Health-Related Quality of Life in Patients with Pulmonary Arterial Hypertension
Health-Related Quality of Life in Patients with Pulmonary Arterial Hypertension
Belma SARIC ZOLJ MD MD1,2*, Kristina GALIC MD, PhD1,2, TanjaZOVKO MD1,2, Suzana KUKULJ MD, PhD3, Gordana PAVLISA MD, PhD3, Marina VASILJ MD1,ValentinaLASIC MD 2,4, Ivan LASIC,Mag.Phys5
1. Department of Department of Pulmonary Diseases and TB, University Clinical Hospital Mostar,88 000 Mostar,Bosnia and Herzegovina
2. Faculty of Medicine, University of Mostar, 88 000 Mostar, Bosnia and Herzegovina
3. University Clinic of Pulmonary Disease Zagreb,10000Zagreb, Croatia
4. Clinic for Surgery, University Clinical Hospital Mostar, 88 000 Mostar,Bosnia and Herzegovina
5. Medical physics and radiation protection office, University Clinical Hospital Mostar, 88 000 Mostar, Bosnia and Herzegovina
Correspondence to: Saric Zolj Belma, MD, Department of Internal Diseases, University of Mostar School of Medicine. Department of Lung Diseases, University Clinical Hospital Mostar. Bosnia and Herzegovina.
Copyright
© 2024 Saric Zolj Belma, MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 July 2024
Published: 01 Aug 2024
Abstract
Objectives: The aim of this studywas to evaluate the HRQL in patients diagnosed with PAH using the36-item Short Form Health Survey questionnaire (SF-36).The second endpoint was to evaluate the impact of physical health, mental health, and religion on HRQL. Methods: Across-sectional, observational study included 40 patientswith a definite diagnosis of (PAH). Inclusion criteria were: completed a research questionnaire consisting ofSF-36, Santa Clara Religious Strength Questionnaire (SCSORF), and Duke University Religion Index Questionnaire(DUREL). Results: Mental health was correlated withthe HQRL(p=0.017).The 6-minute walk distance(6MWD)was significantly correlated with mental health (p=0.034).SF-36physical and SF-36 mental health(correlation coefficient 0,755, p<0.05),and there were statistically significant correlations (correlation coefficient=0.548, p <0.01) between religion and quality of life. Conclusion: HRQoL was impaired in PAH patients, particularly in those with increased disease severity. The findings of this studyimplythe need for a multidisciplinary approach to improve the quality of life of PAH patients and evaluate new and specific treatments.
Keywords: pulmonary arterial hypertension, health-related quality of life, Short Form SF-36 questionnaire, The Duke University Religion Index Questionnaire, Santa Clara Strength of Religious Faith Questionnaire.
Health-Related Quality of Life in Patients with Pulmonary Arterial Hypertension
Abbreviations
PAH,pulmonary arterial hypertension
HRQL, health-related quality of life
6MWT, 6-minute walking test
6MWD, 6-minute walking distance
SF-36, 36-Item Short Form Health Survey questionnaire
DUREL, Duke University Religion Index Questionnaire
SCSORF, Santa Clara Strength of Religious Faith Questionnaire
CES-D scale, Center for Depression Epidemiological Research
NYHA classification, New York Heart Association (NYHA) Classification
WHO-FC, World Health Organization functional class
1. Introduction
Despite targeted therapies,pulmonary arterial hypertension (PAH) is associated with significant morbidity and mortality (9).Available studies demonstrate that, despite the longer survival of patients with PAH, their quality of life (QoL) deteriorates as the condition progresses. Consequently, the goals of PAH therapy have expanded from increasing survival to improving health-related quality of life (HRQL) (10). PAH causes significant physical, social, work, and emotional burdens among affected patients and their caregivers (11).The primary objective of most trials was exercise capacity, whereHRQL was included in only a few studiesas well as a secondary endpoint (12-14). Some studies have shown that HRQL is increasingly important for evaluating new and specific treatment effects (13, 15). Few studies have investigated the HRQL in patients with PAH (16, 17). Compared tohealthy individuals, patients with PAH have reduced physical mobility, lower energy levels, increased pain, and greater social isolation(18). In Finland, for the first time, a study was conducted on the quality of life of 62 patients with PAH, and it was proven that quality of life was reduced for all examined parameters, except for the impact on mental health. Good results on the6-minute walking test (6MWT) were associated with a better quality of life. To our knowledge,there are no studies onthe impact of religion on HQRL in patients with PAH. However, some studies have shown thatpatient satisfaction with treatmentis significantly associated with spiritual and religious well-being (20). It is possible that religion is used more by sick people than by healthy people (21).Therefore, the 6MWT has limited utility as a serial measure for assessing changes in the clinical status of patients with severe heart failure(22).Although several randomized studies on PAH have assessed patients' quality of life parameters, it is not known which variables (disease severity, therapeutic algorithm, socioeconomic status,and psychological statushave the strongest impact on quality of life and how they relate(18).We designed our cross-sectional, observational studyto evaluate the HRQL in patients diagnosed with PAH using theSF-36.An additional goal was to evaluate the impact of physical health, mental health, and religion on HRQL.
