Ultrasonography in Orthopedic Opd Treatment of Carpal Tunnel Syndrome
Ultrasonography in Orthopedic Opd Treatment of Carpal Tunnel Syndrome
Dr Vinod Jogendra Shahoo*
*Correspondence to: Dr Vinod Jogendra Shahoo. (DNB, Orthopedics.)
Copyright
© 2024 Dr Vinod Jogendra Shahoo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 May 2024
Published: 03 June 2024
DOI: https://doi.org/10.5281/zenodo.11440219
Ultrasonography in Orthopedic Opd Treatment of Carpal Tunnel Syndrome
Introduction
Muskuloskeletal medicines is currently undergoing paradigm shift to alternative approaches along with the traditional care.
Conventional methods using anatomical bony landmarks for the injection based therapy is slowly being replaced by precision-guided injections at the POC( Point of care) with high defination Ultrasound and fluroscopy.
A standard of care should be established by adapting to ultrasound guided injections to joints, ligaments and tendons, perineural hydrodissection etc.
What is injected around these stuctures depends on the experti and preference of the injecting surgeon.
It ranges from simple 5% dextrose , steroids, PRP, ACRS, MICRO FAT, LA, OTHER ORTHOBIOLOGIS, GOLDIC, BERBOTAGE.
CARPAL TUNNEL SYNDROME-
Carpal tunnel syndrome (CTS) is the collection of symptoms and signs associated with nerve compression of the median nerve at the carpal tunnel.[6] Most CTS is related to idiopathic compression of the median nerve as it travels through the wrist at the carpal tunnel (IMNCT).[1] Idiopathic means that there is no other disease process contributing to pressure on the nerve. As with most structural issues, it occurs in both hands, and the strongest risk factor is genetics.[1]
Other conditions can cause CTS such as wrist fracture or rheumatoid arthritis. After fracture, swelling, bleeding, and deformity compress the median nerve. With rheumatoid arthritis, the enlarged synovial lining of the tendons causes compression.
The main symptoms are numbness and tingling in the thumb, index finger, middle finger and the thumb side of the ring finger.[1] People often report pain, but pain without tingling is not characteristic of IMNCT. Rather, the numbness can be so intense that it is described as painful.
Symptoms are typically most troublesome at night.[2] Many people sleep with their wrists bent, and the ensuing symptoms may lead to awakening.[7] Untreated, and over years to decades, IMNCT causes loss of sensibility and weakness and shrinkage (atrophy) of the muscles at the base of the thumb.
Work-related factors such as vibration, wrist extension or flexion, hand force, and repetition are proposed risk factors for IMNCT. But to date, there is mostly evidence of association with symptoms (CTS), not neuropathy (IMNCT), which is an important distinction. The only certain risk factor for IMNCT is genetics. All other risk factors are open to debate. It is important to consider IMNCT separately from CTS in diseases such as rheumatoid arthritis.[8][5][3]
Diagnosis of IMNCT can be made with a high probability based on characteristic symptoms and signs. IMNCT can be measured with electrodiagnostic tests.[9]
Signs and Symptoms
The most common symptoms of carpal tunnel syndrome include:
- -> Numbness or pins/needle sensations in the palm of the hand, including the thumb, index and middle fingers
- - Especially at night and in the morning
- - Made worse with pressure on the wrist or wrist bending
- -> Weakness of the muscles in the hands and fingers
- -> Decreased grip strength
Carpal Tunnel Injection (i.e., Median Nerve Hydrodissection)
Pertinent Anatomy
• The carpal tunnel is bounded by the scaphoid and pisiform proximally and tubercle of the trapezium and hook of the hamate distally. The TCL overlies the tunnel.
• Contents of the tunnel include the median nerve, flexor pollicis longus, and the tendons of the flexor digitorum superficialis and profundus (Fig.).
Common Pathology
• Compression of the median nerve can be related to thickening of the TCL, ganglion cysts, tenosynovitis, amyloidosis, joint effusions/synovitis, aneurysms, lipomatous hamartomas, and accessory muscles.
• It is the most common site of nerve compression in the upper extremity, with an incidence of 3.5% and 6.2%.
• There are many anatomic variants of the median nerve that need to be taken into consideration when doing injections about the carpal tunnel. The most common anatomic variant is that of a persistent median artery with a bifid median nerve.
