The Effect of 17% Edta, 17% Edtac, 10% Citric Acid, and Horse Gram as an Effective Irrigant for Removing the Smear Layer Under the Sem: In Vitro Evaluation
The Effect of 17% Edta, 17% Edtac, 10% Citric Acid, and Horse Gram as an Effective Irrigant for Removing the Smear Layer Under the Sem: In Vitro Evaluation
Lingondo Simon Mwambo*
*Correspondence to: Lingondo Simon Mwambo, Cameroon.
Copyright.
© 2024 Lingondo Simon Mwambo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 Sep 2024
Published: 04 Oct 2024
Abstract
The study aimed to compare the effectiveness of Horse Gram as a final irrigant with 17% EDTA, 17% EDTAC, and 10% Citric Acid for smear layer removal under a scanning electron microscope. 75 extracted single-rooted anterior teeth were divided into five groups and irrigated with test irrigants. The samples were observed under a scanning electron microscope (SEM) and scored using a scoring system. Results showed that 17% EDTA provided the best results in smear layer removal in the coronal, middle, and apical third, followed by 17% EDTAC. 10% Citric Acid and Horse Gram showed similar results, especially in the middle third. Herbal medicines in endodontics are becoming more popular due to their safety and minimal side effects.
Key words: 17%EDTA, 17%EDTAC, 10%Citric Acid, Horse Gram, irrigants, smear layer
The Effect of 17% Edta, 17% Edtac, 10% Citric Acid, and Horse Gram as an Effective Irrigant for Removing the Smear Layer Under the Sem: In Vitro Evaluation
INTRODUCTION
Root canal therapy is a complex process that involves accurate diagnosis, appropriate instrumentation, irrigation, and three-dimensional obturation of the root canal system. The formation of a smear layer during endodontic instrumentation is crucial for achieving perfect sealing of the root canal system. Irrigation is one of the best methods to eliminate the smear layer from the root canal, allowing better penetration of irrigants into the dentinal tubules, better flow of cement sealer through empty spaces, and better adhesion between the obturating material and the dentinal wall.
Sodium hypochlorite (NaOCl) is the most widely used chemical solution in biomechanical preparation of the root canal system. However, it alone does not effectively remove the smear layer, so its association with chelating agents is necessary. The demineralizing effect of chelators acts indistinguishably on the smear layer and the root dentin, resulting in exposure of collagen and decrease of dentin microhardness. The greatest reduction in microhardness of the most superficial layer of dentin of the root canal lumen is desired.
The use of EDTA in endodontics was introduced by Nygaard-Ostby B (1957), which is recommended to remove the smear layer and organic tissue in the canal. EDTA solution acts only through direct contact with the substrate, so a surface modifier like Cetavlon or Cetrimide are required to reduce the surface tension of the liquid and improve the action of EDTA. This association is now known as EDTAC, a quaternary ammonium bromide used to reduce surface tension and increase irrigant penetration in dentinal tubules.
Citric Acid is another addition to the irrigation regime, equally efficient and more effective in removing the smear layer from the surface of the middle and coronal third of the root canal. High concentrations (25-50%) of Citric Acid are more effective than EDTA in removing calcium ions from dentine. However, 1% Citric Acid has a low pH, which may have an irritant effect on the periapical tissues.
Horse Gram (Dolichous Biflorus) beans are legumes of the tropics and subtropics grown mostly under dry land agriculture in several parts of South India. They are rich in iron, calcium, molybdenum, polyphenols, and have high antioxidant capacity. In recent years, the isolation and utilization of potential antioxidants from legumes including Horse Gram has achieved high attention as it decreases the risk of intestinal diseases, diabetes, coronary heart disease, and prevention of dental caries.
This study aims to compare the efficacy of Horse Gram in smear layer removal compared to other irrigants such as EDTA, EDTAC, and Citric Acid.
MATERIALS AND METHOD
This study involved 75 single rooted teeth that were extracted using a crown down technique. The teeth were removed from the root surface using hand scaling instruments, and then debrided with a soft brush. The teeth were then immersed in 3% sodium hypochlorite (NaOCl) for 30 minutes and mechanically debrided. Before the study, all teeth were decoronated at a fixed length of 14 mm from the anatomical apex using a diamond disc.
Canal instrumentation was performed using crown down technique using Protaper universal rotary system. Coronal preflaring was performed with Sx orifice shaper, and working length was determined by passing a #10 K-type endodontic file into the root canal until it was visible at the apical foramen. Root canals were prepared to the working length using S1, S2, and F1, F2 while irrigating with a 26 G open-ended beveled needle using 5ml of 3% sodium hypochlorite after each file. Recapitulation with smaller files was done during subsequent steps followed by final irrigation using 5ml of 3% sodium hypochlorite solution.
The solutions used for this study were freshly prepared in the Department of Chemistry at Punjab University, Chandigarh. These solutions included 17% EDTAC, 10% Citric Acid, Horse Gram seeds, and distilled water. The samples were randomly assigned to five groups based on their final rinsing, each containing fifteen samples.
