Scanning Electron Microscopic Study of Nuclear Cataract Lens
Scanning Electron Microscopic Study of Nuclear Cataract Lens
Dr. med. Dieter W. Klaas*
*Correspondence to: Dr. med. Dieter W. Klaas.
Copyright
© 2024 Dr. med. Dieter W. Klaas. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 September 2024
Published: 01 November 2024
Abstract:
Background and Purpose: The introduction highlights that cataracts are common in the elderly, leading to severe vision loss, particularly in the form of nuclear cataracts, characterized by a hard and dense nucleus. The document outlines the historical context of cataract surgery, which has evolved from extracapsular cataract extraction (ECCE) to phacoemulsification, with a focus on reducing complications associated with surgery, such as posterior capsular rupture. The study aims to investigate the micro and nanoscale structures of cataract lenses to enhance surgical techniques and outcomes [[1-2]].
Methodology: Klaas describes the methodology used to obtain cataract lenses during ECCE from patients. The lenses underwent a series of preparation steps for SEM analysis, including fixation, washing, dehydration, and coating. This rigorous methodology was carried out at the University of Erlangen under the supervision of Prof. Rohen [[4]].
Structural Findings: The findings reveal that the normal human lens has a concentric arrangement of lens fibers, crucial for its elasticity and ability to change shape. However, in cataract lenses, particularly in nuclear cataracts, considerable degeneration was noted, including broken fibers and gaps between the cortex and nucleus, which are indicative of significant structural changes due to aging and cataract formation [[5-6]].
Key Observations: The study identifies various regions within the lens, including the central part of the inner nucleus, the outer part of the cataract nucleus, and the equatorial region of the cortex-nucleus compartment. Each region exhibits distinct structural characteristics, such as lamellar arrangements and water clefts that may facilitate surgical interventions [[6-8]].
- The presence of weak connections among lens fibers suggests potential strategies for microsurgical procedures, particularly in separating the lens components during cataract surgery [[13-14]].
Implications for Surgery:The implications of these findings for cataract surgery are profound. Understanding the fine structural characteristics of the lens allows surgeons to utilize strategic advantages in their techniques. For instance, identifying predetermined breaking points within the lens can lead to more effective use of surgical tools like lasers, enhancing the safety and efficacy of procedures [[14]].
Conclusion:The study concludes that SEM analysis of nuclear cataract lenses provides critical insights into their structure and associated degenerative changes. These insights can inform the development of improved surgical techniques, emphasizing the principle that "form follows function" in the context of lens anatomy and cataract surgery [[14-15]].
In summary, Dr. Klaas's study underscores the importance of detailed structural analysis of cataract lenses in advancing surgical practices and minimizing complications, ultimately contributing to better patient outcomes in cataract surgeries
Scanning Electron Microscopic Study of Nuclear Cataract Lens
Introduction and Purpose
REM (scanning electron microscopy) can be used to analyze cataract lenses at the micro and nanoscale. Cataract lenses are opacified due to the aggregation of lens proteins, and these aggregates can be visualized and characterized using electron microscopy techniques.
REM can be used to visualize the surface of the cataract lens and observe the size and morphology of protein aggregates. It can also be used to examine the internal structure of the lens and the organization of the protein aggregates within the lens fibers.
Overall, REM analysis can provide valuable information on the structure and composition of cataract lenses, which can be useful in developing new treatments for cataracts.
Progressive nulear cataracts are associated with yellow to brown color of the lensnucleus and have often an only small area of the cortex as well as reduced space between the lens cortex and the lens capsule. The surgical procedure of these types of cataracts sometimes even today can be a challenge for residents and even experienced ocular surgeons.The changes in the ionic composition and the hardness of the nucleus with complete loss of elasticity and the reduced structure of the lensfibers as well as the increase of the thickness of the cataract lens are associated with severe loss of vision and leads often to difficulties during the surgical treatment. First description of alterations in the lens fibers by Kalariyaet al ., (4; Kalariya et al 1998) showed membrane ruptures, watervacuoles and multilammellar bodies. These alterations were absent in the anterior and posterior cortex.