2. Methods
2. 1. Study design
Thecross-sectional, observational study was conducted at two clinical Centers of the Department of Pulmonary Diseases of the University Clinical Hospital Mostar. Subjects diagnosed with PAH, aged 18-80 years, wereclassified according to the ESC 2019 guidelines for the type of PAH and the New York Heart Association (NYHA)classification. Involvement in the study was voluntary after the respondents received all explanations and were willing to participate. After the physician’s examination, the respondents completed a questionnaire consisting ofSF-36, SCSORF, and DUREL.
HRQoL,SCSORF,and DUREL data were collected using self-administered questionnaires during scheduled clinical visits. Patients were excluded if they were unable to complete the study questionnaires because of illiteracy or cognitive impairment or if they did not agree to participate in the study. The questionnaire was administered in the native language of the patient (Croatian language).
2. 2. Data collection
6MWT
A 6 MWT that measures the distance a patient can walk on a flat, hard surface for 6 minutes was performed. This test evaluates the globally integrated responses of all the systems involved during walking, including cardiopulmonary function, systemic and peripheral circulation, neuromuscular function, and muscle metabolism. The 6 MWT assesses submaximal and functional ability levels. The 6 MWTaccurately reflects the level of daily physical activity and shows an excellent correlation with maximum oxygen consumption (VO2 max). Oxygen saturation was measured at the beginning and end of the six-minute test, and the patient’s oxygen therapy was recorded during the test (23, 24).
NYHA Classification
I-IV: NYHA I: Heart disease without physical limitation;daily activity does not cause inappropriate fatigue, arrhythmia, shortness of breath, or angina pectoris. NYHA II: Heart failure with limited physical capacity. There were no problems at rest, and the daily load caused fatigue, arrhythmia, shortness of breath, or angina pectoris. NYHA III: Heart failure with a higher degree of physical capacity limitation. There were no problems at rest and little effort caused fatigue, arrhythmias, shortness of breath, or angina pectoris. NYHA IV: Difficulties at rest (24).
SF-36 questionnaire
SF-36 is a multi-applicable health status questionnaire with 36 questions. These are multiple-choice questions from 3 to 6, and the results are expressed in eight dimensions that make up the profile of health status:-1. Physical functioning (PF): -10questions; 2. Limitations due to physical difficulties (RP):4 questions 3 body pain (BP):-2 questions 4. Perception of general health (GH):-5 questions; 5. Vitality and energy (VT):-4 questions; 6. Social functioning (SF):-2 questions,-7. Role limitation due to emotional problems (RE):-3 questions; 8. Mental health (MH):-5 questions.The Physical Component Summary Measure (PCS) profile includes the following four dimensions from the aforementioned eight dimensions: physical functioning, limitations due to physical difficulties, physical pain, and general health perceptions. The mental component summary (MCS) profile includes vitality and energy, social functioning, limitations due to emotional difficulties, and mental health. The SF-36 represents a theoretically grounded and empirically verified operationalization of two general concepts of physical and mental health and their two general manifestations: functioning and well-being (24).
SCSORFquestionnaire
Religiosity will be measured by the SCSORF, which consists of ten statements, scored on a Likert-type scale from 1 to 4.
