Effectiveness of Post Operative Analgesia via Ultrasound Guided Transversus Abdominis Plane Block after Lower Segment Cesarean Section
Effectiveness of Post Operative Analgesia via Ultrasound Guided Transversus Abdominis Plane Block after Lower Segment Cesarean Section
DHRUVA PATEL* 1 , MAULI K. GANDHI 2 ,YATI SHARMA 3
1Third Year Resident, Department of Anaesthesia, SMT NHL Municipal Medical College and SVP Hospital, Ahmedabad, Gujarat, India.
2 Assistant Professor and PG Guide, Department of Anaesthesia, SMT NHL Municipal. Ahmedabad, Gujarat, India.
3First year resident, department of Anaesthesia SMT NHL Municipal medical college and SVP Hospital ,Ahmedabad, Gujarat ,India.
*Correspondence to: Dr. Dhruva Patel, Third Year Resident, Department of Anaesthesia, SMT NHL Municipal Medical College and SVP Hospital, Ahmedabad, Gujarat, India.
Copyright
© 2023 Dr. Dhruva Patel. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 July 2024
Published: 15 July 2024
Abstract
INTRODUCTION :
Pain is an unpleasant emotional and sensory experience. After cesarean section good post- operative analgesia for mother is important for optimal care of her neonate, effective breast feeding and also reduce risk of thromboembolic disease, respiratory complications & reduce hospital stay. The purpose is to compare the post-operative analgesic effectiveness of ULTRASOUND GUIDED TRANSVERSUS ABDOMINIS PLANE BLOCK- after lower segment cesarean section over use of intravenous analgesic drugs.
OBJECTIVES :
Primary objectives: -
1) To assess the degree of analgesia achieved by ultrasound guided transversus abdominis plane block.
2) To assess the duration of analgesia achieved by ultrasound guided transversus abdominis plane block.
Secondary objectives: -
To assess the requirement of rescue analgesia after transversus abdominis plane block with-in 24 hours.
MATERIAL AND METHOD :
All 60 participants of physical status ASA II-III who are under going non urgent lower segment cesarean section are included in the study under spinal anesthesia.
They were divided into two groups 30 each randomly into GROUP T & GROUP C, from which group T received ultrasound guided TAP block bilaterally with INJ BUPIVACIANE 0.25% ,20 ML on each side ( total 40 ML ) after procedure is completed while group C will receive normal from iv analgesia INJ DICLOFENAC 75 MG just after end of the procedure. Both the groups were assessed for degree and duration of analgesia using VAS SCORE and also requirement for rescue analgesia for 24 hours.
RESULT :
The Result of the study demonstrated that TAP block was very effective in reducing pain and demand of post operative analgesia was reduced.The duration of analgesia was significantly prolonged in group T as compared to group C.Time for rescue analgesia in the study group was prolonged from 4 h to 9.5 h (P = 0.015831).
CONCLUSION :
The results of this study demonstrated that TAP block without any supplementations of iv analgesia was effective in reducing the severity of pain, delayed the demand of first postoperative analgesic and reduced the need of rescue analgesia during 24 hours and prevent complications like PONV and were more satisfied compared to those who did not receive TAP BLOCK with p value <0.0001.
Keywords: Caesarean section, multimodal analgesia, Bupivacaine, Transversus Abdominis Plane block.
Effectiveness of Post Operative Analgesia via Ultrasound Guided Transversus Abdominis Plane Block after Lower Segment Cesarean Section
Introduction
The number of cesarean deliveries has almost doubled between 2000 and 2020, acute pain intensity related to this procedure is often underestimated. Post-operative pain if treated well will lead to decrease in mortality and morbidity rates, as severe pain may lead to anxiety in mothers, delayed ambulation, delay in immediate breast feeding of neonates, tachyarrhythmia, hypertension and many other complications in cardiovascular and respiratory systems of the body.
At present,analgesia is used with intravenous and intramuscular- opioids, NSAIDs and neuraxial blocks with opioids. However, unwanted side effects like sedation, nausea, vomiting, pruritus, occasionally respiratory depression remains with usage of opioids.