(5; Kuruvilla et al IJIRMPS | Volume 6, Issue 5, 2018 ) found that the lammellar bodies were involved in the repair of ruptured membranes and breakdown of affected proteins.
Of special interest was to get more information of different compartiments of the cataractlens nucleus and also the fines tructure of the zonular region of the cortex area and behind.
Methology
The human cataractlens hardness degree 3-4 was obtained from a patient admitted for cataractsurgery. The surgeon decided not to operate with the phacoemulsificationmethod but standard ECCE. After large 6mm-7mm capsulorhexis the hydrodissection between capsule and cortex was performed. Thereafter the lens was removed though an enlarged corneaoscleral incision of 7.0 mm with help by viscoelastics.
In order to obtain lensfragments for SEM analysis the cataractlens further was split in smaller fragments with help of repeated hydrodissection (2; Klaas, DOG 1998/1991; ) All parts and fragments were washed and cleaned with BSS and immediately placed in 2.5% glutarealdehyd and the ITO-fixationmedium: Paraformaldehyd, Glutaraldehyd and Picrinacid, thereafter washing with Cacodylatpuffer and Osmiutetroxid for at least two hours, followed by again washing out, dehydration, six-step ethanol bath, Aceton, drying with CPD (Critical-point-procedure), coating with silver, and conformal goldcoating with a sputter coating machine to deposit a 100 Angstrom layer. The SEM - examination was done with the Cam Scan 4.DV Cambridge Inc. All Procedures and examination were done by Anatomie I University of Erlangen by Professor Dr. J. W. Rohen and his team.
Structure of the human lens
The structure of the human lens is well known. First we have the inner part of the lens with mainly three compartiments, the inner -embryonal- nucleus, the remaining nucleus which increases with age and the cortex, all inside the lenscapsule with inserting zonulafibers at the lens-aequator. during the development of the lens there are sutures similar to those at other organs.
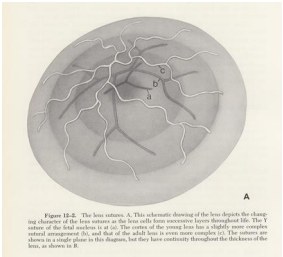
This schematic drawing of the lens depicts the change in character of the lens sutures as the lens form successive layers throughout life. During the growth of the lens, its embryonic lens nucleus remains alsmost unchanged, while the lamellar layers develop sutures, depending on their diameter, to stabilize the growth processes. All compartiments have well arranged sutures and have continuity throughout the whole thickness. (A)
fig. 1 Threedimensional model of the lens
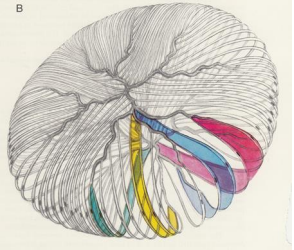
There are also symmetrically arranged bands or strings at the sutures visible and it is possible to fix them during surgery. These bands are so called weak lines -or intended break point- like breaks in swiss chocolate. (B)
fig. 2 Adult lens, complex anterior and posterior organisation of the lensfibers and sutures
Results
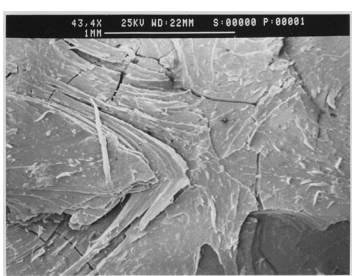
The finestructure of the normal human lens shows concentrical arranged lensfibers with radial composition one layer after the other. So the normal lens is perfect made for changing the form due to their elasticity. The SEM picture shows the arrangement of the lensfibers but between the fibers there are connections which strongly reduce the elasticity. Different layers are connected together which further will reduce the elasticity. We found no cortical swelling but degenerated fibers with large spaces between the remaining cortex and nucleus. As seen at the slitlamp -with the different coloured regions starting at the old embryonic central inner nucleus with dark brown colour decreasing up to the outer nucleus and cortex- we can see this analog to the SEM pictures.
One region was also from interest, the region of the lens-aequator. There we found insertions ore impressions from the zonularegion. Normally the zonuafibers inserts at the outer lenscapsule with some fibers getting through. The accomodation-therorie by Schachar postulated connections to the inner lens. Here we are able to show insertions -I would like to call them digiprints or impressions- at that region.
