Late Onset Bilateral Foot Drop with Sphincteric Unconrolled due to Lumbar Discopathy with Dramatic Improvement Post Operatively.
Late Onset Bilateral Foot Drop with Sphincteric Unconrolled due to Lumbar Discopathy with Dramatic Improvement Post Operatively.
Dr. Abdulrahim H. Zwayed (M.B.Ch.B., Ph.D., F.I.C.S., F.A.C.S.) 1*, Dr. Enas Hasan 2, Dr Abdulrazek Ahmed Abdulrazek 3, Dr. Mohammed Mohsin Damudi 4,Dr Maen Al Mansour 5, Dr. Yasser Abdul Raziek 6
1,2.Department of Neurosurgery, Sohar Hospital, Sultanate of Oman.
3,4, 5. Anaesthesia: Sohar Hospital, Sultanate of Oman.
6. Radiology: Sohar Hospital, Sultanate of Oman.
*Correspondence to: Dr. Abdulrahim-Rahim H. Zwayed (Ph.D.) Department of Neurosurgery, Sohar Hospital, Sultanate of Oman.
Copyright
© 2024 Dr. Abdulrahim-Rahim H. Zwayed, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 July 2024
Published: 20 July 2024
DOI: https://doi.org/10.5281/zenodo.12793868
Abstract
Foot drop is defined as the weakness of the foot and ankle dorsiflexion. Acute unilateral foot drop is a well-documented entity, whereas bilateral foot drop is rarely documented. Bilateral foot drop due to disc herniation is extremely rare.Here we present a case of late onset bilateral foot drop due to disc herniation. The patient was a 42-year-old man presented with late onset bilateral foot drop after 2 weeks, with sign of the cauda equina syndrome as sphincteric uncontrolled. Lumbar magnetic resonance imaging of the patient revealed L2-3-disc herniation.
To our knowledge, this is a rare presentation for a case of bilateral foot drop with signs of cauda equina syndrome caused by L2-3-disc herniation. We performed urgent operation as decompressive laminectomy and extrude disc materials were excised. The patient was recovered with favorable outcome.
Keywords: Bilateral foot drop, lumbar disc herniation, surgery.
Late Onset Bilateral Foot Drop with Sphincteric Unconrolled due to Lumbar Discopathy with Dramatic Improvement Post Operatively.
Introduction
Foot drop is defined as weak anterior tibialis, extensor hallucis longus and extensor digitorum longus muscles which manifests as significant weakness of the foot and ankle dorsiflexion. [1,3,4]
In particular, slow progressing bilateral foot drop occurs with various metabolic causes as in anorexia nervos,hypothyroid myopathy, Chron's disease, and post electroconvulsive therapy,Parasagittal intracranial pathologies and cauda equine may also cause progressive bilateral foot drop.(3,5)
Acute unilateral foot drop is a well-known entity.[2,3]
On the other hand, acute bilateral foot drop in progressive fashion is rare but late onset bilateral foot drop with dramatic improvement is something unique.
Case Report
This is a 42-year-old man presented with history of chronic back pain with an attack of acute exacerbation as severe backache and bilateral foot drop developed while he was lifting a heavy weight. He presented to emergency room 2 weeks after the onset of symptoms. He had mild, non-specific back pain for 3 years previously.
Clinical examination revealed bilateral positive leg raising test at 30° and bilateral foot drop was documented (muscle strength was 1/5 in both foot dorsiflexion and big toe extension bilaterally). Hypoesthesia of both L3 dermatomes was also there. Perianal sensation was less with sphincteric uncontrolled to bladder and bowel functions.
All deep tendon reflexes were normal and no upper motor neuron signs were identified. All other muscle strengths and neurological tests were normal.
Apart from essential hypertension, his past medical history was otherwise unremarkable. Blood tests measured were normal or negative.
He had neither a history of recent surgery nor exposure to toxins or heavy metals.
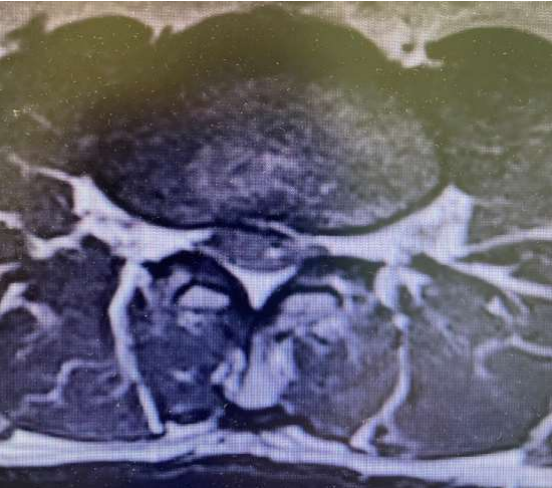
Emergent lumbar spinal magnetic resonance imaging (MRI) was obtained and revealed large extrude disc fragment at L2-3 level.
(Figure 1) with evidence of bilateral compression of L3 foramina
Figure 1
Fig 2: Axial view showing L2/L3 Discopathy with compression
The patient underwent urgent surgery 2 weeks after the initiation of the foot drop. Bilateral L3 decompressive laminectomy was performed and a large extruded central disc fragment causing bilateral neural foraminal obliteration was excised microsurgically.
Postoperatively his bilateral foot drop improved progressively. At the time of discharge (postoperative fifth day), ankle dorsiflexion and big toe extension both improved to 4/5 bilaterally.
His neurological examination at the first postoperative month was completely normal.