Recently regional anesthesia is one of the safe and effective methods for post-operative analgesia like skin infiltration, combined spinal-epidural analgesia, truncal blocks, ultrasound guided transversus abdominis plane (TAP) block. TAP block is a regional anesthesia technique and is one of the most effective methods for providing analgesia after lower abdominal surgeries.
An increasing number of trials and case-reports have highlighted the post-operative analgesic effectiveness of ultrasound guided transversus abdominis plane block after lower segment cesarean section over use of other multimodal analgesic drugs.
Materials and Methods
Study design:
After obtaining institutional ethics committee approval and Clinical Trial Registry of India registration, this prospective randomized controlled study was conducted from June 2021 to December 2021. 60 patients of American society of anesthesiologist’s physical status (ASA PS) II-III who were undergoing elective lower segment cesarean section (LSCS).
Exclusion Criteria:
- Patients with coagulopathy.
- patients with contraindication of spinal anaesthesia.
- patients with allergies to local anaesthetic drugs.
- Pregnancy related complications like pregnancy induced hypertension and gestational diabetes mellitus.
Sample size was determined prospectively using data from previous cesarean sections performed under spinal anesthesia in our institution. A total of 120 patients were assessed for eligibility and 60 patients were enrolled. We considered 30% prolongation of total post op analgesia with TAP block.
After obtaining written informed consent, study was done by double blinded randomised control trial.
Pre anesthetic check-ups were carried out in all patients. After checking adequate hours of nil by mouth, arrival to operation theater intravenous line was taken and co-loading with ringer’s lactate 10-15 ml/minutes was started. Electrocardiograph, noninvasive blood pressure and pulse oximetry were attached and baseline parameters were recorded. All participants received spinal anesthesia under all aseptic precautions with inj. bupivacaine 0.5% (heavy) 2.0 ml.Duration of study was 1.5 -2 hours. After completion of surgery, skin closure and dressing all participants in Group-T received ultrasound guided bilateral TAP block with isobaric inj. bupivacaine 0.25% 20 ml on each side and participants in Group-C received intravenous diclofenac 75 mg.
Ultrasound guided TAP block was performed by senior resident and/or consultant who was experienced for ultrasound guided regional anesthesia. Spinal needle is inserted in the plane of the transducer directly under the probe and advanced, until it reaches the plane between the internal oblique and transversus abdominis muscles. The probe follows the needle entry point medially in its superficial path and then returns to its original position as the needle is directed deeper. Upon reaching the plane 3 ml of normal saline is injected to confirm the correct needle placement, following careful negative aspiration 20 ml of the local anesthetic solution on each side was injected observing for an elliptical separation between the two fascial layers. The transversus abdominis plane was visualized expanding with the injection as a hypoechoic space.
Figure 4
Patients in group T were monitored for local site infection, hematoma formation, local anesthesia toxicity, peritoneal and bowel perforation. Patients in group C will be monitored for gastric irritation.
The assessment of the intensity of the pain post-operatively after transfer of patients to post- operative anesthesia care unit (PACU). Each patient was assessed every 2, 4, 6, 8, 12, 18 and 24h by an independent observer who was unaware of the group allocation for degree of pain using visual analogue scale (VAS) score. Visual analogue scale was explained to the patients, a 10- point horizontal line was used as a scale, on which point on the left indicates no pain (0 point) and the point on the right end indicated a level of unbearable pain (10 points). The patients were asked to mark the level of the experienced pain on the scale. The VAS score recorded in the recovery room immediately after the transfer of the patients to PACU will be accepted as the time 0, and the VAS scores of each patient was recorded on the post-operative 2, 4, 6, 8, 12 and 24 hours. Rescue analgesia will be given if the vas score will be >4.
Total duration of analgesia (from T0 to when the patient's VAS score was >4)was observed as a primary outcome. Analgesic efficacy of TAP block by VAS score and total number of rescue analgesia till 24 hours post-operative were assessed as secondary outcomes.