1–I do not agree entirely; 2–I disagree to a significant extent; 3-agree to a significant extent and 4-agree in full (Plante et al 1997) (25).
DURELquestionnaire
DUREL (Koenig et al. 1998), a self-assessment questionnaire of religiosity, consists of five particles with answers on a Likert scale ranging from 1 to 5. Extrinsic religiosity and intrinsic religiosity were also measured (26).
2. 3. Statistical Analysis
SPSS for Windows (version 13.0, SPSS Inc., Chicago, Illinois, USA) and Microsoft Excell (version 11 Microsoft Corporation, Redmond, Washington, USA) were used for statistical analysis.Nominal variables (e.g., sex) will be analyzed in the study using the χ2 test, and in the absence of the expected frequency, Fisher's exact test will be used. For continuous variables (e.g., age and lactate, oxygen, and carbon dioxide concentrations), the symmetry of their distribution was first analyzed using the Kolmogorov-Smirnov test. If the distribution of continuous variables was symmetric, the arithmetic mean and standard deviation were used to display the mean and scatter measures, and parametric tests (Student's t-test, ANOVA variance) were used to compare these variables. In the asymmetric distribution of continuous variables, the median and interquartile range were used to show the mean and scattering measures, and nonparametric tests (Mann-Whitney U test and, Kruskal-Wallis test) were used to compare them.
3. Results
Forty patients agreed to participate in the study and completed the questionnaire correctly (n = 40). Patients were divided into age groups: 18-35 years 5%(2), 36-49 years 25% (10), 50-64 years 32,5% (13); >65 years, 37.5% (15). There were 50%females(20), male 50% (20).The mean disease duration was 54 Â ±42 months.Most patients were in the World Health Organization functional class(WHO FC) I or II (55%). WHO FC III and I WHO FC I and II (45%) (Table 1).
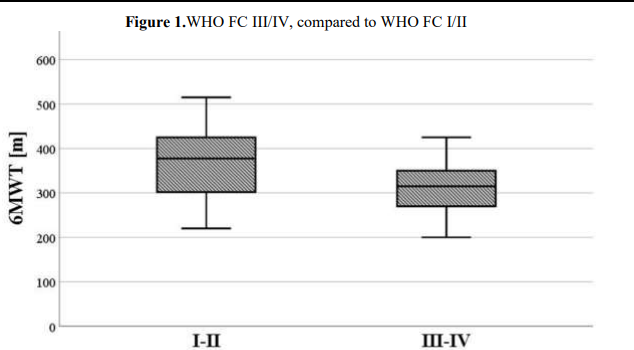
The mean 6MWD was 375.5 ± 78.8 meters in the overall population, but it was significantly reduced in patients in WHO FC III/IV 315 mcompared to groups I/II 375.1 meters (p < 0.05) (Figure1).
The arterial oxygen basal desaturationwas (96.0 ± 7.1)to desaturation during the 6 MWT (89 ± 12.3) mmHg. The mean right ventricular systolic pressure(RVSP) was 58.5±16.1 mmHg. Most of the patients (52.5%) were under PH-specific therapy, calcium channel blockers (22.5%), and supportive therapy (25.0%)(Table 1).
Specific therapies were administered orally,substantial number of patients were under oxygen therapy (40.1%) (Table1).
Importantly, the mean scores were significantly worse in patients with WHO FC III/IVthanin those with WHO FC I/II.
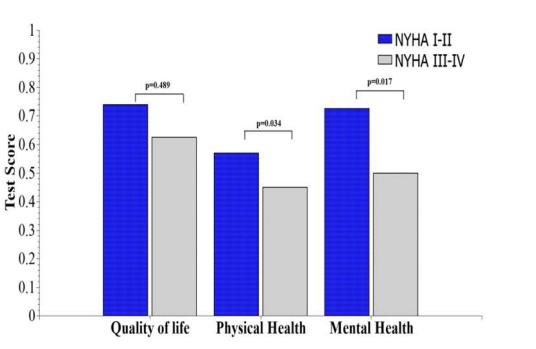
In SF-36 patients, physical health was correlated with HQRL, but thecorrelation was not significant (correlation coefficient 0,113, p=0.489). This is in accordance with the finding that patients’ physical health did not correlate significantly with the 6 MWD results. Mental health was significantly correlated with HQRL (correlation coefficient -0,375, p=0.017).
