Adult Tracheoesophageal Fistula - A Rare Case Report
Adult Tracheoesophageal Fistula - A Rare Case Report
Eppa Vimalakar Reddy*,Sumesh S Raja,Raju Musham
*Correspondence to: Eppa Vimalakar Reddy, India.
Copyright.
© 2024 Eppa Vimalakar Reddy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 Aug 2024
Published: 01 Sep 2024
Abstract
Adult TEF has increased recently, despite congenital TEF being more common. Among acquired TEF 75% are iatrogenic out of which post-intubated cuff-related trauma (3%) is most common. Other benign causes are granulomatous mediastinal infections like tuberculosis in the past. In our case, neither the malignant nor the trauma is the cause. We also discuss the diagnostic and management challenges concerning TEFs. TEF leads to recurrent aspiration pneumonia and can be challenging to manage hence requiring a multidisciplinary approach. Non-surgical interventions have a very limited role and lead to recurrence in most of the cases. Early and definite surgical intervention is proposed once the diagnosis is confirmed. Hence, surgical excision of TEF is the most definitive form of management.
Adult Tracheoesophageal Fistula - A Rare Case Report
Introduction
A tracheo-oesophageal fistula is the pathological connection between the esophagus and trachea which are normally separate structures (1). Adult TEF has increased recently, despite congenital TEF being more common. TEF that is present in adulthood is usually due to malignancy or iatrogenic. Common non-malignant causes include foreign body ingestion, trauma, and iatrogenic injuries. Certain infectious agents such as tuberculosis, syphilis, histoplasmosis, Candida, and mycobacterium cause TEF.
Case Report
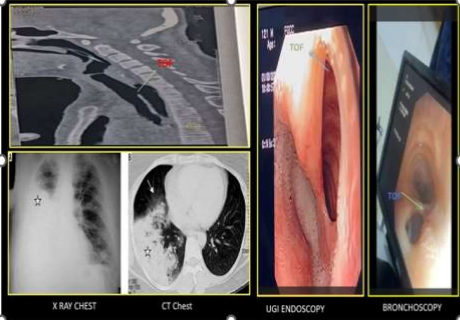
A 24-year-old lady who had recurrent upper respiratory tract infections for the past 6 months was treated by multiple physicians. Finally, the patient presented to a general surgeon who suspected TEF and advised CECT neck and chest revealed abnormal communication between the trachea and esophagus suggested TEF with diffuse patchy ground-glass opacities suggestive of aspiration pneumonia and right lung consolidation (Fig-1). They were referred to us for further management and presented to the emergency department with cough, breathlessness, tachypnoea, tachycardia, and hypoxia. The patient was resuscitated with IV fluids and oxygen. After Stabilization we planned surgery.
UGI-Endoscopy showed a large defect noted between the cervical esophagus and trachea located 23cm from the upper incisor. On Bronchoscopy communication between the trachea and esophagus was established. The patient was not associated with other congenital anomalies. The patient was intubated and the ET tip was located below the level of TEF but above the carina after confirming bilateral air entry. The patient was in a supine position with the neck extended and right lateral tilt. Laparoscopic feeding jejunostomy was done. Skin incision made along the anterior border of the sternocleidomastoid muscle. The Fistula tract was excised. The tracheal defect was closed by intermittent suture using 3-0 prolene and the esophageal defect was closed using 2-0 vicryl. The sternothyroid flap is placed between the trachea and esophagus (Fig-2,3,4). Biopsy from the fistula tract was suggestive of chronic inflammation and showed no evidence of active tuberculosis or malignancy.
On pod -2 patient was extubated and hemodynamically stable. On pod-11 patient was discharged with NG tube and Feeding jejunostomy.