Demographic data were analyzed using Student’s t?test or Fisher’s exact test as appropriate. The comparison of total dose of rescue analgesic requirement, time to first analgesic administration and VAS between the two groups was done by paired t?test. Confidence interval in this study was 95%. P < 0.05 was considered statistically significant.
Results
The result of the study demonstrated that TAP block was effective in reducing pain, delayed the demand of first post- operative analgesic and reduced the need of rescue analgesic doses during the first 24 hours after surgery in patients undergoing cesarean section under spinal anesthesia. The duration of analgesia was significantly prolonged in group-T as compared to group-C (16.407±6.783 vs. 5.630±1.75, p=0.0001). Number of 4 (14.8%) patients had nausea and number of 3 (11.1%) patients had vomiting in group-C while in group-T there were no nausea and vomiting and any other complications.
Sixty patients were recruited in the study, of these thirty were randomized to undergo TAP block with INJ BUPIVACIANE 0.25% ,20ML on each side ( total 40 ML ) and remaining 30 with INJ DICLOFENAC 75MG IV.
TABLE 1: DEMOGRAPHIC DATA
|
VARIABLES |
GROUP T (N=30) |
GROUP C (N=30) |
P VALUE |
|
AGE (YEARS) |
22.6±6.3 |
23.2±6.2 |
0.453 |
|
Weight (kg) |
62.5±4.2 |
64.4±4.5 |
0.564 |
|
ASA© (%) II-III |
66.7 |
40.7 |
0.432 |
|
33.3 |
59.3 |
0.324 |
|
|
Heart rate (/min) |
75.5±6.2 |
78.5±6.5 |
0.453 |
|
Mean arterial pressure (mmHg) |
101.64±7.2 |
103.7±7.5 |
0.654 |
Demographic profile, pulse, blood pressure and saturation were comparable in both groups. Demographic data is not significant in our study (P value>0.05).
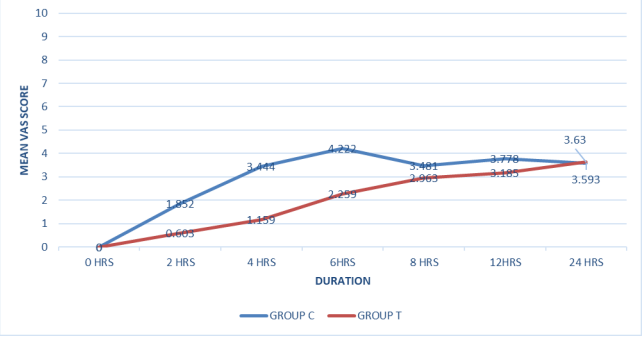
Figure 1: Comparison of VAS score
In patients receiving TAP block with 0.25% Bupivacaine (Group T), the requirement for analgesic significantly reduced as compared to those who received the Inj. Diclofenac 75mg iv (Group C).VAS was noted at 2, 4, 6, 8, 12, 18 and 24 h. VAS was reduced after TAP block with 0.25% Bupivacaine for the first 8–10 h post?operatively as compared to patients receiving Inj. Diclofenac 75mg iv. [Figure 1]
In this study, Analgesic efficacy of ultrasound guided TAP block was studied by VAS SCORES at 0,2,4,6,8,12, 24 hours respectively. The results were statistically significant at 2,4,6,8 hours and not significant at 12 and 24 hours (figure 1).
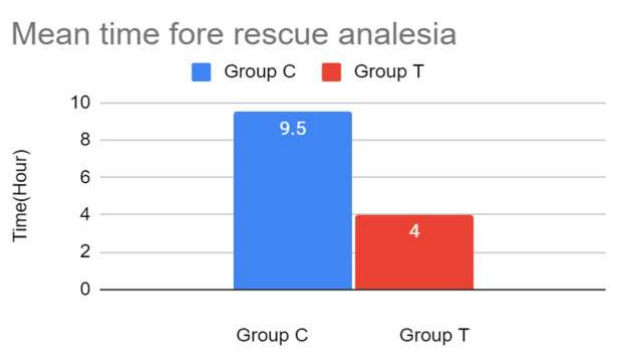
Figure 2: Total duration of post-operative time analgesia
This above graph showed that the first dose of rescue analgesia was required in group C was 4 hours later in postoperative period whereas, first dose of rescue analgesia was required in group T was 9.5 hours later in post operative period.P=0.0163.