6MWT significantly correlates with mental health (One-way ANOVA f 2.654)(p=0.034).
The SF-36 physical andSF-36 mental healthscores were significantly correlated (correlation coefficient 0,755, p<0.05)(Figure 2).
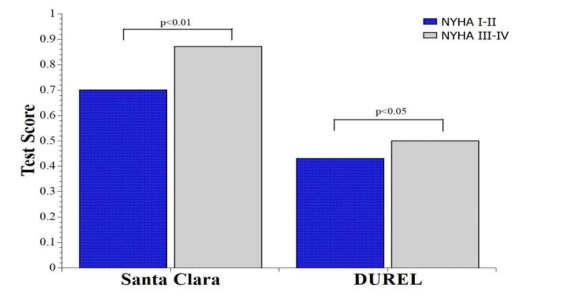
There was a statistically significant negative correlation between religion and QoL, such that patients with a worse quality oflife had more religiosity (correlation coefficient -0.548, p <0.01)(Figure 3).
There was a statistically significant correlation between the 6 MWT and patients’ sense of physical fitness(correlation coefficient, 0.512; p <0.05).
For the correlation of both tests of religion, we examined the connection with Spermar r and concluded that there were statistically significant correlations (correlation coefficient -0.848, p <0.01).
Table 1. Demographic and clinical characteristics of the study population.
|
Characteristic |
PH patients |
||||
|
(n=40) |
|||||
|
Age, years, % (n) |
|
||||
|
|
18-35 |
|
|
|
5 (2) |
|
|
36-49 |
|
|
|
25 (10) |
|
|
50-64 |
|
|
|
32.5 (13) |
|
|
65+ |
|
|
|
37.5 (15) |
|
Gender, % (n) |
|||||
|
Female |
50 (20) |
||||
|
Male |
50 (20) |
||||
|
Marital status, % (n) |
|||||
|
Single |
15 (6) |
||||
|
Married/Divorced/Widowed |
75 (34) |
||||
|
Working status, % (n) |
|||||
|
Full-time |
37.5 (15) |
||||
|
Unemployment |
7.5 (3) |
||||
|
Retired |
52.5 (21) |
||||
|
Disease duration, months |
54 ± 42 |
||||
|
|
|||||
|
WHO Functional class, % (n) |
|||||
|
I/II |
55 (22) |
||||
|
III/IV |
45 (18) |
||||
|
6MWD, meters |
375.5 ± 78.8 |
||||
|
02Sat_Bas,mmHg |
96 ± 7.1 |
||||
|
02Sat_Min,mmHg |
89 ± 12.3 |
||||
|
RVSP, mmHg |
58.5 ± 16.1 |
||||
|
PH specific therapy, % (n) |
52.5 (21) |
||||
|
Calcium channel blockers, % (n) |
17.5 (7) |
||||
|
PH supportive therapy, % (n) |
17.5 (7) |
||||
|
|
|
||||
Figure 1.WHO FC III/IV, compared to WHO FC I/II
Legend: NYHA -New York Heart Association,6MTW-The six minute walking test
Figure 2.Correlation physical, mental health and quality of life with NYHA patients status
Legend NYHA -New York Heart Association
Figure3. Correlation beetwen religion test and NYHA patients status
Legend: NYHA -New York Heart Association; Santa Clara - Questionnaire on the strength of religious faith, DUREL- Duke University Religion Index;
4. Discussion
In thiscross-sectional study, we examined the HQRL as the primary point in patients with PAH. According to available data, there is very little research worldwide on the quality of life of patients with PAH. This study investigated the impact of the clinical characteristicsof PAH with physical, socioeconomic, and subjective mental status on HQRL.In addition,the impact of spirituality on HRQL was determined using Durrel,SCSORF,and previous studies have shown that the HRQL of patients with PAH has a significant effect in comparison to healthy individuals (13). This study monitored the individual and overall impact of these variants on the quality of life of the respondents.The mean 6MWD was 375.5 ± 78.8 meters in the overall population, but it was significantly reduced in patients in WHO FC III/IV (320.3 ± 99.4 meters) compared to that in groups I/II (469.1 ± 75.4 meters).The 6 MWT score was significantly correlated withthe physical functioning dimensions (energy level and physical mobility)and HRQoL impairment in our cohort. The results are in line with the researchRais et al WHO FC, 6MWT, index was highly correlated with HRQoL impairment in PAH patients.These findings largely agree with previous evidence thatfound these two measures to be the most relevant predictors of HRQoL in PAH (27, 25, 26).