• There are also anatomic variants of the thenar motor branch, which should be identified prior to procedures about the median nerve.
• Equipment
• 30 to 25-gauge needle, 1 and 2 inch
• High-frequency linear array ultrasound transducer
Common Injectates
• Local anesthetics, corticosteroids
• Neuroprolotherapy (5% dextrose)
• Orthobiologics (PRP, platelet lysate)
Injectate Volume
• 1 to 5 cc
Technique
Patient Position
• Seated with the elbow flexed and the wrist supinated, with fingers relaxed.
• An alternate position is lateral recumbent or supine with the arm at the side, on the arm board.
Clinician Position
• Seated or standing facing the patient’s wrist and monitor.
FIG 1. Median Nerve Hydrodissection(HD) at The Wrist Under Ultrasound Guidance.
Transducer Orientation
• The transducer is placed in the anatomic axial plane, short axis to the median nerve, identifying the proximal and distal carpal tunnel and any anatomic variants that would prohibit a safe injection (Fig.).
Needle Orientation
• The needle is introduced via an in-plane, ulnar-to-radial approach.
• Alternatively, an out-of-plane, distal-proximal or proximal-to-distal approach can be used with the transducer in the same position (see Fig.).
Target
• Place the needle both superficial and deep to the median nerve at the level of the proximal carpal tunnel (see Fig. ). Anesthetic and sterile saline is used to create a halo around the nerve for the hydrodissection.
• With the alternative out-of-plane approach, the goal is to stay ulnar to the nerve.
HD Methods
There are two primary methods of US-guided HD of peripheral nerves.10
Literature review revealed no indepth comparison of the performance of these techniques with respect to the learning curve, effectiveness, and safety of each.
Method 1 (in-Plane Approach, Needle Perpendicular to the Long Axis of the Nerve) -
Generally, when using method 1 for HD of nerves, the needle and probe are both perpendicular to the long axis of the nerve. The needle is in-plane to the transducer, and the tissues above and below the nerves are hydrodissected. The needle first approaches the inferior surface of the nerve with the needle bevel positioned up, and the pressure of the injectate is used to open the soft tissues around the nerve layer by layer until the injectate surrounds the epineurium. Since flexible hypodermic needles with bevels are typically used, it is safer to approach the inferior surface of the nerve bevel up as the resistance of the soft tissue will generally force the needle to go deep, and avoid damaging the inferior part of the nerve.28 The same process is repeated with the needle approaching from the superior surface of the nerve, with the needle bevel positioned down (Figure ). The hypodermic needle is bevel down so that the resistance of the soft tissue will force the needle to move more superficial and avoid injuring the superior part of the nerve. The hydrodissected nerve appears oval and surrounded by anechoic fluid on US when the release is completed. A 25-gauge 50 mm, or 22-gauge 70–100 needle is used, depending on the depth of the nerve, and keeping in mind the benefit from an enhanced needle echogenicity that results from reduction of the angle between the probe and the path of needle movement
Clinical Pearls Related to HD in General and Method 1 Specifically -
1. The basic principle of US-guided HD of peripheral nerves is that the fluid injectate, not the needle, is the tool used to separate the soft tissues. Therefore, after administering local anesthetics at the superficial entry point of the needle, it is essential to advance the needle slowly and visualize the needle at all times during the procedure, particularly during needle advancement, during which the physician will continually inject fluid. The injectate incrementally separates the soft tissues in front of the needle, followed by movement of the needle tip into the resultant fluid space.
2. Slow needle advancement while injecting also minimizes disruption of important soft tissues; e.g., vascular bundles and other nerves, running parallel to the target nerve to be hydrodissected. It also maximizes comfort through allowing more time for surrounding tissues to be gently pushed aside by a continuous fluid jet. This facilitates performance of hydrodissection without a lidocaine component.
3. In addition to observing the bevel position, continuous needle tip observation, continuous injection before and during needle movement, and slow needle advancement, safety is further enhanced by encouraging a verbal commentary from the patient during which they describe what sensations they experience during the procedure. It is best to advise patients that, when the nerve is hydrodissected from the surrounding soft tissues, they will commonly experience aching, numbness, a burning sensation, or cramping in the distribution of the nerve, particularly at the moment of fascial release, and rarely an electrical sensation if the epineurium is lightly contacted or when scar tissue is peeled off the epineurium.