Possibly they are able to support some way of accomodation in interaction with forces from the zonulafibers to the lens-capsule.
The lamellar structure is visible also within all regions of the cataract-lens including the segmental arranged sutures. The increase of density towards the inner nucleus of the lens (but also the not rigid but rather loose intercellular cross-links, by which only a change of shape during accommodation is possible in the younger , more elastic lens), made it possible to induce a separation by targeted fluid injections into these layers, which on this basis should enable various microsurgical procedures.
Three different parts of the cataractlens could be examined:
1. central part of the inner nucleus
2. outer part of the cataractnucleus with epinucleus
3. aequatoreal region of the cortex-nucleus-compartiment
fig. 2 segmental structures - view through the operation microscope
Even the pie-piece-like and roseleaf-like segments visible after the sectoral structure, corresponding to the segmental structure often visible after the arrangement of the sutures, could be approached differently by microsurgery due to still existing so-called predetermined breaking points. Often we are able to see this structures during surgery as small vacuoles in segmental arranged manner.
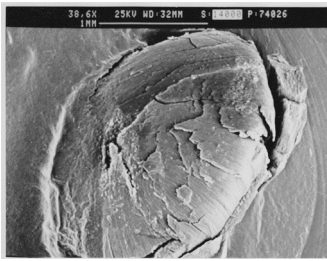
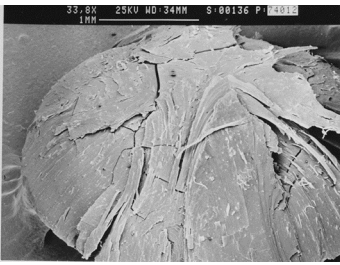
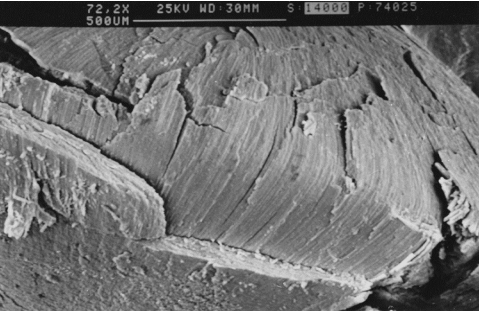
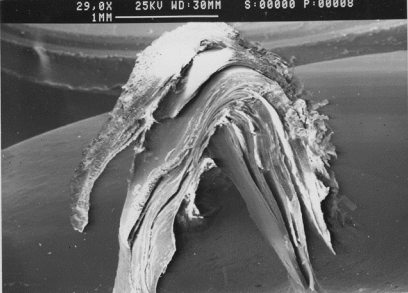
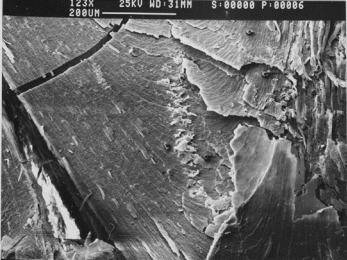
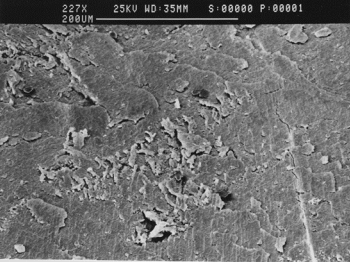
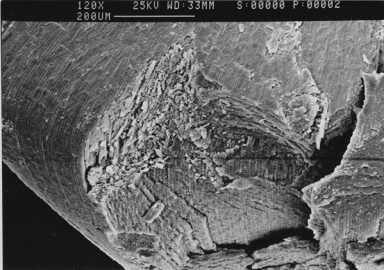
1. central part of the inner nucleus
fig. 3, fig 4 Inner Nucleus, lamellar structure
These embedded half nuclar parts show the typical lamellated bands of the lensfibers and broken region especially at the aequator.
In the degenerated region edge and groove patterns are visible.
The interfibrillare connections seem to be weaken, so that waterclefts in between showing the border of the different lens parts but also the harder inner part of the nucleus.