The root canals were dried with paper points, and the coronal openings were blocked with cotton pellets to prevent foreign material entry. Sectioning of the teeth was done with a diamond disc, and the sections were split into three parts: cervical third, middle third, and apical third. These sections were dehydrated by dipping them into 50, 75, and 100% ethyl alcohol for 24 hours, and coated with a thin conductive metal film.
The specimens were ready for observation under a scanning electron microscope (SEM) and photomicrographs were obtained in x1000 magnification. Quantitative analysis was performed using Image-Pro Premier 9.1 software.
RESULTS
The study aimed to compare the efficacy of Horse Gram as a final irrigant with 17% EDTA, 17% EDTAC, and 10% Citric Acid for smear layer removal under a scanning electron microscope. Test specimens were divided into 5 groups of 15 each. The quantitative SEM evaluation was performed using computerized image analysis, with 24 squares divided into 6 parts each using CorelDRAW12. The percentage of open dentinal tubules was calculated using a formula: A = 76-100% of open dentinal tubules (completely-uniform), B = 51%-75% (moderately-uniform), C= 26%- 50% (mildly-uniform), and D= 0%- 25% (non-uniform).
Quantitative analysis was performed using Image-Pro Premier 9.1 software, and the open tubules/total dentinal ratio was calculated using the formula: Open dentinal tubules ×100
Results showed that Horse Gram was the most effective in removing smear layer, followed by Horse Gram and Distilled Water. The middle third showed the most effective treatment, followed by Horse Gram and Distilled Water. The apical third showed the least effective treatment, with Horse Gram showing the least effectiveness. The study concluded that Horse Gram is a suitable irrigant for removing smear layer removal.
DISCUSSION
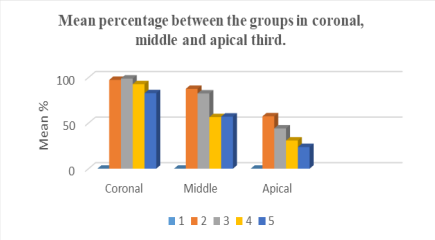
The study aimed to compare the efficacy of Horse Gram as a final irrigant with 17% EDTA, 17% EDTAC, and 10% Citric Acid for smear layer removal under scanning electron microscope. The results showed a down trend in open dentinal tubules from coronal third to apical third, which is consistent with previous work. The coronal and middle portions of the canal are wide enough for proper backflow of irrigants, resulting in better smear layer removal than the apical third.
The apical third of the root canal system is particularly difficult to clean due to the complexity of the root canal morphology, making irrigant delivery and activation less effective. Recapitulation with a K-file after flushing improved irrigant penetration. In Group 1, Distilled Water was completely ineffective (0%) in removing the smear layer from all three regions, as it showed a heavy smear layer throughout the entire length of the root canal. This finding supports previous findings by Paul ML (2013).
In Group 2, 17% EDTA as a final rinse was completely effective in removing the smear layer in coronal third (97.33%) and had good results in middle third (87.53%). It showed better results in apical third (57.4%) than other groups. In Group 3, 17% EDTAC as a final rinse was also completely effective in removing the smear layer in coronal third (98.8%), but less effective than 17% EDTA in middle (82.5%) and apical third (44.13%).
This finding supports previous work showing that reducing surface tension does not improve the effectiveness of EDTA. The lesser efficiency of EDTAC to remove calcium ions from dentin could be responsible for this finding. Recapitulation with a K-file after flushing improved irrigant penetration.
In a study, 10% Citric Acid was found to be effective in removing smear layer in the coronal third (92.7%), but less effective in the middle (56.5%) and apical third (30.9%). The study found that Citric Acid alone or a combination of concentrations of 10, 25, and 50% Citric Acid was more effective than NaOCl alone in removing the smear layer from the surface of the instrumented canal.
In the present study, the instrumented canals irrigated with 10% Citric Acid showed canal surfaces almost free of the smear layer. The middle third of the canal also exhibited a cleaner surface, possibly due to better volume and penetration of the acid in this region. Perez-Heredia M et al. (2006) found better results for the cervical and middle third compared to the apical one-third. Khedmat S and Shokouhinejad N (2011) found that these solutions were equally efficient and more effective in the cervical and middle thirds than in the apical third.
In Group 5, Horse Gram as a final rinse was also effective in removing smear layer in the coronal third (82.8%), but less effective in the middle (57.1%) and apical third (23.7%). It showed A value (76%-100%) in 11 samples and B value (51%-75%) in 4 samples in the coronal-third. In the middle-third, it showed B value (51%-75%) in 12 samples each and C value (26%-50%) in 3 samples.
In conclusion, 10% Citric Acid and Horse Gram were found to be effective in removing smear layer in the coronal and middle thirds, but less effective in the middle and apical thirds.
CONCLUSION
Herbal medicines are increasingly used in endodontics due to their safety and effectiveness, but misuse can be harmful. Proper delivery techniques and a combination of irrigants and sequential use are crucial for successful treatment. Efficient irrigation and agitation are essential for successful endodontic treatment, and proper delivery techniques can help achieve these prerequisites. This approach ensures successful root canal treatment.