4. Method 1 requires less injectate volume to separate the nerve from the surrounding soft tissues. If the nerve is tethered significantly to the soft tissue; e.g., scar tissue, method 1 can be used to safely detach the nerve from the scar tissue.
Method 1 can be learned rapidly, proportional to the amount of hands-on practice of needling technique, supplemented as feasible by cadaver workshops.
5. Bevel position may impact needle direction/tracking, especially if a long and thin needle is used (Figure). If the bevel of a needle is positioned on the side the needle will tend to bend to the opposite side, out of alignment with the target, and out of the narrow viewing plane of the ultrasound probe.
6. Usually, HD of the nerve is initiated from the site where the nerve is most severely damaged or trapped. If the diseased nerve or the damaged/ entrapped part of the nerve is long, the same entry point can be used, with the transducer and needle pivoted to the proximal portion of the nerve, and after that, to the distal part of the nerve to repeat the HD process (Figure ).
Method 2 (Out-of-Plane with Subsequent in-Plane Approach-
During the performance of method 2, the needle is parallel to the long axis of the nerve, and the probe is first perpendicular and then parallel to the long axis of the nerve. An “out-of plane” technique is used to HD the nerve from the surrounding tissues, confirming that the nerve is freed from the surrounding soft tissues by the visualization of anechoic fluid surrounding the nerve (both above and below the nerve). Subsequently, the probe is turned “in-plane” toward the nerve, the needle tip is guided back to the top of the nerve, and fluid is injected above it, with the bevel positioned down when approaching the nerve to avoid making accidental contact with the nerve. The injected fluid can accomplish this, but method 2 can separate a comparatively longer length of nerve from surrounding soft tissue through a single insertion point.
Method 2 for HD of nerves requires good “out-of -plane” and “in-plane” techniques, and often the ability to switch back and forth between the two. If the needle tip is not visualized, and the doctor keeps advancing the needle, impalement of the nerve may occur. The learning process for method 2 is usually much longer than method 1. Extensive practice of this technique in cadaver courses and a high comfort level with out-of plane visualization is recommended prior to attempting method 2. If not proficient in this technique, a doctor with good method 1 skill can perform in-plane HD perpendicular to the short axis of the nerve first, followed by HD of the nerve in-plane with the needle and transducer parallel to the long axis of the nerve through another needle entry point. Another alternative, using an in-plane technique through the same needle entry point, is to utilize several needle redirections as described under pearls for method 1. A third option is to simply use method 1 with different entry points to HD the nerve at several locations along the area of constriction.
Figure 2, Figure 3, Figure 4, Figure 5
TOTAL 4 ULTRASOUND GUIDED MEDIAL NERVE HYDRODISSECTION FOR CARPAL TUNNEL SYNDROME WERE DONE BETWEEN JULY 2023- JANUARY 2024.
Technique used – method 1
Linear probe, high frequency.
25 g needle 1.5” length
Syringe 5 and 10 ml
20-50 ml 5% dextrose
2% lidocaine
Dressing
STEPS-
NERVE IDENTIFICATION- I usually start from proximal to distal from the forearm identifying the nerve ( honey comb appearance) in the forearm and then trace it distally into the carpal tunnel in the wrist.
The nerve is easy to find proximally in the forearm due to absence of any tendons and clarity of the structure within the forearm MUSCLES.
A 360 degree dial needle placement and injectate injection is done to free the nerve from the adhesions all around as shown in the diagram and USG pictures.
Figure 6, Figure 7, Figure 8
Hypotheses for a Direct Ameliorative Effect of Dextrose on Neuropathic Pain
Neuropathic pain results from such minimal compression that it supports the concept that minimal nerve compression is capable of creating structural changes in nerves as well as neuropathic pain. Many conditions can increase the susceptibility of sensory nerves to compression. A direct mechanical benefit from nerve release may result from the restoration of nervi or vasa nervorum function though the release of pressure effects. Examination and ultrasound visualization are jointly helpful to identify pathologic nerves. In-plane technique (method 1) is recommended as the primary/safer approach with key features of using the injectate jet to dissect the soft tissue in front of the needle, and fully releasing fascia until the nerve appearance is rounded and the nerve is completely surrounded by injectate fluid. The injectate of preference may be D5W for most applications, based on preliminary literature findings evaluating comparative injectates, empirical and clinical evidence of a direct analgesic effect of dextrose separate from a hydrodissection mechanism, and the ability of D5W to be used for high volume and multiple-nerve applications. The mechanism of benefit of HD for benefit in neurogenic pain has not been established and will require substantial basic science research.
