Synchronous Endometrial and Ovarian Carcinoma-A Case Report
Synchronous Endometrial and Ovarian Carcinoma-A Case Report
Dr Poojashree K S *
*Correspondence to: Dr Poojashree K S, DMRT DNB Radiation Oncology, Cytecare Hospitals, Bengaluru.
Copyright.
© 2024 Dr Poojashree K S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2024
Published: 01 July 2024
Abstract
Synchronous Endometrial and Ovarian cancer (SEOC) is defined as the simultaneous presence of these two cancers at the time of diagnosis as opposed to metachronous cancer where these two cancers are diagnosed at different chronologic time points. Synchronous malignancies in the female genital tract are very rare entities (0.5-1.7%). Among them, synchronous endometrial and ovarian tumors are the most common types of malignancy, with a frequency of 5% among endometrial and 10% among ovarian primary tumors. A 27 years old female unmarried and nulliparous, presented to our hospital with mass per abdomen since 2 months. History of occasional dull aching pain and occasional low back ache since 2-3 months. Evaluated for the above complaints, diagnosed to have Synchronous Endometrial and Ovarian Carcinoma. All the biochemical parameters are within acceptable limits. Underwent Fertility sparing surgery, followed by adjuvant chemotheray and radiotherapy given.
Key Words: Synchronous endometrial and ovarian cancer, Radiotherapy, brachytherapy.
Synchronous Endometrial and Ovarian Carcinoma-A Case Report
Introduction
Synchronous endometrial and ovarian cancer (SEOC) is defined as the simultaneous presence of these two cancers at the time of diagnosis as opposed to metachronous cancer where these two cancers are diagnosed at different chronologic time points.1 Synchronous malignancies in the female genital tract are very rare entities (0.5-1.7%). Among them, synchronous endometrial and ovarian tumors are the most common types of malignancy, with a frequency of 5% among endometrial and 10% among ovarian primary tumors.2
Synchronous endometrial and ovarian tumors are rare variants of gynecological cancers, and they must be differentiated from either primary endometrium or ovarian tumors with metastasis. The landmark criteria have been laid down by Ulbright and Roth, and later refined substantially by Scully et al.3
Obesity has resulted in changing trends of endometrial disease, resulting in a gradual increase in the incidence of the disease in the past few decades. Menopausal hormonal therapy as well as the use of oral contraceptives have caused a steady fall in the incidence of ovarian cancer. Many theories have been proposed about these relative proportions of synchronous tumors, which include changing demographic trends and the introduction of diagnostic criteria in 1980, which was adopted by many centers in later years.4
Factors such as obesity, nulliparity, and comparatively younger age may attribute a “hormonal field effect” to the development of synchronous endometrioid cancers. The morphological unit consisting of the uterus, fallopian tubes, and ovary as part of the Mullerian system may explain the synchronous appearance of these malignancies. Niskakoski et al have suggested a shared origin of synchronous endometrial and ovarian carcinoma in Lynch syndrome (LS), indicating converging pathways of tumorigenesis. L1 cell adhesion molecule (L1CAM) over expression was significantly common (43%) among synchronous patients. The mentioned case reported here was diagnosed after the patient underwent surgical staging for endometrial cancer.5
Case Report
A 27 years old female unmarried and nulliparous, presented with mass per abdomen since 2- months. History of occasional dull aching pain and occasional low back ache since 2-3 months. Evaluated in our hospital for the same diagnosed to have Synchronous Endometrial and Ovarian Carcinoma. All the biochemical parameters are within acceptable limits.
CT abdomen abdomen and pelvis showed well defined solid cystic lesion in right adnexa 12.5x7.8x9.7cm, solid component measuring 6.6x 7.6x 3cm, abutting right External iliac vessels, mid/distal ureters, and psoas, adjacent bowel loops - likely neoplastic etiology. Minimal free fluid.Serum CA125 concentration was- 297 U/mL (normal range <35 U/mL). CEA, AFP, Beta hCG, LDH - within normal limits.
She underwent Laparotomy and adhesiolysis and right salphingo-ovariotomy and frozen section and proceeded with fertility sparing surgical staging – omentectomy and right pelvic lymph node debulking and peritoneal cytology sampling done.Frozen section suggestive of malignant ovarian tumour.
Pathological findings shows- Endometroid Adenocarcinoma. Peritoneral omental fluid shows few malignant cells. Overall suggestive of Carcinoma Ovary stage IC with Endometrium Mucinous differentiation. Omentum
- Free.Lymph Nodes- 8 lymph nodes identified, all free. Few Lymph nodes show endometriosis. Peritoneal Fluid showed positive for malignant cells.
She is planned for Chemotherapy with Paclitaxel and Carboplatin (3 weekly) for 6 cycles. Received 3 cycles of adjuvant chemotherapy. She underwent Completion surgery for carcinoma ovary - laparoscopic adhesiolysis and total laparoscopic hysterectomy and left adnexectomy. Received three more cycles of adjuvant chemotherapy.
Pathology findings suggestive of Features are those of well differentiated endometrioid carcinoma, NOS -Uterus. Tumor is infiltrating less than half of total myometrial thickness. Numerous lymphovascular invasion seen. Histologic Grade: International Federation of Gynecology and Obstetrics (FIGO) Grading System - FIGO grade 1. Myometrial Invasion: Present.
