The Non-Operative Treatment of Childhood Finger Injuries: Case Report
The Non-Operative Treatment of Childhood Finger Injuries: Case Report
Kassem El Houcheimi*
*Correspondence to: Kassem El Houcheimi, United Arab Emirates.
Copyright
© 2024: Kassem El Houcheimi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 December 2023
Published: 22 December 2023
The Non-Operative Treatment of Childhood Finger Injuries: Case Report
Introduction
Fractures and joint injuries are common. Although it is often seen as a minor injury, improper nail treatment can lead to serious consequences. These injuries can be chronic, harsh and debilitating; It is not difficult to overtreat stable fractures and neglect unstable bones; both can cause permanent disability. Accurate diagnosis and prompt treatment of these injuries remain the foundation of good hand care.
Treatment Principles
The aim of treatment in any finger injury is to restore the normal function of the finger. Restoration of bone tissue is important for rehabilitation; However, achieving this goal does not require anatomical reduction, especially at the expense of scar tissue and loss of movement. For early onset of hand function, bone development must be ensured through bone stabilization, splinting or internal fixation. Early mobilization prevents sliding tissue adhesions of the extensor and flexor tendon systems and prevents capsular contracture. Immobilization of the finger for more than 4 weeks will cause long-term stiffness due to scarring of the extensor tendons and capsule. For example, the sensitivity of the phalanx bone that does not heal with reduction and separation is followed by the joint after 3-4 weeks. Even if a joint needs a splint, the splint must be small enough to allow pain-free movement. Acquired cases usually have sufficient connective tissue to make them stable and easier to heal without inhibiting movement, even if there is a partial fracture in the bones or fingers next to the buddy band. Rotated or angular malpositioned fractures may be candidates for closed reduction and splinting, but these fractures are at risk for reduction and return deformity. These less stable bones require careful and frequent observation and radiographic evaluation. Surgical treatment is indicated for all broken fractures, open fractures, shortened or malrotated fractures, and fractures that do not close. Delayed recovery from these bone surgeries is always more difficult; stiffness results in decreased performance due to incomplete deformity and subsequent arthritis.
Diagnosis
Signs of injury are usually obvious: pain, swelling, tenderness, ecchymosis, deformity and/or skin abrasions. The differential diagnosis of finger injuries includes fractures, ligament ruptures, and lacerations or ruptures. Careful examination of flexor tendon, extensor tendon, and neurovascular function should be considered. Posterior, anterior (PA), side and oblique view display for trauma. When targeting a specific finger, lateral views of the injured finger should be obtained medial to the PA and PIP joint.
Principles of closed correction
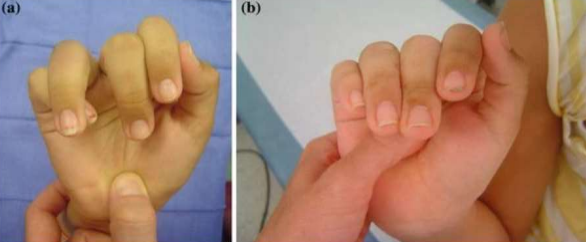
Reduction can be done with axial traction and the deformity can then be reversed. For the ankle joint, the muscle may relax from the MCP joint. When the recovery is complete, check this number to determine the stability of the recovery. Check rotation by moving your fingers, looking at the screw plane, and measuring finger overlap. All fingers should point to tuberculosis (Figure 1). one). If pain prevents active flexion, tenodesis and gentle wrist extension will allow finger flexion.
Figure 01 (a) This image shows a rotational malalignment of the ring finger (crossing over the small finger) from a fracture at the base of the proximal phalanx of the ring finger. Due to a fairly normal looking appearance of the hand with the fingers extended the injury was initially treated non-operatively. Notice the gap between the middle and ring fingers, and the deviation of the ring finger from the normal cascade. The patient was treated with an operative reduction and percutaneous pinning.
(b) A normal finger cascade with all fingers pointing toward the thenar eminence is seen in the same patient 4 weeks after surgery. Passive finger flexion is demonstrated using the tenodesis effect that occurs with passive wrist extension
A radial or ulnar groove type splint with MCP joint flexion as close to 90° as possible will maintain finger alignment during release and prevent joint ligament contracture. Although splinting at 90° MCP flexion is a better option, as long as 60° MCP flexion is sufficient to maximally affect ligamentous information and is easier to do. In the case of a stable, non-displaced fracture, "buddy taping" of the injured finger to the adjacent uninjured finger may be sufficient. There are six. Analysis of the sagittal relationship in the lateral view is often difficult, especially in casts, and a series of oblique radiographs may be needed to confirm that the relationship is well established. Follow-up with new radiographs should be performed 1 week after the start of reduction to confirm good maintenance relationship. A delay of more than 1 week in follow-up may make it difficult to track the decline.
