)—A review of a new treatment paradigm. Biologics 2012, 6, 37–46
16. Rathi, N.K.; Tanner, A.R.; Dinh, A.; Dong, W.; Feng, L.; Ensor, J.; Wallace, S.K.; Haque, S.A.; Rondon, G.; Price, K.J.; et al. Low-, medium- and high-dose steroids with or without aminocaproic acid in adult hematopoietic SCT patients with diffuse alveolar hemorrhage. Bone Marrow Transplant. 2015, 50, 420–426
17. Walsh, M.; Jayne, D. Rituximab in the treatment of anti-neutrophil cytoplasm antibody associated vasculitis and systemic lupus erythematosus: Past, present and future. Kidney Int. 2007, 72, 676–682.
18 . Jones, R.B.; Ferraro, A.J.; Chaudhry, A.N.; Brogan, P.; Salama, A.D.; Smith, K.G.; Savage, C.O.; Jayne, D.R. A multicenter survey of rituximab therapy for refractory antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum. 2009, 60, 2156–2168
19. Cartin-Ceba R, Fervenza F, Ytterberg SR, Specks U. Diffuse Alveolar Hemorrhage Secondary to ANCA-Associated Vasculitis: Predictors of Respiratory Failure and Clinical Outcomes
[abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10).
https://acrabstracts.org/abstract/diffuse-alveolar-hemorrhage-secondary-to-anca-associated-vasculit is-predictors-of-respiratory-failure-and-clinical-outcomes/. Accessed November 29, 2022.
20. Stone, J.H.; Merkel, P.A.; Spiera, R.; Seo, P.; Langford, C.A.; Hoffman, G.S.; Kallenberg, C.G.; St Clair, E.W.; Turkiewicz, A.; Tchao, N.K.; et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N. Engl. J. Med. 2010, 363, 221–232.
21. Solomonov, A.; Fruchter, O.; Zuckerman, T.; Brenner, B.; Yigla, M. Pulmonary hemorrhage: A novel mode of therapy. Respir. Med. 2009, 103, 1196–1200.
22. O’Neil, E.R.; Schmees, L.R.; Resendiz, K.; Justino, H.; Anders, M.M. Inhaled Tranexamic Acid as a Novel Treatment for Pulmonary Hemorrhage in Critically Ill Pediatric Patients: An Observational Study. Crit. Care Explor. 2020, 2, e0075.
23. Bafaqih, H.; Chehab, M.; Almohaimeed, S.; Thabet, F.; Alhejaily, A.; AlShahrani, M.; Zolaly, M.A.; Abdelmoneim, A.A.; Abd, E.S. Pilot trial of a novel two-step therapy protocol using nebulized tranexamic acid and recombinant factor VIIa in children with intractable diffuse alveolar hemorrhage. Ann. Saudi Med. 2015, 35, 231–233
24 Khattar ramini et al, AUTOIMMUNE DIFFUSE ALVEOLAR HEMORRHAGE TREATED WITH CYCLOPHOSPHAMIDE WHILE ON EXTRACORPOREAL MEMBRANE OXYGENATION,CHEST , Oct 18-21,
2020, https://doi.org/10.1016/j.chest.2020.08.692.
25 https://rdcu.be/c6FTV
26 Hartmann A, Nordal KP, Svennevig J, Noddeland H, Pedersen T, Skarbøvik AJ, Fauchald P. Successful use of artificial lung (ECMO) and kidney in the treatment of a 20-year-old female with Wegener's syndrome. Nephrol Dial Transplant. 1994;9(3):316-9. PMID: 8052441.
27 Rawal G, Kumar R, Yadav S. ECMO Rescue Therapy in Diffuse Alveolar Haemorrhage: A Case Report with Review of Literature. J Clin Diagn Res. 2016 Jun;10(6):OD10-1. doi: 10.7860/JCDR/2016/20649.7969. Epub 2016 Jun 1. PMID: 27504336; PMCID: PMC4963696.
28 Wang L, Wang J, Xu Y, Jiao J, Xie L, Mo G. A novel therapeutic strategy using extracorporeal membrane oxygenation in patients with anti-neutrophil cytoplasmic antibodies-associated vasculitis: a case report and literature review. Ann Transl Med. 2021 Aug;9(15):1267. doi:
10.21037/atm-21-3133. PMID: 34532404; PMCID: PMC8421983.
29 Yin K, March RJ, Hoopes CW, Balk RA, Raman J, Lateef OB, Tiwari A, Bak E, Karlson KJ, Edwards NM, Dobrilovic N. Extracorporeal membrane oxygenation in the management of granulomatosis with polyangiitis. J Card Surg. 2021 Feb;36(2):743-747. doi: 10.1111/jocs.15252. Epub 2020 Dec 22. PMID: 33350513.
30 Hohenforst-Schmidt W, Petermann A, Visouli A, Zarogoulidis P, Darwiche K, Kougioumtzi I, Tsakiridis K, Machairiotis N, Ketteler M, Zarogoulidis K, Brachmann J. Successful application of extracorporeal membrane oxygenation due to pulmonary hemorrhage secondary to granulomatosis with polyangiitis. Drug Des Devel Ther. 2013 Jul 24;7:627-33. doi: 10.2147/DDDT.S47156. PMID: 23926421; PMCID: PMC3728271.
31 Kelly D, Makkuni D, Ail D. Rare cause of respiratory failure in a young woman: isolated diffuse alveolar haemorrhage requiring extracorporeal membrane oxygenation. BMJ Case Rep. 2017 Aug 3;2017:bcr2017219235. doi: 10.1136/bcr-2017-219235. PMID: 28775083; PMCID: PMC5612507
32 Arnold S, Deja M, Nitschke M, Bohnet S, Wallis S, Humrich JY, Riemekasten G, Steinhoff J, Lamprecht P. Extracorporeal membrane oxygenation in ANCA-associated vasculitis. Autoimmun Rev. 2021 Jan;20(1):102702. doi: 10.1016/j.autrev.2020.102702. Epub 2020 Nov 11. PMID: 33188916.
33 Lee CF, Huang CT, Ruan SY. Endotracheal tube clamping and extracorporeal membrane oxygenation to resuscitate massive pulmonary haemorrhage. Respirol Case Rep 2018;6:e00321.
34 Kundu S, Sharma S, Minhas R, et al. Acute Respiratory Distress Syndrome Requiring Extracorporeal Membrane Oxygenation as the Initial Presentation of Anti-neutrophillic Cytoplasmic Auto-antibody Positive Vasculitis. Cureus 2019;11:e6135.
35. Ahmed SH, Aziz T, Cochran J, Highland K (2004) Use of extracorporeal membrane oxygenation in a patient with diffuse alveolar hemorrhage. Chest 126(1):305–309
36. Balasubramanian SK, Tiruvoipati R, Chatterjee S, Sosnowski A, Firmin RK (2005) Extracorporeal membrane oxygenation with lepirudin anticoagulation for Wegener’s granulomatosis with heparin-induced thrombocytopenia. ASAIO J 51(4):477–479.