((This is important for us during surgery. The waterclefts as well as the border of different parts of density of the cataractlens will allows us special surgery options and strategies.))
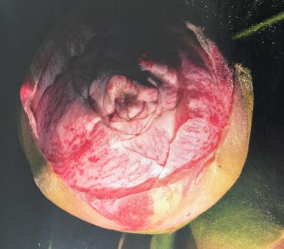
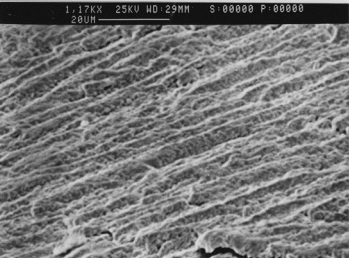
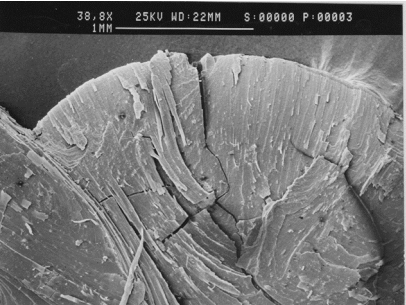
Fig 5: Inner Nucleus, lamellarconcentrical structure higher magnifacation with roseleaf similar composition of the concentrical lensfiberlayers.
Fig 6: lamellar roseleaf similar composition structure as an example in nature allows displacements of the slats
This embedded inner nuclear shows on the one hand the typicall lamellated bands of the lensfibers but also on the other hand a roseleaf-similar structure and threedimensional composition of the lensfibers itself. (fig 5)
So, in a way, we can already compare the fine structure of the lamellae of the lens with other examples from nature, for example a rose blossom. (fig 6)
These lamellar-structures (fig 7-10) allows movements to acchieve changes in its elasiticity. This finding is remarcable, because of its structure similar to roseflowers. This natural composition will allow in a more easy way to make changes in its three-dimensional form e.g. during the complicated process of accomodation.
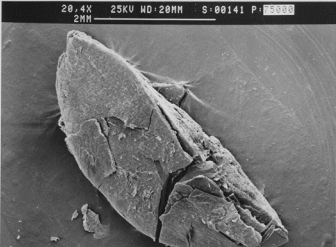
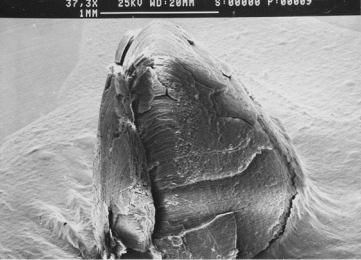
Fig 7: Smallest unit of the most inner part of the central lensnucleus with nearly no lensfibers structures due to the hardness of the cataractlens
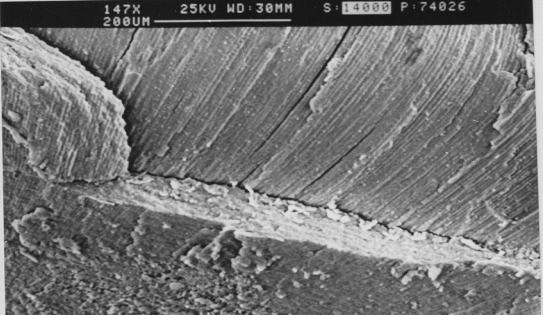
Fig 8: Second part of an embedded nucleus, Inner Nucleus with demarcation line at the nucleuspart with lower density, lamellar waterclefts, at the point of changes in densitry, concentrical structure , parallel arranged lensfibers concentrically to the center.
The sutures are only visible as small segmental arranged lines.
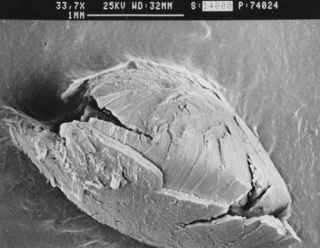
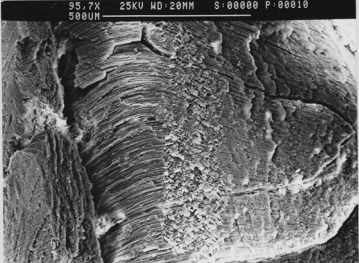
Fig 9: Higher magnification : Border between different parts of the outer nucleus, lamellar-concentrical structure with parallel lensfibers, numerous thin layers
Fig 10: Detail view: Higher magnification : Border between different parts of the outer nucleus, lamellar-concentrical structure with parallel lensfibers, numerous thin layers.