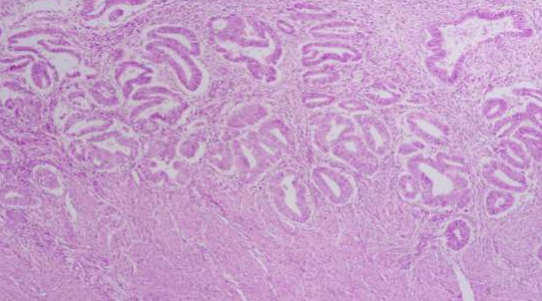
H and E images showing endometrial glands crowded and superficial invasion of myometrium
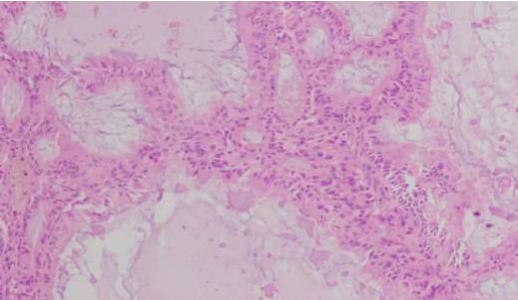
H and E images showing endometroid carcinoma with central mucin present.
After explaining diagnosis treatment outcomes acute and late side effects and consent is taken for Radiotherapy. She was planned and was treated to the planned target volume (External Beam Radiotherapy) to a dose of 4500cGy in 25 fractions along with adequate PTV margins by maintaining Organs at Risk according to the QUANTEC guidelines
She tolerated the treatment well without significant Radiation toxicities. Received adjuvant brachtherapy (HDR Intravaginal brachytherapy) prescribed to the vaginal surface to the dose of 1800cGy in 3 fractions.
Figure 1, Figure 2
Discussion
Synchronous endometrial and ovarian tumors are rare variants of gynecological cancers, and they must be differentiated from either primary endometrium or ovarian tumors with metastasis. The landmark criteria have been laid down by Ulbright and Roth, and later refined substantially by Scully et al.6
SEOCs are characterized by histological dissimilarity of the tumors, no or only superficial myometrial invasion of endometrial cancer, no vascular space invasion of endometrial and ovarian tumor, absence of other evidence of spread, ovarian unilateral tumor, ovarian tumor in the parenchyma and without involvement of the surface of the ovary, dissimilarity of molecular genetic or karyotypic abnormalities in the tumors, and different ploidy of DNA of the tumors.9 Young age, obesity, pre-menopausal status, and nulliparity were the distinct features among this rare entity. Three cases in perimenopausal and post menopausal age group has been reported by gynecological oncology unit at “Attikon” University Hospital, National University of Athens, Greece to be synchronous endometrioid endometrial and ovarian cancer.10
Conclusion
Synchronous endometrial and ovarian tumors are rare variants of gynecological cancers, and they must be differentiated from either primary endometrium or ovarian tumors with metastasis. The landmark criteria for diagnosing such cases have been laid down by Ulbright and Roth. Molecular biomarkers required for further identification and characterstics behind the pathogenesis of Synchronous endometrial and ovarian tumors.
References
1. Ree YS, Cho SH, Kim SR, Cho SH, Kim KT, Park MH. Synchronous primary endometrial and ovarian cancer with three different histologic patterns: a case report. Int J Gynecol Cancer. 2003; 13(5): 678-682.
2. Wang T, Zhang X, Lu Z, Wang J, Hua K. Comparison and analysis of the clinicopathological features of SCEO and ECOM. J Ovarian Res. 2019; 12(1): 10.
3. Grammatoglou X, Skafida E, Glava C, Katsamagkou E, Delliou E, Vasilakaki T. Synchronous endometrioid carcinoma of the uterine corpus and ovary. A case report and review of the literature. Eur J Gynaecol Oncol. 2009; 30(4): 437-439.
4. Makris GM, Manousopoulou G, Battista MJ, Salloum I, Chrelias G, Chrelias C. Synchronous endometrial and ovarian carcinoma: a case series. Case Rep Oncol. 2017; 10(2): 732-736.
5. Liu Y, Li J, Jin H, Lu Y, Lu X. Clinicopathological characteristics of patients with synchronous primary endometrial and ovarian cancers: a review of 43 cases. Oncol Lett. 2013; 5(1): 267-270.
6. Moro F, Leombroni M, Pasciuto T, et al. Synchronous primary cancers of endometrium and ovary vs endometrial cancer with ovarian metastasis: an observational study. Ultrasound Obstet Gynecol. 2019; 53(6): 827-835.
7. D?bska-Szmich S, Czernek U, Krakowska M, et al. Synchronous primary ovarian and endometrial cancers: a series of cases and a review of literature. Prz Menopauzalny. 2014; 13(1): 64-69.
8. Soliman PT, Slomovitz BM, Broaddus RR, et al. Synchronous primary cancers of the endometrium and ovary: a single institution review of 84 cases. Gynecol Oncol. 2004; 94(2): 456-462.
9. Song T, Seong SJ, Bae DS, et al. Prognostic factors in women with synchronous endometrial and ovarian cancers. Int J Gynecol Cancer. 2014; 24(3): 520-527.