Several hypotheses have been proposed to explain the effect of dextrose solution on treating neuropathic pain such as:
Down regulation of the Transient Receptor Potential Vanilloid Receptor-1 (TRPV1) Ion Channel or Reduction of Its Downstream Mechanism of Action Up regulation (persistent opening) of the TRPV1 ion channel is strongly associated with the persistence of chronic neuropathic pain. The TRPV1 ion channel was previously called the capsaicin receptor because no other ion channels are affected by capsaicin. Capsaicin causes a characteristic burning sensation by upregulating the TRPV1 channel. Mannitol, a 6-carbon-atom sugar, has been found to reduce the burning sensation after exposure to capsaicin, suggesting an antagonistic (calming) effect on TRPV1 up regulation, either directly or by downstream effect. Dextrose, similar in structure to mannitol, has empirically been observed to have a similar effect, although it has not been formally tested using the capsaicin model developed by Bertrand et al.
Correction of Perineural/Intraneural Glycopenia Chronic neuropathic pain may signify glycopenia around the corresponding nerve(s). Injecting dextrose may promptly correct this glycopenia and consequently reduce neuropathic pain. Moreover, 40% of our peripheral somatosensory nervous system is comprised of small capsaicin-sensitive nerves (nerves with the TRPV1 ion channels on their surface), which are predominantly C fibers, and have an apparent homeostatic role in monitoring the level of systemic dextrose. Both the brain and peripheral nerves have a high and constant requirement for glucose. MacIver reported that when isolated C fibers are exposed in vitro to a hypoglycemic environment by substituting D-glucose with non-metabolizable L-glucose, they demonstrate a dramatic (653±23%) increase in discharge frequency within 5 minutes, maximized after 15 minutes. The C fiber firing rate returned to baseline within 2 minutes of replacement of D-glucose in the culture solution. MacIver explains these prompt changes in neural firing rates by reminding us of the central role of D-glucose metabolism in provision of ATP to power the cellular Na+ -K+ pump in animal and human cells. Hypoglycemia results in reduced activity of the ATP dependent Na+-K+ pump, resulting in a progressive nerve depolarization and hyperexcitability.
Potential Improvement of Nerve Mobility Through US Hydrodissection A cadaveric study done in Mayo clinic showed that HD can decrease the gliding resistance of the median nerve within the carpal tunnel, supporting the concept that HD may result in a beneficial mechanical change in nerve movement. However, the gliding resistance was measured immediately after hydrodissection and does not offer proof of a sustainable benefit. At this time that can be implied only indirectly by sustainable symptomatic benefit, and improvement of neural edema and nerve conduction parameters.
Safety of US-Guided HD of Nerves –
Whenever a doctor is injecting around the nerve, nerve injury is a potential complication. Jeng et al suggest that nerve damage is rare due to the polyfascicular architecture of the peripheral nerve and nerve fiber dispersal within the nerve. The importance of avoiding nerve contact cannot be overemphasized, and the advantages of hydrodissection without lidocaine may be considerable, in that it allows the clinician to hydrodissect continually and liberally ahead of the needle, without concern for anesthetic toxicity. Nevertheless, HD of nerves is not a technique for beginners in US-guided pain interventions, requiring relatively advanced skills in US-guided needling techniques. Cadaveric injection experience is crucial, and the authors stress repetitively that the injecting pressure should be the separating agent to release the soft tissues tethered to the nerves, not the needle itself.
Pearls and Pitfalls
• Color Doppler will help visualize the ulnar artery and ensure safe needle placement away from the vasculature.
• An ultrasound can be used for real-time visualization of injectate flow along the nerve by moving the transducer along the length of the nerve.
• A gel standoff is recommended during an in-plane approach to avoid the ulnar artery and nerve.
• Identification of at-risk structures and understanding of possible variant anatomy prior to injection is recommended.