2. outer part of the cataract nucleus with epinucleus
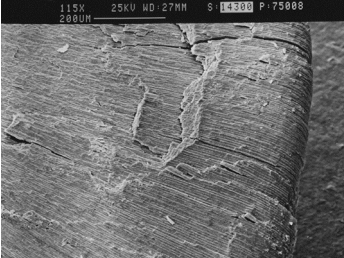
Fig 11, Fig 12
Again the epinucleus has similar lamellar structures with clearly visible concentric structure, whereby the embryonic core has a more homogeneous structure due to internal mineral deposits
Fig 13, Fig 14 lamellar structure, waterclefts, surgery relevant structures
Older fibres are internalised by the addition of younger nerve fibres at the equator this produces an age gradient of fibres within a single lens. (fig 13, 14)
According to Kalariyaet al., (1998) in the lens fibers three main age-related fine structural alterations were found membrane ruptures, water vacuoles and multilamellar bodies. The frequency of these alterations increased with age and they remained restricted to the superficial equatorial cortex and nucleus. The membrane ruptures and water vacuoles are in morphological support of the view, based on biochemical evidence,that oxidative stress leads to destabilization and disintegration of membranes and consequently disturbs the water balance of fibers. There is dissolution of the cortical cells (Fig.C3) and fragmentation and separation of the cortical region. Due to the nuclear swelling the cortical rupture and separation of fibres occurred. Nuclear area is well degenerated. Swollen disintegrated fibres in the equatorial region can be noticed.
3. aequatoreal region of the cortex-nucleus-compartiment
Fig 15, Fig 16
The outer part of the lens shows at the area of the lens capsules zonular region numerous knob-similar structures depending of the insertion points of the zonular fibers.
Fig 17, Fig 18, Fig 19
equatoreal region, insertion marking of the zonulafiber-prozesses
In addition there are structures visible who may well correspondend to insertion structures of zonula fibers that continue centrally under the lens capsule, as we can clearly see during some operations, these fibrous processes must be spared for the sake of stability of the posterior capsule. (fig 17-19). Large disinsertions of the zonules were present in noumerous eyes that had undergone extracapsular cataract extraction (ECCE)(8).
These insertions are immense important for the stability of the residual capsular bag after cataractsurgery. Within the inside of the capsular bag there exists fibers who are following the lamellar structures and may insert at the surface under beneath the capsule. In the normal lens a fibre to fibre arrangement and little interfibre spaces are peculiar to the lens morphology.
Degenerated subcapsular region with small vesicles and broken capsular region and in the posterior broken region elongated ribbon like lens fibres are present with numerous small vesicles on the surface.
Lamellated bands of lens fibers of different density with fine spaces and broken cortical region can be seen through cut surface due to the swelling of the nuclear region (fig 11-12).
Broken nuclear cataractous whole lens can be observed (fig 15-18). Arranged cortical fibres in the upper part and broken and separated lens fibers in the cut end (Fig.3b-2) with large vesicles or spherical masses of different shape and size are present on the surface of the lens fibres.
In the degenerated and disarranged nuclear region, edge and groove patterns are visible. The many compartment like arrangements of the cataract lens especially in nuclear cataracts (fig 13-14) are predefined structures that enable various operation options. So we are not expressed to find structures that we have often discovered by chance during eye operations: Clear separation of the individual lens nucleus compartments.
We are also not surprised to find structures e.g. the formation of fluidwaves between the lenscapsule and the lenscortex as well as the formation of the so-called golden ring, a sign of a clear separation of the individual lens nucleus compartments by fluid injections. These areas have no firm connections to the other core areas, whereas internally there are firmer connections between the individual lamellar lens fibrils, an essential prerequisite for the elasticity and special deformability of the lens with different curvature surfaces and different density gradients decreasing towards the cortex and lens capsule, in contrast to a rigid rubber-ball-like system. So the deformability of the lens is greater in the outer parts of the lens with regard to the ability of accomodation.