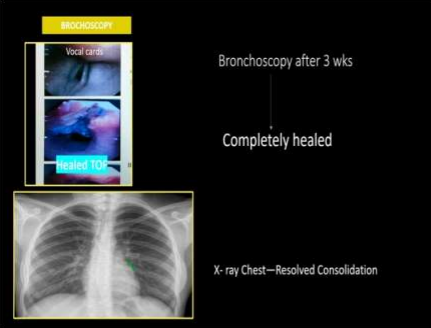
After 3 weeks, Bronchoscopy revealed a completely healed defect site of TEF, and chest x-ray revealed resolved consolidation. The patient is leading a normal life.(Fig-5)
Discussion
TEF is classified into two main categories: congenital and acquired contributing 50% each. Among acquired TEF 75% are iatrogenic. Most commonly post-intubated cuff-related trauma (3%). Other benign causes are granulomatous mediastinal infections like tuberculosis in the past (2). In our case, neither the malignant nor the trauma history was there. Hence the patient was treated by multiple physicians for the past 6months for upper respiratory tract infection. But at all in their 200-case series described cough (56%), aspiration (37%), fever (25%), dysphagia (19%), pneumonia (5%), hemoptysis (5%), and chest pain (5%) (3). Ono’s sign (worsening cough with swallowing solid/liquid) was present in 81% of the patients (4). A maximum of 30 days of delay in diagnosis was observed in benign TEF whereas in our case absence of an etiological factor might have delayed their presentation to the surgeon (5). CECT-Neck and Chest was the preferred non-invasive investigation in malignant as well as idiopathic cases like in our case.
But for the confirmation of location, size, and HPE, both UGI-Endoscopy and bronchoscopy are a must.
In our case, we confirmed the size, location, and benign featuristic of TEF with both scopy. Hence, we did not proceed to biopsy. Non-surgical management like fibrin glue injection, atrial closure device, endoscopic stenting, and repairs are described in a large number of series with benign etiology with reasonably good outcomes(6). In our case, in view of the large size of the defect around 3×3cm, and location which is just below the vocal cord (bronchial side) and just below the cricopharynx ( oesophageal side), which are non-amenable for stenting and opted for surgical management. Different types of surgical management described in the literature are excision of the fistula tract and include primary repair of an esophageal defect, esophageal repair with muscle flap, tracheal resection and anastomosis, tracheal defect repair with muscle flap(7). Like many cases of TEF, our case with elective intubation as well as the continuation of ventilation postoperatively with guarding stitch to avoid flap necrosis. Benign TEF usually has good outcomes with perioperative mortality is 0-2.8% and morbidity is 32-56%. In a large case series, all patients who underwent surgical intervention for benign TEF survived a median 41-month follow-up (6) . In our case, the patient was discharged on pod-11. The patient is leading a normal life.
Conclusion
The involvement of multidisciplinary teams remains important in the management of TEFs. Non-surgical interventions have a very limited role and lead to recurrence in most cases. Early and definite surgical intervention is proposed once the diagnosis is confirmed. Hence, surgical excision of TEF is the most definitive form of management for benign conditions.
Reference
1. Davydov M, Stilidi I, Bokhyan V, Arzykulov G. Surgical treatment of esophageal carcinoma complicated by fistulas. European Journal of Cardio-Thoracic Surgery. 2001 Aug;20(2):405–8.
2. Reed MF, Mathisen DJ. Tracheoesophageal fistula. Chest Surg Clin N Am. 2003 May;13(2):271–89.
3. Burt M, Diehl W, Martini N, Bains MS, Ginsberg RJ, McCormack PM, et al. Malignant esophagorespiratory fistula: Management options and survival. Ann Thorac Surg. 1991 Dec;52(6):1222–9.
4. Gerzi? Z, Raki? S, Randjelovi? T. Acquired benign esophagorespiratory fistula: Report of 16 consecutive cases. Ann Thorac Surg. 1990 Nov;50(5):724–7.
5. Diddee R, Shaw IH. Acquired tracheo-oesophageal fistula in adults. Continuing Education in Anaesthesia Critical Care & Pain. 2006 Jun;6(3):105–8.
6. Marulli G, Loizzi M, Cardillo G, Battistella L, De Palma A, Ialongo P, et al. Early and late outcome after surgical treatment of acquired non-malignant tracheo-oesophageal fistulae. European Journal of Cardio-Thoracic Surgery. 2013 Jun 1;43(6):e155–61.
7. Ke M, Wu X, Zeng J. The treatment strategy for tracheoesophageal fistula. J Thorac Dis. 2015 Dec;7(Suppl 4):S389-97.