References
1) Ultrasound-Guided Nerve Hydrodissection for Pain Management: Rationale, Methods, Current Literature, and Theoretical Mechanisms This article was published in the following Dove Press journal: Journal of Pain Research King Hei Stanley Lam, 1,2 Chen-Yu Hung, 3 Yi-Pin Chiang, 4,5 Kentaro Onishi,6 Daniel Chiung Jui Su,7 Thomas B Clark,8 K Dean Reeves 9
2) Bennett’s animal model of neuropathic pain .
3) Atlas of interventional orthopedic procedures (WILLIAMS. SUSSMAN, PITTS) ELSEVIER.
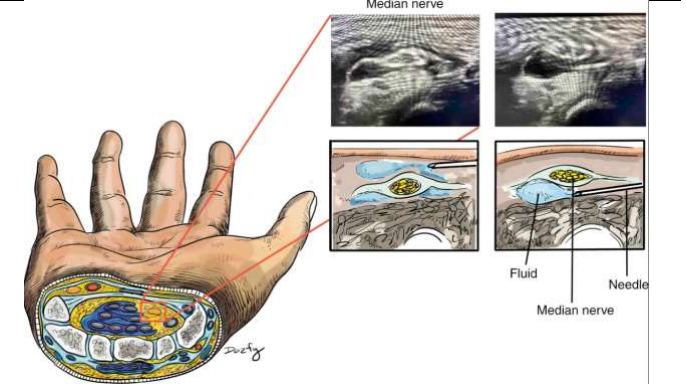
Figure 1
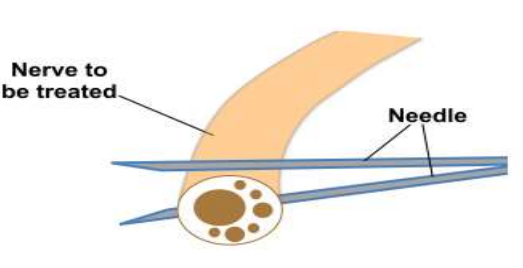
Figure 2
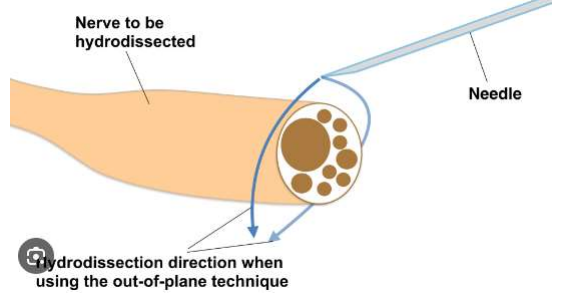
Figure 3
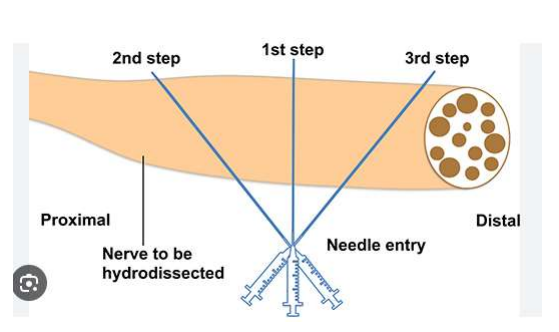
Figure 4
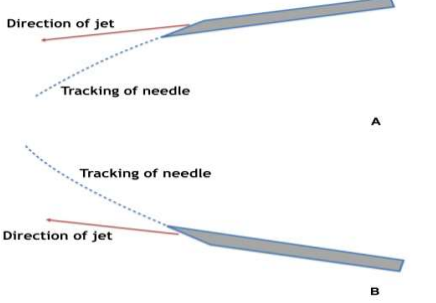
Figure 5

Figure 6
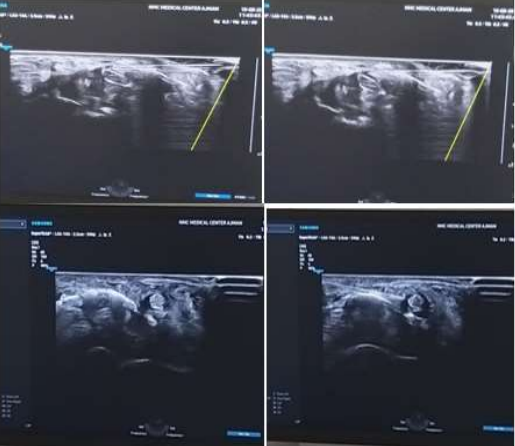
Figure 7

Figure 8