Completion Left Pneumonectomy and Carinal Resection through One Stage Left Thoracotomy
Completion Left Pneumonectomy and Carinal Resection through One Stage Left Thoracotomy
Lukadi Joseph Lula1*, Andrei Daniel Dermengiu2, Vlad Teodor Silaghi1, Anca Oana Ghenu2, Lucian Dorobantu3 and Codin Theodor Saon1
1. Thoracic surgery unit, Nord Pipera Hospital, Bucharest, Romania.
2. Anesthesiology unit, Nord Pipera Hospital, Bucharest, Romania.
3. Cardiovascular surgery unit, Nord Pipera Hospital, Bucharest, Romania.
*Correspondence to: Lukadi Joseph Lula, Nord Pipera Hospital, Bucuresti, Romania
18, bulevardul Dimitrie Pompeiu 9-9A, Bucuresti, 020335.
ORCID:https://orcid.org/0000-0001-9745-0259
Copyright
© 2024 Lukadi Joseph Lula. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 Oct 2024
Published: 23 Oct 2024
Abstract:
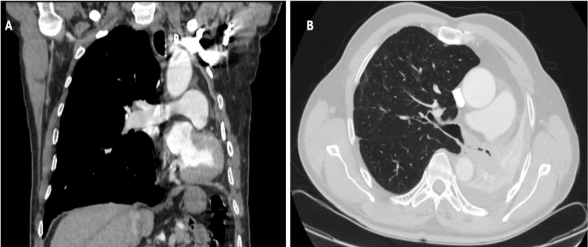
Left pneumonectomy with carinal resection is seldom performed through one stage left thoracotomy. We report a such intervention in a redux background. A 64-year-old gentleman had history of open left upper lobectomy with adjuvant chemotherapy for a squamous carcinoma six years ago. He experienced a pathologically proven recurrence in the remaining lower lob with invasion extending up to the carina. Chest CT revealed a substantial mediastinal left shift with a complete atelectasis of the remaining left lung lower lobe. A completion left pneumonectomy with carinal resection and lymph nodes dissection were exclusively performed through a left postero-lateral thoracotomy, in summer 2024. He experienced atrial fibrillation on the 2nd postoperative day and had a week length of hospital stay. Despite the redux, one stage left thoracotomy approach allowed a radical pathologically proven resection of the specimen with an acceptable early outcome.
Completion Left Pneumonectomy and Carinal Resection through One Stage Left Thoracotomy
Introduction
This was not a straightforward decision. At the multidisciplinary team discussion, upfront surgical option prevailed because of the complete main left bronchial obstruction and pulmonary arterial-venous shunt induced by the complete lower left lung atelectasis, in a patient with no surgical contraindication.
Case Presentation
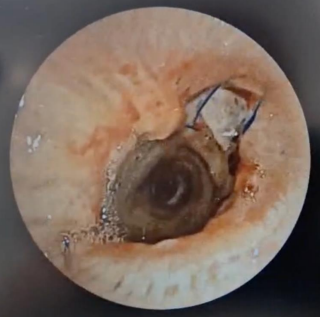
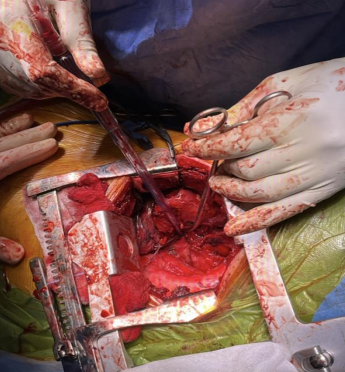
A 64-year-old gentleman underwent an upper left lobectomy with radical lymphadenectomy by left lateral thoracotomy and had an adjuvant chemotherapy for a pT2bN0 squamous lung carcinoma in 2018. He was admitted in our department with a proven recurrence in the remaining lower left lung and invasion of the main bronchus up to the carina. Enhanced CT-Scan revealed a complete left lower lung atelectasis and left shifted mediastinum (Fig 1). An intrapericardial left completion pneumonectomy, carinal resection and anastomosis between the proximal trachea and the distal right main bronchus stump were performed only through a left posterolateral thoracotomy. Anesthetic management consisted in thoracic epidural analgesia, an internal jugular central venous line, and a radial arterial catheter. Anesthesia was induced using propofol, ketamine, fentanyl, and rocuronium. The patient was intubated with a 37 Fr left double-lumen endotracheal tube (ETT) and maintained on propofol TCI to avoid sevoflurane contamination in the operating room. Thoracotomy was performed away from the previous scar, entrance in the pleural cavity was carefully carried out, pericardium abutting at the chest wall, hilar structures were individualized within the pericardium, left pulmonary artery and the inferior pulmonary vein were