Specific injury patterns
Distal Cluster Fracture
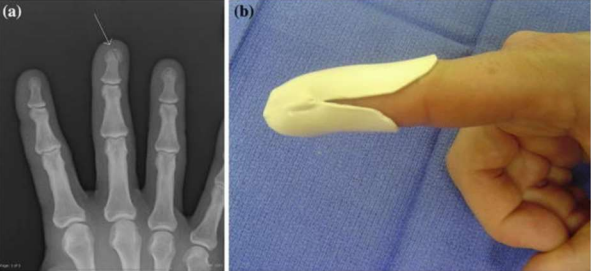
The most common hand fracture is the phalangeal bone extending into the hand, especially the thumb, index finger and middle finger. Because the deformation force of the distal phalanx is small, these types of fractures can often be treated with closed procedures such as simple splinting, closed reduction and splinting, or closed reduction and percutaneous fixation. splinting, while unstable transverse fractures are best treated with surgical fixation with longitudinal Kirschner wires or screws [1]. Even if the treatment is chosen for bone injury, damage to the affected tissue and nail bed will often not be ignored. Most of these are open injuries and should be based on the principles of treatment for open bones; for example: a class of antibiotics and optimization of devitalized tissue. Bed injuries should be treated by decompression of the subungual hematoma and resuturing of the nail bed laceration with well-absorbable sutures (e.g., 5-0 sutures). Proximal screws can be kept open by preventing damage to these structures and providing a temporary location if the entire screw plate must be removed [2]. Simple splinting for 3 weeks, including the DIP joint but excluding the PIP
(Figure 2). The action of DIP begins in 2-3 weeks and protection continues until pain is felt throughout the use period. Due to the damage to the fingertip as a principle of the body, patients should be warned that they will often experience loss due to hyperesthesia, cold sensitivity, and numbness even 6 months after the injury (1). Fibrous nonunion of bone can often result in functional impairment
Figure 02 (a) AP radiograph showing a distal tuft fracture (arrow) (b) Typical clamshell splint used to protect a tuft fracture
Hammer Fracture
Most distal phalanx base fractures are "hammer injuries" that occur due to disruption of the distal extensor mechanism due to axial loading. Continuous DIP splinting for 8 weeks followed by nightly splinting for 1 month may be effective in treating mallet syndrome with or without fracture [3]. Immobilization with dorsal, volar or prefabricated Stack type splinting is a suitable treatment method (Figure 3). Care should be taken when immobilizing the DIP joint in the hyperextension position to avoid dorsal skin ischemia and potential damage.
Figure 03 (a) Lateral radiograph of a mallet fracture (b) Dorsal splint used for mallet finger (soft tissue or bony mallet). Notice slight extension pre-bent into splint to assist in reduction of the avulsed fracture fragment seen in Fig. 3a. Patients treated with dorsal splints should be examined frequently for dorsal skin breakdown under the splint
When the fracture is protected with the extensor muscle, the chance of healing increases as the bone can heal better than the muscle, but x-rays must be taken together to ensure integrity. The PIP must remain free because the combination of the PIP joint and its possible stiffness can cause more pain than the original injury. Patients are advised to expect a slight extensor lag (5° to 10°) and a slight loss of full range of motion in the best-case scenario. If the dorsal hammer deformity after splinting exceeds 20°, the splinting plan needs to be repeated for one or two months. A long hammer injury can of course become bone stabilized within 3 months [4]. still. Open reduction carries a significant risk of complications, so reduction using K-wires if possible and fixation with percutaneous internal fixation is the procedure of choice. Various lead configurations have been shown to be safe and effective as long as resetting the DIP connector is confirmed on the X-ray side [5, 6].
Middle and proximal phalanx body fractures
Treatment of proximal and middle phalanx extra-articular fractures can be done by dividing these injuries into non-dominant and non-survivable bones. Most nonunion fractures can be treated with partner taping and range of motion for 3-4 weeks. Attention should be paid to stability after closed reduction to remove broken bones. For fractures or other unstable bones, isolation may be attempted, but follow-up is necessary to assess subsequent changes (Figure 4).
Figure 04 AP radiograph of a long oblique fracture of the proximal phalanx. The inherent instability of the fracture pattern will lead to suboptimal finger function if treated non-operatively.
Even if reduced, the fracture will be unstable and difficult to reduce. Oblique, spiral, or comminuted fractures between the diaphyseal bones tend to be unstable, whereas once fractures in adults or Salter II metaphyseal fractures in children tend to be stable. Rotation of bones in adults occurs at the base of the proximal phalanx. Pulling of the internal and external muscles causes the fingers to lengthen, resulting in bone extension-type deformity at the fracture site. While the bones of the middle phalanx distal to the attachment site of the flexor superficial (FDS) muscle will be deformed equally, the bones near the attachment location of this muscle will be deformed at an angle to the apex.
Metacarpal Fractures
As with phalanx fractures, stable, localized metacarpal fractures can often be treated with simple closed reduction and splinting. The intermetacarpal ligament is a strong ligament that connects between each metacarpal head and prevents movement of weak bones. The most common hand fracture is a fracture of the metacarpal neck of the little finger, known as a "boxer's fracture" (Figure 5).