Fig 20: A.Grzybowski, R.A.Schachar lensdeformation during accomodation
The ability of deformation in the epinuleus- and cortex-region with its smoother consistence and absence of intercompartment connexions -in contrast to the interfiber-layer connexions - may be also one additional cause of the theory of accomodation by Schachar et al.(9). Additional investigations eg high resolution fotos from the inside of the capsular bag of the zonular region with help of the new microfiber-fotoequipment can be helpful .
Summary and Conclusion
SEM study of nuclear cataract lens obtained from a patient, who had ECCE surgical treatment instead of phacoemulsification, showed typical alterations of the fine structure of a cataract lens. The clear gaps between the individual parts of the nucleus were impressive, whereas the inner core of the lens appeared very compact dens and homogenous, its surface without any developed fine structure eg of lens fibers as in the others parts of the nucleus. Damage to the fiber cell membranes was noted in all regions of the nucleus. The most important damage occurred within undulating membrane junctions where the loss of membrane segments was common.
In the other two parts of the nucleus up to the so-called epinucleus, the typical lamellar structure of the lens fibers with sector-shaped demarcation were impressive- as it is often visible under the operating microscope- altered by vesicles or spherical masses of different shape and size present on the surface of the lens fibres. In the degenerated and disarranged nuclear region, edge and groove patterns are visible, also impressive fine structures in the zonular region. These impression-like structures within the equator region indicate a continuation of the zonula fiber-like finestructure into the lens equatoreal region.
In fact, such fine fibers are often seen intraoperatively.
Microsurgical interventions can be oriented to the basic anatomical structures, e.g. by utilizing strategic advantages through knowledge of the so-called predetermined breaking lines or breaking points by using ultrasound or laser energy more gently, especially in our nowadays available better Femtolaser-machines. The femtolaser patterns should be oriented to the so-called predetermined breaking points of the cataract lens, in order to be energetically oriented in the sense of a gentle surgical technique. In this way, we can also apply the basic principles of scientific laws here:
Form Follows Function - Function Follows Form
Acknowledgement: I would like to thank Prof Dr Johannes W. Rohen in Marburg 1970 for his many years of support and professional exchange posthumously with this paper.
Please click here to view article with complete figures
References
1. A Y Anis; Understanding Hydrodelineation: the term and the procedure Doc Ophthalmol1994;87(2):123-37. doi: 10.1007/BF01204789.
(2) Dieter W. Klaas: Aquadissectio alia post aliam. A helpful technique in the fractionated preparation of the lens nucleus in extra capsular cataract extraction.: Fortschritte Ophthalmologie 1990;
DOG presentation 1989 PMID2210578 [PubMed - indexed for MEDLINE]
(3) Douglas D. Koch, John F Liu : Multilamellar hydrodissection in phacoemulsification and planned extra capsular surgery JSCRS Vol 16, % 1990, pg 559-562
(4) Kalariya N., RawalUM.,Vasavada AR (1998). Human lens epithelial layer in cortical cataract.In J Opthalmol.46(3): 159-162
(5) Kuruvilla et al IJIRMPS | Volume 6, Issue 5, 2018
(6) Gimbel HV. Hydrodissection and Hydrodelineation Int Ophthalmol Clin. 1994 Spring;34(2):73-90. doi: 10.1097/00004397-199403420-00006.
(7) Brint SF, Blaydes JE, Bloomberg L, Crozafon P, Fine IH, Kraff MC, Filippelli J, Hoffman J.: initial experience with the hydrosonics instrument to soften cataracts before phacoemulsification
J Cataract Refract Surg. 1992 Mar;18(2):130-5. doi: 10.1016/s0886-3350(13)80918-2.
(8) D J Wilson, M J Jaeger, W R Green: Effects of extracapsular cataract extraction on the lens zonules ; 1987 May;94(5):467-70. doi: 10.1016/s0161-6420(87)33423-2.
(9) A.Grzybowski, R.A.Schachar et al - Int J Ophthalmol, Vol. 12, No. 11, Nov.18, 2019.