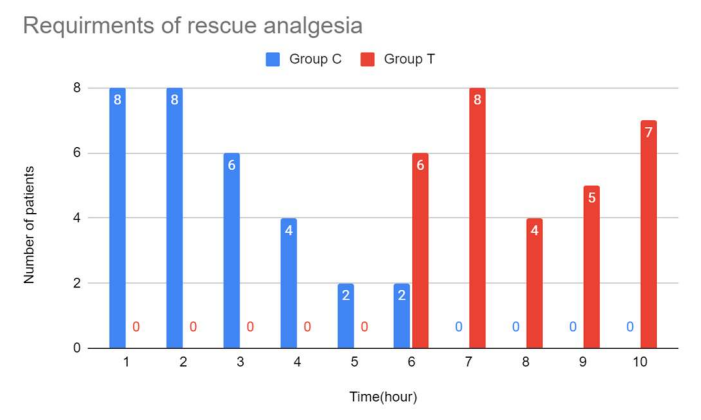
Figure 3: Requirements of rescue analgesia
In the above mentioned chart, in group T, the number of patients required rescue analgesic dose till the first 5 hours postoperatively were zero. After 6 hours postoperatively 6(20%) patients required the first dose of rescue analgeia. At 7,8,9,10 hours postoperatively the number of patients required rescue analgesic dose were 8(26.67%),4(13.33%),5(16.67%),7(23.33%) respectively. Whereas, in group C the number of patients required rescue analgesic dose at 1,2,3,4,5,6 hours of postoperative period were (26.67%), 8(26.67%), 6(20%), 4(13.33%), 2(6.67%), 2(6.67%) respectively. So in our study less number of patients in group T were required rescue analgesia dose in compared to group C patients in the initial 5 hours of postoperative period.
Discussion
The results of our study show that TAP block when used as part of multimodal analgesic regimen after cesarean delivery delayed time for rescue analgesia, reduced requirement of opioid analgesic and decreased VAS. Multimodal analgesia is an established technique for controlling post-operative pain. Multimodal analgesia provides better results by combining various drugs with different duration, and onset of action also reduces the side effects of individual drugs.[2]
Epidural analgesia is a good alternative for post-operative pain relief, but the gravid uterus making it difficult to identify the space. Furthermore, it may not be preferred in case of emergency cesarean section. Infiltration of local anaesthetic is also used to provide pain relief, but it is not effective for prolonged analgesia.[4]
Ultrasound guided Transversus abdominis plane block is a relatively new abdominal nerve block with excellent efficacy and greater margin of safety compared to landmark technique for a variety of abdominal surgeries including cesarean section. TAP block involves the injection of LA in between the transverse abdominis muscle and internal oblique muscle. TAP block can also be given using anatomical landmarks(iliac crest) by first identifying a triangle of petit. The USG probe was placed transverse to the abdominal wall which made the three muscle layers distinctly visible after which the probe was moved to the mid-axillary line just above the iliac crest (i.e., over the triangle of Petit). The needle was then advanced medially by in-plane approach. This is referred to as the posterior approach. This approach is used in our study.
TAP block has been used for various abdominal procedures other than caesarean section such as large bowel resection, open/laparoscopic appendectomy, total abdominal hysterectomy, laparoscopic cholecystectomy, open prostatectomy, abdominoplasty with or without flank liposuction, inguinal hernia and iliac crest bone graft. The TAP has poor vascularity, and hence the action is prolonged and not associated with any major complications. This interfacial plane contains the intercostal,subcostal,iliohypogastric and ilioinguinal nerve.These nerves give sensation to anterior and lateral abdominal walls and parietal peritoneum at T5-L1 level. This procedure blocks these nerves depending upon at what level the block is given and how much spread of local anaesthetic drug. TAP block provides only somatic and not visceral analgesia. TAP block is a part of multimodal analgesia in abdominal surgeries because of its safety, ease and effectiveness on postoperative analgesia.