Figure 05 Lateral radiograph of a boxer’s fracture (arrow)
Traditional teaching allows for conservative management of metacarpal neck fractures with the following degree of apex dorsal angulation: small finger: 40–50°, ring finger: 30°, middle finger: 20°, index finger: 30°, middle finger: 20°, index finger: 10°. An external radiograph of the hand can measure the dorsal or circumferential aspect of the apex of the fracture site. Cadaveric studies have shown that oblique views are misleading and often exaggerate the true angle of the fracture [7]. Failure to reduce the dorsal apex angle will cause changes in the MCP joint on the dorsum of the hand. A recent retrospective review evaluated three different casting techniques for clinical closure of the extra metacarpal bone: a cast group with MCP fusion when allowance was made for the entire interphalangeal (IP) joint, and another group cast with the MCP joint in extension and extension. . The authors found no differences between groups in reducing bone loss, finger range of motion, or grip strength [8]. Deformity is acquired. Minor rotations of the fingers should be carefully evaluated, as swelling of the fracture site in the fourth abdominal cavity may cause visible rotation deformity. Additionally, recent data from cadaveric experiments have shown that metacarpal shortening of up to 1 cm will cause an almost 50% decrease in grip strength [9]. A postoperative complication in the treatment of metacarpal fracture by reduction, percutaneous nailing, or open reduction and internal repair is adhesions of the overlying extensor tendon. To minimize the effects of extensor tendon adhesions, adequate immobilization should be provided to allow early finger movement.
Treatment Tips
Correct identification of finger injuries requiring surgery is as important as treatment of stable fingers. Attempting to withhold treatment for these injuries will delay appropriate care, often affecting the final outcome (Figure 1). and study well. Fractures that are at risk for this deformity include oblique and spiral fractures, as well as comminuted fractures that prevent the broken bone from passing through the bone. As mentioned above, it is important to carefully evaluate changes in the injured finger to avoid a difficult deformity. The condition called “Jersey finger” refers to avulsion of the distal insertion point of the flexor digitorum profundus (FDP) tendon from the volar aspect of the distal phalanx. These injuries range from avulsion with mild retraction of the FDP tendon, to avulsion fractures of the tendon, to dorsal subluxation of the distal phalanx after avulsion injury. Due to the need for reduced body stability and immobilization as well as the need for early physical care to prevent long-term stiffness, referral to a specialist is necessary when these injuries are diagnosed or suspected [5]. Intra-articular injuries involving IP joints and MCP joints are associated with permanent stiffness and often result in long-term functional deficits in the injured joint. Like most fractures, these injuries require physical reduction, immobilization, and early intervention. Appropriate triage and referral for these fractures are critical to achieving long-term outcomes.
Conclusion
Fractures of the phalanx and metacarpal bones are common injuries. Initial evaluation of these injuries requires good radiographs to identify the injury and determine appropriate treatment: failure to avoid surgery. A stable bone with no rotational deformity or attachment at the joint is the best treatment for failure, including reduction, appropriate splinting, and early support for bone healing without any debris. Cluster fractures, hammer toe fractures, and boxer fractures are examples of injuries that are easier to treat with care rather than surgery. Bones that fail to heal properly, including residual deformity, intra-articular extension, or tendon injuries, are referred to a specialist for early treatment.
References
1. DaCruz DJ, Slade RJ, Malone W. Fractures of the distal phalanges. J Hand Surg [Br] 1988;13:350–2.
2. Brown RE. Acute nail bed injuries. Hand Clin 2002;18:561–75. Article PubMed Google Scholar
3. Kalainov DM, Hoepfner PE, Hartigan BJ, et al. Nonsurgical treatment of closed mallet finger fractures. J Hand Surg [Am] 2005;30:580–6. Article Google Scholar
4. Patel MR, Desai SS, Bassini-Lipson L. Conservative management of chronic mallet finger. J Hand Surg [Am] 1986;11:570–3. CAS Google Scholar
5. Lubahn JD, Hood JM. Fractures of the distal interphalangeal joint. Clin Orthop Relat Res 1996;327:12–20.
6. Badia A, Riano F. A simple fixation method for unstable bony mallet finger. J Hand Surg [Am] 2004;29:1051–5. Article Google Scholar
7. Lamraski G, Monsaert A, De Maeseneer M, et al. Reliability and validity of plain radiographs to assess angulation of small finger metacarpal neck fractures: human cadaveric study. J Orthop Res 2006;24:37–45. Article PubMed CAS Google Scholar
8. Tavassoli J, Ruland RT, Hogan CJ, et al. Three cast techniques for the treatment of extra-articular metacarpal fractures. Comparison of short-term outcomes and final fracture alignments. J Bone Joint Surg Am 2005;87:2196–201. Article PubMed Google Scholar
9. Meunier MJ, Hentzen E, Ryan M, et al. Predicted effects of metacarpal shortening on interosseous muscle function. J Hand Surg [Am] 2004;29:689–93. Article Google Scholar.