Discussion
Foot drop is defined as the weakness of the anterior tibialis muscle and is frequently accompanied by weakness of the extensor hallucis longus and extensor digitorum longus. Foot drop results from a disruption in the neural pathway starting from parasagittal cortical motor neurons to the spinal cord upper motor neurons and the peripheral spinal cord roots and ending with the peroneal nerve. It is usually caused by lower motor neuron pathologies, commonly disruption of the conduction from deep peroneal nerve (L2-3). (1,4,6,8)
L2-3 radiculopathy is a common cause of foot drop, usually caused by disc herniation of foraminal stenosis. [1].
Furthermore, lumbar disc herniation may cause cauda equina syndrome which leads to foot drop. But in this condition, foot drop is mostly unilateral, almost always progressive and associated with loss of function of the bowel, bladder, and sexual functions.[2,3]
Other common etiologies include local peroneal nerve damage due to trauma, entrapment, compartment syndrome, and tumor.[9,10,11]
Systemic diseases such as diabetes, vasculitis, connective tissue, and autoimmune disease may also be the etiological cause.[8,12].
In these circumstances, foot drop is almost always unilateral.
An isolated bilateral foot drop is a very rare condition and occurs with various metabolic conditions such as anorexia nervosa, hypothyroid myopathy, Chron's disease, and post electroconvulsive therapy. Also, intracranial pathologies such as parasagittal tumors may also cause bilateral foot drop.[3,5,] .
However, in these conditions, foot drop is in progressive nature. A sudden onset of bilateral foot drop is an extremely rare condition. [7,11]
Our patient who presented with history of chronic back pain with an attack of acute exacerbation as severe backache and bilateral foot drop developed while he was lifting a heavy weight.
He presented to emergency room 2 weeks after the onset of symptoms. He had mild, non-specific back pain for 3 years previously.
MRI proved to have a large extrude disc fragment at L2-3 level.
with evidence of bilateral compression of L3 foramina.
So, he underwent emergent L2-3 laminectomy and a large extruded disc material was removed.
The patient recovered well in the postoperative period.
The patient presented in our report had an acute L2-3-disc herniation which was the cause of acute bilateral foot drop. This patient had signs and the symptoms of the cauda equina syndrome. As to our knowledge, this is the first case of L2-3-disc herniation causing acute bilateral foot drop with association of cauda equina syndrome. In this condition, acute radiculopathy associated with bilateral L3 root may occur as a result of L2-3 disc herniation causing bilateral foot drop.
Although the L1 nerve root situated laterally to the cord and the remaining nerve roots are arranged in an appropriate order, respectively, where L5 nerve root is situated at the most medial side around the cord. We can explain with anatomical localization that L2-L3 disc herniation compressed both L5 nerve roots and leaded to bilateral acute foot drop.(10)
A rapid onset of spinal nerve root compression may cause more serious effect on the function than a progressive compression. However, the recovery is also more rapid after early decompression of the acute compression. [9]
The patient was recovered well after early decompressive surgery.
In conclusion, acute bilateral foot drop is an extremely rare entity. L2-3 disc herniations may be the cause. In this situation, emergent lumbar spinal MRI with extension to lower lumbar vertebrae is recommended. Early surgery may prevent catastrophic neurological sequels and have favorable outcome (10)
Reference
1. Bartels RH, de Vries J. Hemi-cauda equina syndrome from herniated lumbar disc: A neurosurgical emergency? Can J Neurol Sci. 1996; 23:296–9.
2. Chang HS, Nakagawa H, Mizuno J. Lumbar herniated disc presenting with cauda equina syndrome. Long term follow up of four cases. Surg Neurol. 2000; 53:100–5.
3. Eskandary H, Hamzei A, Yasamy MT. Foot drop following brain lesion. Surg Neurol. 1995;43:89–90. [PubMed] [Google Scholar]
4. Gariballa SE, Gunashekhar NP. Bilateral foot drop, weight loss and rectal bleeding as an acute presentation of Crohn's disease. Postgrad Med J. 1994;70:762–3.
5. Katirji B. Peroneal neuropathy. Neurol Clin. 1999;17:567–91.
6. Kershenbaum A, Jaffa T, Zeman A, Boniface S. Bilateral foot drop in-patient with anorexia nervosa. Int J Eat Disord. 1997;22:335–7.
7.Iizuka Y, Iizuka H, Tsutsumi S, Nakagawa Y, Nakajima T, Sorimachi Y, et al. Foot drop due to lumbar degenerative conditions: Mechanism and prognostic factors in herniated nucleus pulposus and lumbar spinal stenosis. J Neurosurg. Spine. 2009; 10:260–4.
8. Mahapatra AK, Gupta PK, Pawar SJ, Sharma RR. Sudden bilateral foot drop: An unusual presentation of lumbar disc prolapse. Neurol India. 2003;51:71–2.
9. Olmarker K. Spinal nerve root compression. Nutrition and function of the porcine cauda equine compressed in vivo. Acta Orthop Scand Suppl. 1991; 242:1–27.
10. Oluigbo CO, Qadri SR, Dardis R, Choksey MS. Lumbar canal stenosis presenting with acute bilateral foot drop. Br J Neurosurg. 2006; 20:87–9.
11. Papapostolou A, Tsivgoulis G, Papadopoulou M, Karandreas N, Zambelis T, Spengos K. Bilateral drop foot due to thoracic disc herniation. Eur J Neurol. 2007;14.
12. Stewart JD. Foot drop: Where, why and what to do? Pract Neurol. 2008;8:158–69.