stapled, the bronchial tree was meticulously dissected with a digital dissection of the distal tracheal and right tracheal tree and with simultaneous lymphadenectomy. Tracheal was sectioned one cartilage above the carina and the right main bronchus between the first and the second cartilage. The specimen was extracted, a cross-field tube 5.0 mm cuffed endotracheal tube was used to intubate in the right bronchial tree and running suture was performed between trachea and right main bronchus with 3.0 PDS. The patient was immediately extubated with less than 12 hours stay in intensive care unit. He underwent active physiotherapy, he had pain killers and preventive anticoagulation (Fig 2). He presented atrial fibrillation (on day 2) that was converted with medication. The control bronchoscopy performed on day 7 was satisfactory (Fig 3), he was discharged the same day. The definitive histopathology revealed a pT4N0M0 R0 squamous carcinoma.
Discussion
The carinal left pneumonectomy only performed through left thoracotomy was reported by Grillo (1), we did not find so far any other report except some related scenario where for instance carinal resection was performed through left thoracotomy addressing a left pneumonectomy complication, performed with extracorporeal membrane oxygenation (2). Most teams perform this operation in 2 approaches(3): a left pneumonectomy by left thoracotomy or thoracoscopy and carinal sleeve resection thought right thoracotomy. Some others perform a sternotomy, a clamshell with a difficult access to hilum and carina. One stage approach avoids the 2 sides scars with subsequent lower pain, a better postoperative mobilization and a mitigated risk of pulmonary infection (which is critical for a patient with a remaining single lung). Preforming this intervention in a redux context is more than convincing that it can done in an elective background. Authors believe that surgeons are reluctant to perform carinal left pneumonectomy through a left thoracotomy, because they worry to be impeded by the aortic arc, they also may think that the bronchial tree mobilization is impossible through the left. We advocate that for a tumor or invasion limited to the carina (with no tracheal invasion), aortic may be pulled cranial as it is done in case of left sleeve lobectomies (Fig 4.); related to the bronchial tree mobilization, we believe that a digital dissection is enough.
However, we should recognize the difficulty of cross-field ventilation, the right bronchus being not long enough, but close collaboration with anesthesiologist is essential for preventing significant hypoxemia. The positioning of the ETT should be controlled and adjusted by the surgical team while anesthesiologist monitors airway pressure and flow. This may also be easier using jet-ventilation.
Left pneumonectomy with carinal resection can be performed by one stage left thoracotomy even when it is about a completion pneumonectomy with none compromised outcome.
Funding statement
None
Conflict of interest statement
No author has any conflict of interest
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient.
References
1. Grillo H. Surgery of the Trachea and Bronchi. Hamilton: B.C. Decker, Inc., 2004;599–617. B.C. Decker, Inc. 2004. 559–617 p.
2. Lei J, Su K, Li XF, Zhou YA, Han Y, Huang LJ, et al. Ecmo-assisted carinal resection and reconstruction after left pneumonectomy. J Cardiothorac Surg. 2010 Dec;5(1):89.
3. Yen Y, Lai W. Right Thoracotomy for Carinal Resection With Left Thoracoscopic Pneumonectomy as a New Approach for Left Sleeve Pneumonectomy: A Case Report. Kaohsiung J Med Sci. 2010 Nov;26(11):609–14.