The WHO FC and 6MWT remained the most important correlates for the physical functioning dimensions (energy level and physical mobility)but had a substantially lower predictive value,which is in accordance with our findingthat physicalhealth hasan impact on HQRL, but not significantly.
We found that mental health significantly impactedHQRL(correlation coefficient -0,375, p=0.017). When we analyzed other predictors, measures of mental health status could have been important for inclusion in these models since other studies have also identified mental conditions to be correlated with HRQoL in PAH (23, 24).
In our study, we demonstrated an association between the SF-36 and the mental health of respondents.Adequate provision of psychosocial support requires careful monitoring by professional organizations.In its recent guidelines, a joint working group of ESC and the European Respiratory Society (ERS) has issued an International Committeerecommendation for patients to receive psychosocial support, reflecting the importance of this approach in improving HRQoL.The ESC/ERS guidelines state that multidisciplinary teams should be involved in providing psychosocial support to effectively manage the psychological, social, financial, emotional, and spiritual needs of patients (3).
We analyzed the impact of spirituality on the HqRQL and found a strong correlation. As HRQoL evaluates the effects ofphysical, mental, and social aspects, theeffects of illness on individual and other patient characteristics,such as spirituality,affectat patient’s sense of well-being. Recent studieson HRQLin PAH patients did not includethe impact of spirituality on HQRL.Health care providers recognize spiritualityas having a significant influence on an individual's ability to cooperate, while others have indicated that those who are spiritual tend to have a more positive outlook and better quality of life (28, 29).
We used both a general and disease-specific instrument to provide a more comprehensive picture of overall patient status, and other instruments (especially general instruments) could have been selected.To address this evidence gap, a recent study examined the prevalence of psychological symptoms and their association with HRQoL in patients with PAH. The researchers noted that mental status, functional class, and disabilityhad major effects on the observed variance in HRQoL in the study population.
The limitations of this study are the relatively small sample size and the small number of patients withsevere disease.This was a self-reported questionnaire. For more consistent results it is necessary to study a larger population and to carry out a long-term, prospective follow-up, which will serve to strengthen our results.
In conclusion, HRQoL was impaired in patients with PAH, particularly in those with increased disease severity.The new knowledge and findings gained in this study will provide a better understanding of the impact of the examined parameters on the quality of life of patients with PAH.
5. Conclusion
The results of this research should be useful in the development of a model that includes, in addition to the evaluation of the underlying disease, the overall socioeconomic and psychological status of patients with pulmonary hypertension in determining the overall quality of life.These results imply the need for a multidisciplinary approach to improve the quality of life of PAH patients.
Funding: Our research received no specific grants from any funding agency in the public, commercial, or not-for-profit sector.
Institutional Review Board Statement: The study was approved by the Ethics Committee of the University clinical hospital where the study was conducted and under the ethical standards of the Helsinki Declaration of 1975, as revised in 2000.
Data Availability Statement: Data is available on request from the authors.
Acknowledgments: none.
Conflict of interest: Authors declare that they have no conflicts of interest.
References
1. Norris S. H. Lan, Benjamin D. Massam, Sandeep S. Kulkarni, Chim C. Lang. Pulmonary Arterial Hypertension: Pathophysiology and Treatment. Diseases 2018, 6, 38.
2. K Sarzy?ska, N ?wi?toniowska-Lonc, K Dudek, K Jonas, G Kope?, J Gajek, B Jankowska-Pola?ska. Quality of life of patients with pulmonary arterial hypertension: a meta-analysis. Eur Rev Med Pharmacol Sci. 2021 Aug;25:4983-4998.