Table 1 Substances used and the irrigation protocol
|
|
Group |
Irrigating solution during root canal preparation |
Final solution for removal of the smear layer |
|
1 |
Control |
3% NaOCl |
Distilled water |
|
2 |
2 |
3% NaOCl |
17% EDTA |
|
3 |
3 |
3% NaOCl |
17% EDTAC |
|
4 |
4 |
3% NaOCl |
10% Citric Acid |
|
5 |
5 |
3% NaOCl |
Horse Gram |
Figure 1
Reference
1. Abbott PV, Heithersay GS. A SEM study of the effects of different irrigation sequences and ultrasonics. Int Endod J 1991; 24: 308-316.
2. Abed AM, Farhad SZ, Farhad A, Barekatain M, Mafi M, Abooie MS. Debris and smear layer removal efficacy and changes in morphology of dentinal tubules after using citric acid, tetracycline?hydrochloride and mixture of tetracycline and acid and detergent. J Dent Res 2013; 10(2):232-237.
3. Atodariya U, Barad R, Upadhyay S, Upadhyay S. Anti-Urolithiatic Activity of Dolichos Biflorus Seeds. Journal of Pharmacognosy and Phytochemistry 2013; 2(2): 209-213.
4. Ballal NV, Kundabala M and Bhat KS. Evaluation of the efficacy of various concentrations of maleic acid and EDTA in removal of smear layer - An SEM study. IJCD 2011; 3(4): 225- 234.
5. Baumgartner J, Mader C. A scanning electron microscopic evaluation of four root canal irrigation regimes. J Endod 1987; 13:147–157.
6. Brannstrom M, Nyborg H. Cavity treatment with a microbicidal fluoride solution: growth of bacteria and effect on the pulp. J Pros Dent 1973; 30: 303–10.
7.Bronnec F, Bouillaguet S and Machtou P. Ex vivo assessment of irrigant penetration and renewal during the cleaning and shaping of root canals: a digital subtraction radiographic study. Int Endod J 2010; 43: 275–282.
8. Butterweck V, Khan S. Herbal Medicines in the Management of Urolithiasis: Alternative or Complementary? Planta Med 2009; 75: 1095–1103.
9. Bystrom A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J 1985; 18:35–40.
10. Callahan JR. Sulfuric acid for opening root-canals. Dental Cosmos 1894; 36: 957–959.
11. Cengiz T, Aktener BO and Piskin B. The effect of dentinal tubule orientation on the removal of smear layer by root canal irrigants. A scanning electron microscopic study. Int Endod J 1990; 23: 163-171.
12. Cergneux M, Ciucchi B, Dietschi JM, Holz J. The influence of the smear layer on the sealing ability of canal obturation. Int Endod J 1987; 20: 228–32.
13. Chailertvanitkul P, Saunders WP, MacKenzie D. The effect of smear layer on microbial coronal leakage of gutta-percha root fillings. Int Endod J 1996; 29: 242–8.
14. Chitme HR, Alok S, Jain SK, Sabharwal M. Herbal Treatment for Urinary Stones. International Journal of Pharmaceutical Sciences and Research 2010; 1(2): 24-31.
15. Ciucchi B, Khettabi M & Holz J. The effectiveness of different endodontic irrigation procedures on the removal of the smear layer: a scanning electron microscopic study. Int Endod J 1989; 22: 21-28.
16. Cruz-Filho AM, Sousa-Neto MD, Savioli RN, Silva RG, Vansan LP and Pecora JD. Effect of Chelating Solutions on the microhardness of Root Canal Lumen Dentin. J Endod 2011; 37 (3): 358- 362.
17. Dakshita J, Ashish A. Recent concepts on root canal chelation. ENDO 2011; 5(3):175–194.
18. Darda S, Madria K, Jamenis R, Heda A, Khanna A, Sardar L. An in-vitro evaluation of effect of EDTAC on root dentin with respect to time. J Int Oral Health 2014; 6(2):22-27.
19. Dechichi P, Moura CCG. Smear layer: a brief review of general concepts. Part II. The most common agents to remove endodontic smear layer. RFO UPF 2006; 11(2):100-104.
20. De-Deus G, Paciornik S, Mauricio MH. Evaluation of the effect of EDTA, EDTAC and citric acid on the microhardness of root dentine. Int Endod J 2006; 39: 401-7.
21. Mohgana, R., Samuel, A. J. S. J., Kalusalingam, A. & Bethala, K. Hepatoprotective Activity of Macrotyloma uniflorum (Lam.) Verdc. Seeds Extracts against Paracetamol Induced Hepatotoxicity in Wistar Albino Rats. British Journal of Pharmaceutical Research.2017,15(5), 1-9.
22. Saroj, K. P. & Manoj, K. S. Horse gram- an underutilized nutraceutical pulse crop: a review. J Food Sci Technol. 2015, 52(5), 2489–2499