The result of this study demonstrated that TAP block was effective in reducing pain, delayed the demand of first postoperative analgesic and reduced the need of rescue analgesia during the first 24 hrs after cesarean section under spinal anesthesia even if given as solitary analgesic drug.
In this study, the mean of duration of analgesia in group-T was 16.7 hours as compared to group-C 5.6 hours. In the study done by Srivastava U et al[7], median time to first rescue analgesia in control group was 6.5 hours while in study group (TAP block with 20ml 0.25% bupivacaine on each side using landmark technique) was 12 hours.
In the study done by Mankikar MG et al[5], ropivacaine 0.5% 15ml in group-S and in group-c normal saline in usg guided TAP block. Time to first analgesic administration was prolonged significantly in Group S (mean - 9.5 h) as compared to Group C (mean - 4 h).
Degree of analgesia was measured by visual analogue scale of 10, with 10/10 score taken as maximum pain, and 0/10 taken as no pain.
In our study vas score was recorded at 0,2,4,6,8,12,24 hours mean vas score at 2,4,6,8 hours in Group T compared to Group C were statistically significant.
In a study done by Dr. Shrivastava et al. (2015)[7] studied the mean vas score at 0,4,8,12,24, 36 and 48 hours respectively the vas score was statistically significant at 0,4,8,12,and 24 hours were not statistically significant at 36 and 48 hours.
Conclusion
The USG guided TAP block with prolong total duration of post-operative analgesia, reduce doses of rescue analgesic without side effects.
Source of Support: Nil
Conflict of Interest: None Declared
Reference
1. Adeniji AO, Atanda OO. Randomized comparison of effectiveness of unimodal opioid analgesia with multimodal analgesia in post-cesarean section pain management. J Pain Res. 2013;6:419–24. [PMC free article] [PubMed] [Google Scholar]
2. Belavy D, Cowlishaw PJ, Howes M, Phillips F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009 Nov;103(5):726-30. doi: 10.1093/bja/aep235. Epub 2009 Aug 22. PMID: 19700776.
3. Gupta A, Gupta A, Yadav N. Effect of dexamethasone as an adjuvant to ropivacaine on duration and quality of analgesia in ultrasound-guided transversus abdominis plane block in patients undergoing lower segment cesarean section - A prospective, randomised, single-blinded study. Indian J Anaesth 2019;63:469-74.
4. Jadon A, Jain P, Chakraborty S, Motaka M, Parida SS, Sinha N, Agrawal A, Pati AK. Role of ultrasound guided transversus abdominis plane block as a component of multimodal analgesic regimen for lower segment caesarean section: a randomized double blind clinical study. BMC Anesthesiol. 2018 May 14;18(1):53. doi: 10.1186/s12871-018-0512-x.
5. Mankikar MG, Sardesai SP, Ghodki PS. Ultrasound-guided transversus abdominis plane block for post-operative analgesia in patients undergoing caesarean section. Indian J Anaesth. 2016;60(4):253-257. doi:10.4103/0019-5049.179451
6. Mankikar, Maitreyi Gajanan & Sardesai, Shalini Pravin & Ghodki, Poonam Sachin (2016). Ultrasound-guided transversus abdominis plane block for post-operative analgesia in patients undergoing caesarean section. Indian Journal of Anesthesia. 60.253. 10.4103/0019- 5049.179451.
7. Srivastava U, Verma S, Singh TK, Gupta A, Saxsena A, Jagar KD, Gupta M. Efficacy of trans abdominis plane block for post cesarean delivery analgesia: A double-blind, randomized trial. Saudi J Anaesth. 2015 Jul-Sep;9(3):298-302. doi: 10.4103/1658-354X.154732
8. Yu N, Long X, Lujan-Hernandez JR, Succar J, Xin X, Wang X. Transversus abdominis-plane block versus local anesthetic wound infiltration in lower abdominal surgery: A systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2014;14:121. [PMC free article] [PubMed] [Google Scholar.