3. Deborah Jo Levine. Pulmonary arterial hypertension: updates in epidemiology and evaluation of patients. Am J Manag Care. 21 Mar;27:S35-S41.
4. H. Chen, D.B. Taichman, R.L. Doyle. Health-related quality of life and patient-reported outcomes in pulmonary arterial hypertension. Proc Am Thorac Soc, 5 (2008), pp. 623-630
5. M.M. Hoeper, R.J. Oudiz, A. Peacock, V.F. Tapson, S.G. Haworth, A.E. Frost, et al. End points and clinical trial designs in pulmonary arterial hypertension: clinical and regulatory perspectives. J Am Coll Cardiol, 43 (2004), pp. 48S-55S.
6. R. Condliffe, D.G. Kiely, J.S. Gibbs, P.A. Corris, A.J. Peacock, D.P. Jenkins, et al. Improved outcomes in medically and surgically treated chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med, 177 (2008), pp. 1122-1127.
7. J. Pepke-Zaba, C. Gilbert, L. Collings, M.C. Brown. Sildenafil improves health-related quality of life in patients with pulmonary arterial hypertension. Chest, 133 (2008), pp. 183-189.
8. S.P. McKenna, N. Doughty, D.M. Meads, L.C. Doward, J. Pepke-Zaba. The Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR): a measure of health-related quality of life and quality of life for patients with pulmonary hypertension. Qual Life Res, 15 (2006), pp. 103-115.
9. S. Shafazand, M.K. Goldstein, R.L. Doyle, M.A. Hlatky, M.K. Gould. Health-related quality of life in patients with pulmonary arterial hypertension. Chest, 126 (2004), pp. 1452-1459.
10. Kukkonen M, Puhakka A, Halme M. Quality of life among pulmonary hypertension patients in Finland. Eur Clin Respir J. 2016; 3: 10.3402.
11. Marques LFA. A saúde e o bem-estar espiritual em adultosporto-alegrenses [tese]. Porto Alegre: Faculdade de Psicologia, Pontifícia Universidade Católica do Rio Grande do Sul; 2000.
12. Powell LH, Shahabi L, Thoresen CE. Religion and spirituality: linkages to physical health. Am Psychol. 2003;58(1):36-52.
13. Oudiz RJ, Barst RJ, Hansen JE, et al. Cardiopulmonary exercise testing and six-minute walk correlationsin pulmonary arterial hypertension. Am J Cardiol.2006;97(1):123-6.
14. Cheetham C.Taylor R.Burke V.O'Driscoll G.Green D.The 6-minute walk test does not reliably detect changes in functional capacity of patients awaiting cardiac transplantation.J Heart Lung Transplant. 2005; 24: 848-853.
15. Remme WJ, Swedberg K Task Force for the Diagnosis and Treatment of Chronic Heart Failure, European Society of Cardiology. Guidelines for the diagnosis and treatment of chronic heart failure. Eur Heart J 2001; 22: 1527-60.
16. Ware jr JE. SF-36® Health Survey Update. 2009, SF-36.org: Lincoln, RI. http://www.sf-36.org.
17. Elliott D, Lazarus R, Leeder SR. Health outcomes of pati¬ents undergoing cardiac surgery: repeated measures using Short Form-36 and 15 dimensions of quality of life questionnaire. Heart Lung 2006;35(4):245-51.
18. Cummings, J. P., Carson, C. S., Shrestha, S., Kunik, M. E., Armento, M. E., Stanley, M. A., &Amspoker, A. B. Santa Clara Strength of Religious Faith (2015).
19. Pietra GG, Capron F, Stewart S, et al. Pathologic assessment of vasculopathies in pulmonary hypertension. J Am CollCardiol. 2004;43(12 Suppl S):25S-32S.
20. Koenig HG, George LK, Peterson BL. Religiosity and Remission of Depression in Medically Ill Older Patients. Am J Psychiatry 1998; 155:536–542.
21. Ehman JW, Ott BB, Short TH, Ciampa RC, Hansen-Flaschen J. Do patients want physicians to inquire about their spiritual or religious beliefs if they become gravely ill? Arch Intern Med. 1999;159:1803–1806.